
Abstract
Background:
The safety and feasibility of using kinesiotape as a short-term alternative treatment to compression garments or gloves for hand lymphedema have not been examined. The aim of this study was to examine if kinesiotape could maintain size and extracellular fluid (ECF) volume of the hand and forearm, as well as upper limb function and quality of life for women with secondary hand lymphedema.
Methods and Results:
Six women with secondary hand lymphedema underwent pretreatment measurements, including hand and digit size using a tape measure; ECF volume using bioimpedance spectroscopy; and patient-reported outcome measurements of upper limb function and quality of life. Kinesiotape was then applied to the dorsum of the hand and left for 48 h, during which participants were asked not to wear compression garments. Posttreatment measurements were completed after kinesiotape removal. Changes in measurements were compared to the smallest detectable change (SDC). Hand size did not change more than the SDC; however, a single affected digit increased in circumference by more than the SDC. Changes of the whole arm ECF volume were less than the SDC. The ECF volume of the dorsum of the hand increased in one and decreased in another participant. The forearm ECF volume decreased in two participants. Upper limb function and quality of life did not change. No adverse event was reported.
Conclusion:
Short-term kinesiotape use appears to be safe in maintaining the physical presentation of hand lymphedema. However, these results should be examined in a larger sample. The feasibility of using kinesiotape as an alternative treatment to compression requires further investigation.
Clinical Trial Registration number:
ACTRN12618001232224p, July 23, 2018 retrospectively registered.
Introduction
Secondary hand lymphedema is a permanent swelling that may manifest as an increase in hand size, present in the whole hand or localized to a region such as the dorsum of the hand or digits, 1 affecting ∼37% of individuals with secondary upper limb lymphedema. 2 Persistent hand swelling can affect the range of motion and function of the hand,3,4 which may negatively impact the ability to perform activities of daily living and quality of life.5,6
Compression garments or gloves are the main treatment used for secondary upper limb and hand lymphedema1,7; however, compression is not always well tolerated, nor practical to wear. Thirty percent of individuals who were prescribed a garment or glove, did not follow the advice to wear them, reportedly due mainly to discomfort. 8 Individuals who wear a compression garment or glove also report their skin being hot and/or itchy under the garment. 9 In addition, persons with hand lymphedema may not be able to wear their compression garment in all situations, for instance, when working or in situations where the garment could be wet or soiled. 1 Alternative treatments to compression garments or gloves that could overcome these barriers are required.
Kinesiotape is an elastic cotton tape10–12 that is applied to the skin and can be worn in wet or humid conditions.13,14 It purports to lift the skin, opening the initial lymphatic capillaries,10,11,15 which may improve the movement of fluid into the lymphatic system. 16 While kinesiotape may not necessarily improve hand swelling, similar to compression garments and gloves, 13 kinesiotape may assist with maintenance or reduction of swelling17–20 when a compression garment cannot be worn.
However, the safety and feasibility of using kinesiotape to maintain the size of the hand and digits in hand lymphedema have not been examined. The aim of this study, therefore, was to determine the safety and feasibility of a kinesiotape application to maintain the size of the hand and digits, and the volume of extracellular fluid (ECF) of the hand, forearm and whole arm, as well as upper limb function, symptoms, and quality of life.
Materials and Methods
Ethics approval was obtained from the Human Research Ethics Committee of The University of Sydney and Clinical Trial Governance (2018/666). All participants provided written, informed consent before participation in the study.
Participants
Potential participants were recruited from a private lymphedema clinic in New South Wales or through social media. Eligible participants were those who had secondary hand lymphedema, had completed cancer-related treatments except for hormone-related treatments, at least 6 months previously, and did not undertake active lymphedema treatment at least 1 month before participation. Furthermore, participants had to be able to communicate and comprehend English language and be willing to not wear their compression garment or glove for 2 days.
Potential participants were excluded if they had an infection or condition that might lead to swelling (heart or kidney disease, pregnancy), or were taking medication affecting the volume of body fluid. They were also excluded if they had a pacemaker or in-dwelling defibrillator, an irremovable bracelet or ring, skin conditions, wounds, infections, or an allergy to kinesiotape material. A small kinesiotape piece was mailed to potential participants who were asked to apply it to the dorsum of the unaffected hand for 24 h; only those who did not react to the tape were invited into the study.
Kinesiotape application
In consultation with four clinical lymphedema experts in New South Wales, Australia, a standardized kinesiotape application was determined and a garment removal period of 2 days (48 h) was determined to be safe.
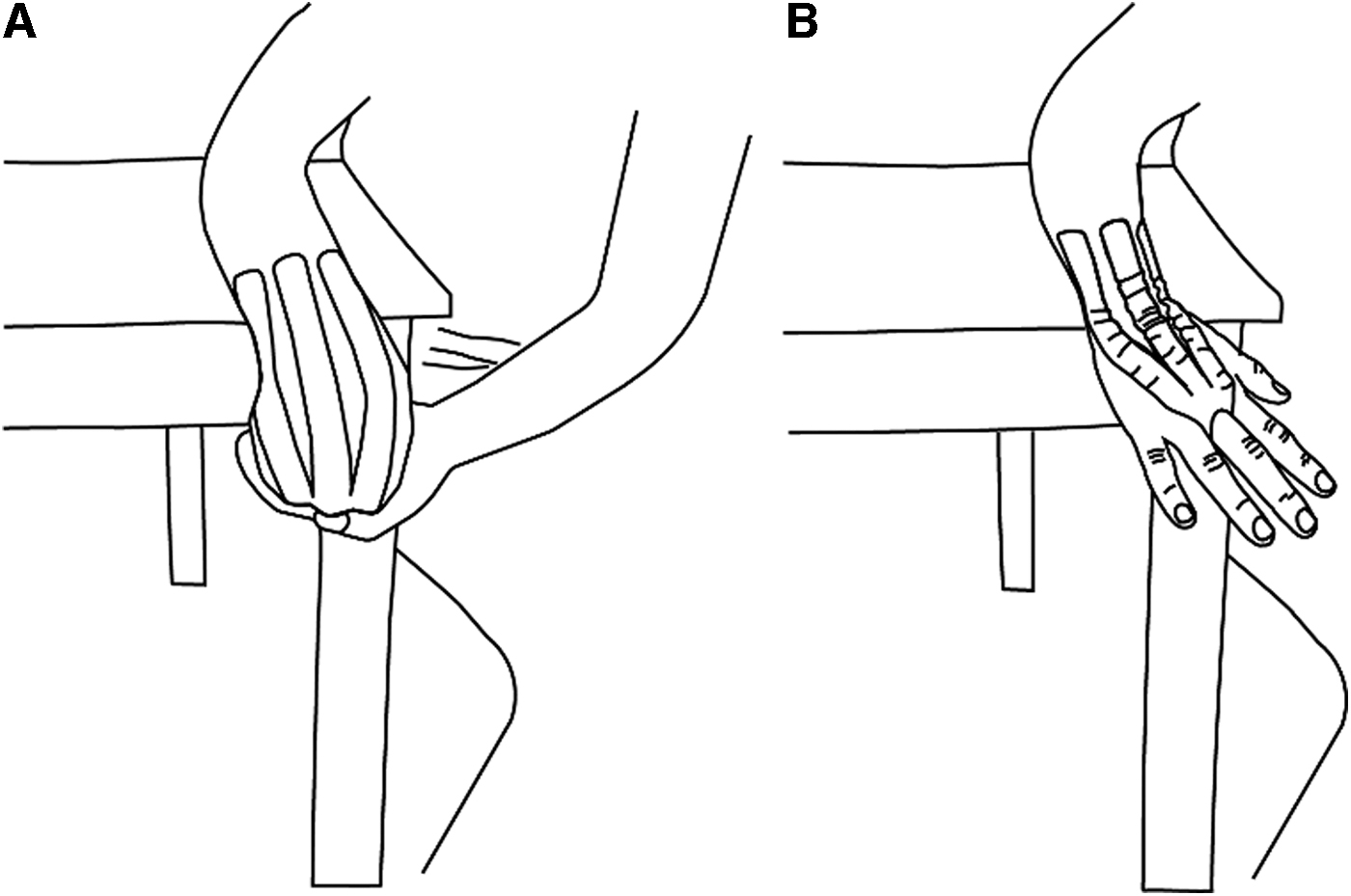
The kinesiotape was applied to participants sitting with their forearm resting on a table and wrist and digits in maximum flexion (Fig. 1A). The wrist was positioned with ulnar deviation to apply the medial tail of the tape and radial deviation to apply the lateral tail. A tension of 15%–25% of the maximum tension of the kinesiotape was applied to the tape, which was then applied to the skin from the palm to the dorsum of the hand to create wrinkling of the skin when the wrist and fingers moved into extension (Fig. 1B).
Participants were asked not to remove the kinesiotape unless they had a skin reaction and were provided with instructions on how to remove the tape if this occurred. They were instructed to maintain their standard lymphedema care routines, excepting garment usage. A research team member contacted the participants 24 h after the kinesiotape application to check on their skin response.
Assessments
Participants attended two face-to-face sessions, 48 h apart. Participants who wore a compression garment or glove were asked to remove it 2 h before the pretreatment assessment. All assessments were undertaken at both the pretreatment and posttreatment sessions.
Size of the hand and digits
Measurements of the body of the hand, using a figure of eight technique, 21 and the size of the digits at the level of the medial phalanx were undertaken with a nonelastic ribbon rather than a tape measure. The tension applied to the ribbon was standardized by a small weight tied to an end of the ribbon that was left hanging off a table. For measurement of the body of the hand, the elbow was flexed to 90° and supported on a table, wrist in a neutral position, fingers adducted and extended, and thumb abducted in the plane of the hand (Fig. 2A).
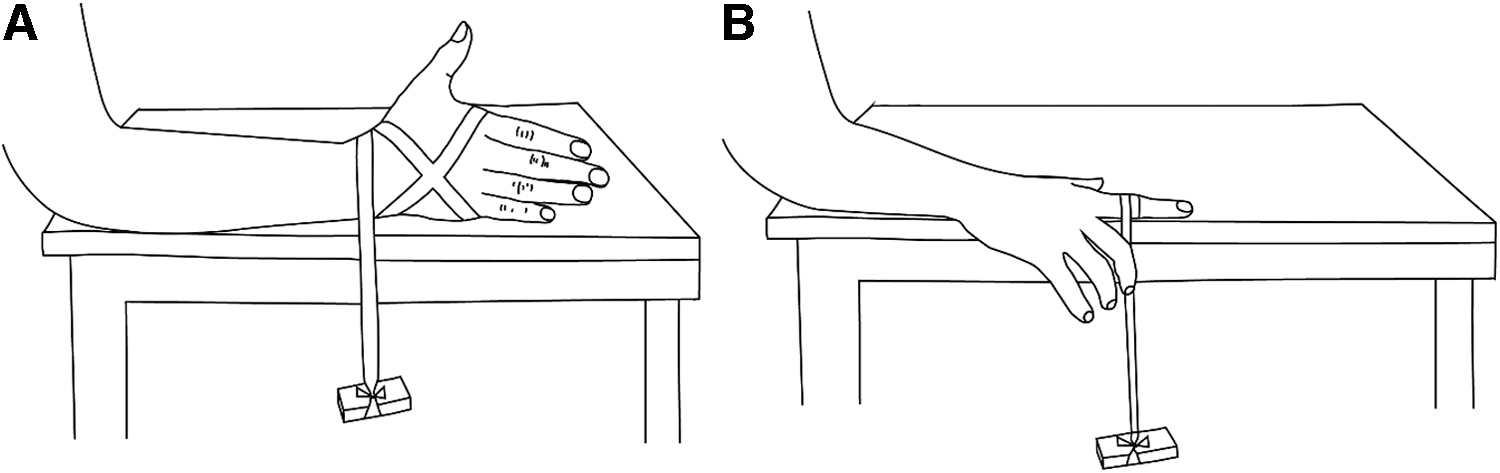
For measurement of the digits, the hand was positioned in pronation, wrist in a neutral position, with all digits relaxed in abduction and extension, leaving the digit to be measured aligned with the edge of the table (Fig. 2B). The nonelastic ribbon improved the standardization of the measurement locations and blinding of the researcher. The right hand was assessed first in all participants.
Volume of ECF
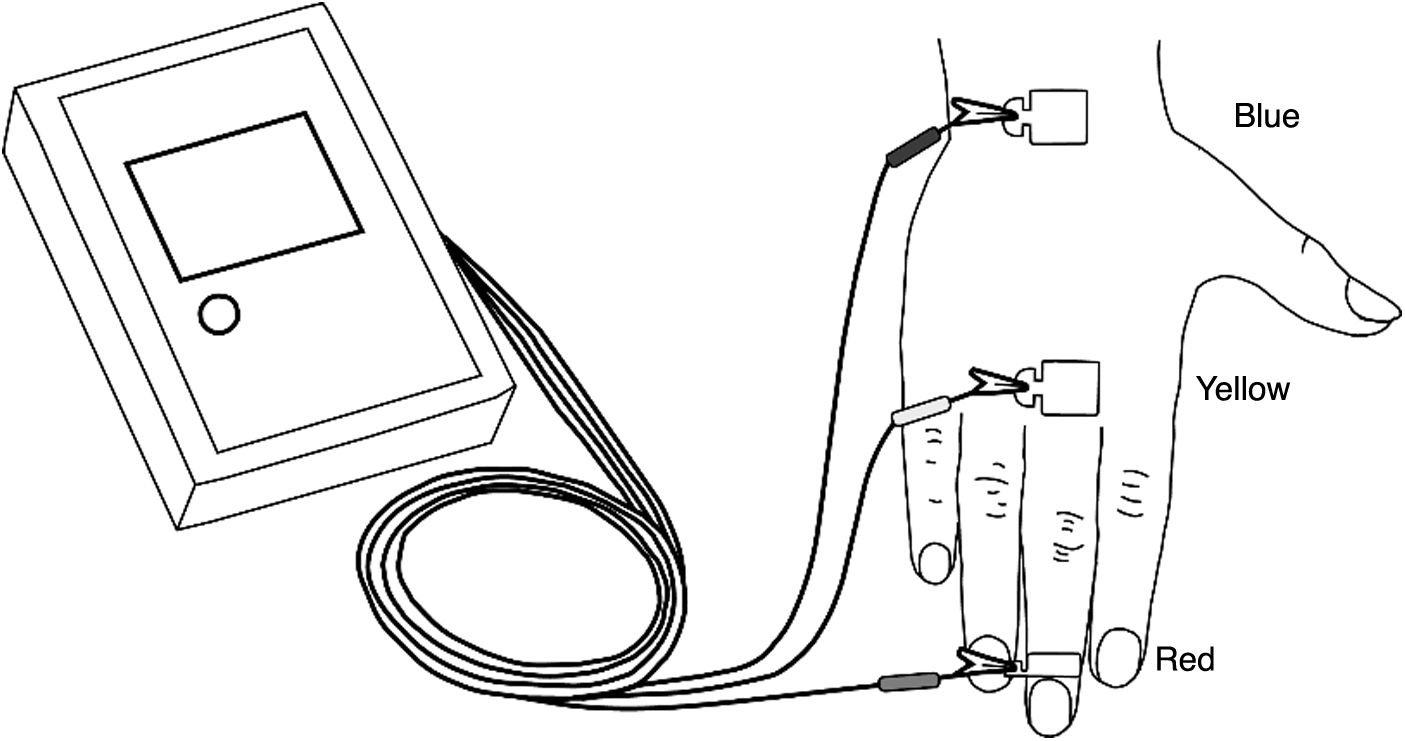
Measurements of impedance of the whole arm, the dorsum of the hand, and a 10-centimeter segment of the forearm that commenced at the ulnar styloid were obtained using a bioimpedance spectroscopy (BIS) device (SFB7; Impedimed Ltd., Brisbane, Australia). Impedance at zero frequency was determined for both hands, forearms and whole arms, and the interlimb ratios between the same regions were calculated. All measurements were taken with the participant resting in supine with the hands relaxed in pronation, for at least 5 min.
Gel electrodes were placed on the participant's right foot and on both hands as per the standard protocol (Fig. 3).22,23 Impedance values at zero resistance (R0), which reflects ECF volumes, were obtained by processing BIS files using the manufacturer's software (Bioimp v.5.4.0.3; Impedimed Ltd.) for each participant file. The impedance values of both hands, forearms and whole arms, allowed determining the ratios between the same regions calculated as the impedance of the unaffected side divided by that of the affected side.
Participant-reported response and satisfaction with kinesiotape
A set of questions was used to assess participants' response and satisfaction with kinesiotape, including skin conditions, pain or altered sensation, detachment of the tape, and satisfaction with kinesiotape.
Tissue compliance
Tissue compliance was assessed using a pitting test, 24 at the participant's perceived most swollen spot in the dorsum of the hand. Pressure was applied with the researcher's thumb for 60 s. The presence or absence of an indentation was recorded upon pressure released.
Lymphedema severity and perception
Lymphedema severity was assessed using the Norman questionnaire, 25 which indicates self-determined severity as mild, moderate, or severe. Lymphedema perception was evaluated using a set of questions to identify the area of greatest swelling, the magnitude of swelling, and fibrosis, which was rated using a 10 cm visual analog scale. Participants also rated their perception of the level of concern about their hand lymphedema and the effectiveness of compression garments or gloves.
Participant-reported upper limb function and quality of life
Upper limb function and quality of life were assessed by the Lymphedema Quality of life of the limbs (LYMQOL) 26 modified for the hand. Participants completed this questionnaire using an online survey Qualtrics; when it was not possible, participants completed it on paper (n = 3).
Data analysis
The smallest detectable change (SDC) was used to interpret the changes in the size of the hand and digits, as well as ECF volume after the kinesiotape application. The SDC is the smallest amount of change above the threshold of error in the measurement that is indicative of a true change. 27 SDC values were calculated as 1.96 × √2 × standard error of the measurement (SEM). 28 Changes in tape or BIS ratio measurements outside their SDC values are indicative of a true increase or decrease in size or ECF volume, respectively.
The SEM used to calculate SDC of the figure of eight measurements was 7.1 mm, 29 and the 1 mm SEM reported for circumference measurements of the little finger 30 was used to calculate SDC for circumference measurements of all digits. The SEM values used to calculate SDC values for BIS ratio measurements was 0.06 interlimb ratio for the whole arm, 31 and 0.03 interhand or interforearm ratio for the hand and forearm. 32
Participant-reported responses to kinesiotape were recorded after the application, including whether detachment of the tape occurred, and if yes, where. Satisfaction with kinesiotape was rated on a 0–10 scale, with values from 0 to 5 considered generally unsatisfied to very unsatisfied, and from 5 to 10 considered generally satisfied to very satisfied.
For participant-reported upper limb function and quality of life, the SDC values of 2.9, 4.7, 9.0, and 4.0, were used for interpretation of LYMQOL subscale scores in the domains of function, appearance, symptom, and mood, respectively. 33
Results
Six female participants, between 41 and 69 years of age, completed the study. Participant characteristics are summarized in Table 1.
Participants' Demographic and Lymphedema Characteristics
BMI, body mass index; NA, not applicable.
Size of the hand and digits
Objective outcomes using the figure of eight technique and circumferences of the digits, before and after kinesiotape application, are presented in Table 2. For both the affected and unaffected side of all participants, the change in size between before and after the application was within the SDC of 20 mm for the figure of eight technique. Change in 6 out of 60 circumference measurements of the digits exceeded the SDC of 3 mm; only three of them were on the affected side, with two decreasing by more than the SDC. Only one measurement was an increase more than the SDC in the circumference of the affected thumb.
Change from Pretreatment to Posttreatment in Circumference Measurements, Bioimpedance Spectroscopy Ratios, and Quality of Life After Kinesiotape Application
Changes outside the SDC of 20 mm for the figure of eight, 27 3 mm for the digits 28 ; 0.166 interlimb ratio for the whole arm 29 and 0.08 interhand or forearm ratio for the hand and forearm, 30 or 2.9, 4.7, 9.0, and 4.0 for function, appearance, symptom, and mood domains of LYMQOL, respectively. 31 Scores on each domain range from 0 to 10, with higher scores indicating worse quality of life; Negative values indicate decreases in scores; Overall QoL: Overall quality of life score that ranges from 0 to 10, with values indicating poor and excellent quality of life, respectively.
—, missing data; BIS, bioimpedance spectroscopy; LYMQOL, Lymphedema Quality of Life of the limbs questionnaire; QoL, quality of life; SDC, smallest detectable change.
Volume of ECF
The impedance of the whole arm, dorsum of the hand, and initial 10-cm segment of the forearm were assessed in three participants (Table 2). There were missing data of impedance measurements for the other three participants due to technical difficulties with the BIS device. The whole arm interlimb ratios did not exceed the SDC of 0.166 interlimb ratio in any of the participants. However, changes outside the reported SDC of 0.08 for interhand and interforearm ratios were found. The interhand ratio increased in one participant and decreased in another participant. The interforearm ratio decreased in two participants, suggesting a reduction in the volume of ECF in the initial 10-cm segment of the forearm.
Participant-reported response and satisfaction with kinesiotape
No adverse event or skin condition was reported after the kinesiotape application (Table 3). However, one participant reported a feeling of increased edema in the fingers. The tape remained in place in all participants, although five participants reported detachment of kinesiotape at the palm. Five participants rated their satisfaction with kinesiotape treatment at ≥5/10, indicating that they were generally satisfied to very satisfied.
Perceptions of Hand Lymphedema Before and After Kinesiotape Intervention and Satisfaction with Kinesiotape
Evaluated using visual analog scale.
Lymphedema perception and severity
All participants perceived the hand lymphedema to be less concerning after the intervention (Table 3). Four participants reported no change in their self-determined severity, region perceived with greatest swelling or fibrosis after the intervention (Table 3). Four participants also reported a decrease in the perceived swelling at the dorsum, one reported an increase in swelling, and the other one reported no change. Of those who reported changes in fibrosis, one had an increased perception of fibrosis and the other one a decrease in it. No change occurred in pitting edema.
Participant-reported upper limb function and quality of life
Participants' upper limb function and quality of life assessed by the LYMQOL did not change after the kinesiotape application (Table 2). No change for any participant on the subscales were outside the SDC values reported of 2.9, 4.7, 9.0, and 4.0 for function, appearance, symptom, and mood 33 respectively.
Discussion
Kinesiotape, used in place of a compression garment for 2 days, resulted in no change in the objectively measured size of the hand and digits or the ECF volume of the whole limb in the affected side. However, an increase in the ECF volume at the dorsum of the hand in one participant was noted. Furthermore, participants did not report a change in upper limb function or quality of life in 2 days without wearing a garment.
Our kinesiotape application protocol appeared to demonstrate its safety in multiple ways. A 48-h application of kinesiotape resulted in no report of adverse events. In addition, no potential participant had to be excluded due to skin reaction to kinesiotape before participating in the study. Furthermore, only minimal changes were observed in the size of the body of the hand or digits. Notably only one circumference measurement increased on the affected side by more that the SDC and this was for a thumb. The SDC value of 3 mm, used for all circumferences of the digits, was calculated from the SEM of the little finger 30 as this has been only reported SEM for a digit measurement.
However, the SEM of the little finger could be expected to be smaller than the SEM, which might be determined for the other digits, such as the thumb. The increase in the circumference of the thumb, therefore, may be still within the normal variance. There was more variability in the BIS assessment; however, it is not known what a normal fluctuation of ECF in the hand and forearm is. While normative variability in whole arm interlimb impedance ratio has been previously demonstrated, 34 it is unknown what is construed as normal fluctuation for the hand and forearm. In addition, it is unknown what the impact to swelling within the forearm when specifically treating the hand is.
Whether with a larger sample, or a longer treatment period, treating only the hand would continue to lead to stable ECF outcomes in the whole arm or ECF volume decreases in the forearm is unknown and requires further investigation. Future interventions for hand lymphedema using kinesiotape could explore treatment protocols that could reduce detachment of the tape from the skin, the use of kinesiotape in conjunction with arm compression sleeves, or the impact of kinesiotape on different hand lymphedema presentation and severity. While kinesiotape appeared to be a safe short-term treatment for hand lymphedema, the feasibility of its use is less clear.
The feasibility of using kinesiotape for hand lymphedema in place of compression garments or gloves needs further exploration. Initially, this study was proposed as an efficacy trial with a calculated sample size of 32; however, this sample size was not met, despite many attempts to increase recruitment. There may be two potential explanations for this. First, the incidence of secondary hand lymphedema may be overestimated; the only reported incidence of hand lymphedema of 37% is based on a self-report. 2 Second, the removal of garments or gloves for 2 days, although deemed safe by clinical experts, may be fear-inducing in individuals with hand lymphedema, who worry that without their garment, the swelling will worsen. 8
Two potential participants declined to participate because they felt uncomfortable with the idea of having the garment or glove removed. Future studies on treatments for hand lymphedema, apart from compression, may need to consider whether their treatment is acceptable to individuals, as this will impact the feasibility of intervention trials. Multicenter studies that could investigate hand lymphedema incidence and feasibility may help to address challenges with recruitment.
Evidence to support the assessment and treatment for secondary hand lymphedema is lacking. A range of reliable and valid assessments tools and measurement methods with reported SEM values for determination of measurement error 35 are available to objectively quantify the size, volume, or ECF volume of the hand in secondary hand lymphedema. However, information regarding the minimal important change (MIC) for most of these tools and methods is lacking and therefore limits their use. In this study, the reported SEM values allowed us to calculate SDC values for each assessment tool or measurement method, from which changes outside were considered true increases or decreases; however, MIC values would aid in determining whether observed changes would be considered clinically important to patients or to indicate a change in their management. 36
Furthermore, patient-reported outcome assessments to evaluate the impact of secondary hand lymphedema are required. The LYMQOL questionnaire, 26 used to assess the quality of life of the study participants, was modified from its original focus on the arm to include questions specific to the hand. The influence of these changes on its reliability is unknown. Patient-reported assessments that focus specifically on the impact of hand lymphedema, including on symptoms, function, and quality of life, will assist in differentiating the impact of lymphedema within the arm from that within the hand.
Conclusions
Kinesiotape, worn for 48 h in place of a compression garment in women with secondary hand lymphedema, appears to be safe in maintaining the size of the hand and digits, as well as the whole limb ECF volume. No adverse event was reported with the use of kinesiotape. However, these results should be examined in a larger sample. The effect of kinesiotape in longer-term use and how interested patients are in using it, as an alternative to compression, requires further investigation. Changes in ECF volumes at the dorsum of the hand and forearm as a result of kinesiotape treatment also require further investigation.
Footnotes
Acknowledgment
C.L. would like to thank the National Agency of Research and Development (ANID), Chile, for the funding provided.
Author Disclosure Statement
The authors have nothing to declare and reported no conflict of interests.
Funding Information
C.L. was supported by the National Agency of Research and Development (ANID)/Scholarship Program/MAGISTER EN EL EXTRANJERO BECAS CHILE/2017—73180204. The funder played no role in the design, conduct, or reporting of this study.