
Abstract
Background:
Breast lymphedema after breast cancer is challenging to quantify. Three-dimensional (3D) surface imaging is one available technique to measure breast volume, however, the measurement properties of available software programs have not been fully determined. The aim of this study was to determine equivalency of measurements with two software programs as well as reliability, standard error of measurement (SEM), and smallest detectable change (SDC).
Methods and Results:
Retrospective three-dimensional surface imaging (3D-SI) of 100 breasts taken before or after breast conserving surgery for breast cancer were retrieved for reliability analysis. Three assessors followed a standardized measurement technique using two software programs, Vectra® 3D Analysis Module (VAM) and Breast Sculptor®. Mean breast volume was 489.9 ± 206 cc using VAM and 480.1 ± 229.1 cc using Breast Sculptor. Lin's concordance showed poor agreement between programs (0.81–0.88). Measurements using VAM had excellent intra- and inter-rater reliability with SEM = 4.1% for one assessor and 8.7% for multiple assessors. Breast Sculptor also had excellent intra-rater and substantial inter-rater reliability but the SEM was much larger at 14.5% (intra-rater) and 19.1% (inter-rater). The SDC value was lowest for VAM and a single rater with 56 cc indicating a meaningful change beyond measurement error.
Conclusion:
Breast volume measurements captured with 3D-SI using VECTRA-XT are highly reliable, but the volumes, SEM, and SDC varied between the two software programs. Measurement error was lowest with VAM software. Although the usefulness of VECTRA-XT and VAM software to detect change in breast volume is promising, further solutions to reduce measurement error are required to improve clinical utility to measure breast lymphedema.
Introduction
Breast lymphedema can arise as a painful and distressing complication from the conservative treatment of breast cancer. However, there is no current consensus on how best to assess breast lymphedema. 1 Breast volume measurement is used to assess cosmetic outcomes from conservative breast cancer surgery and radiotherapy and may also be useful in assessing breast lymphedema.2–4 Accurate measurement of breast volume, however, is challenging. Unlike measurement of limb volume, it is difficult to reliably identify the breast border as there are no obvious anatomical landmarks at the superior and lateral breast regions.
Furthermore, as the chest wall is not visible, interpolation of this convex surface is required to calculate volume. 5 Three-dimensional surface imaging (3D-SI) is one possible approach to measure breast volume and to quantify breast lymphedema and has been previously used in breast cancer populations 6 and to measure limb lymphedema. 7 This measurement approach could be used to monitor breast lymphedema changes over time and determine the efficacy of breast lymphedema treatments.
3D-SI captures 3D images of the breast using multiple cameras. 5 The assessor identifies the borders of the breast on the 3D image and the curvature of the chest wall is simulated by an algorithm to complete the breast shape.5,8 Advantages of 3D-SI over other approaches are that it is quick to perform and causes minimal patient discomfort while also correlating strongly with mastectomy specimen volume as well as breast volume measured using MRI.6,8–12 One 3D-SI device, VECTRA®-XT (Canfield Sci, New Jersey), uses two software programs, VECTRA® 3D Analysis Module (VAM), which requires manual breast border selection, and Breast Sculptor® (Canfield Sci), which uses an automated program to designate the breast border from landmark points, to quantify breast volume.
The validity and reliability of these software programs have been determined separately, but never directly compared. For instance, breast volume quantified by VAM software was validated against the water displacement method using a phantom model on a flat board with a mean relative difference between these methods of 2.2% to 2.3% (limits of agreement [LOA] = −0.4% to 5.0%). 13 VAM software has demonstrated low coefficient of variation in two studies13,14 and excellent inter-rater reliability (intraclass correlation coefficient [ICC] = 0.991), with a mean difference of 1.73 cm3 (LOA = −56.9 to 60.3 cm3) between assessors in a third study. 12
The accuracy of Breast Sculptor software has been assessed against resected mastectomy volume and compared with other software programs, showing a lot of variability in the measurement error. 15 However, the reliability of the Breast Sculptor software has not been investigated, nor has the reliability of the two software programs been compared in a single population. Furthermore, it is unknown what is the measurement error associated with these two applications, and lastly, what is the smallest detectable change (SDC) for these software programs. Without this knowledge, what constitutes a real breast volume change beyond measurement error is unknown.
The aims of this study were, therefore, to (1) determine the extent to which breast volumes quantified by the two software programs are equivalent and (2) determine the reliability, measurement error, and SDC for each software program to explore which is more reproducible.
Materials and Methods
Study design
Previously acquired VECTRA-XT images were used to determine the level of reliability and measurement error of quantification of breast volumes using two software programs. Ethical approval was received by the human research and ethics committee of Western Sydney Local Health District (Ethics reference: 2020/ETH00059, Governance reference: 2020/STE00267).
Sample size calculation
A sample of 100 breast images measured once by three assessors and twice by one assessor was determined to be sufficient for determination of intra- and inter-rater reliability for an ICC of 0.8% and confidence interval (95% CI) ±0.1. 16
Participants
VECTRA-XT 3D surface images taken between 2018 and 2019 as part of routine clinical practice by nursing staff trained to use VECTRA-XT were retrieved for this study. Before capturing each image, the clinical protocol specified marking body landmarks using an indelible pen on the following: suprasternal notch, bilateral marks on the clavicle 7 cm from the suprasternal notch, the medial mammary margin, and the lateral mammary margin at the junction with the anterior axillary line. Women stood on floor markers to standardize positioning in relation to the 3D camera, with their arms extended at 45° shoulder abduction.
Nursing staff adjusted the position of women to align the nipples and anterior axillary line with the guidelines on the VECTRA-XT capture program and supported the women with one hand positioned on the hip to reduce movement during image capture. All images were taken in one clinic room using the same VECTRA-XT device.
A clinical staff member (C.S.) not involved in the assessment of images retrieved images taken either before any surgery for breast cancer or after breast conserving surgery with or without reduction mammoplasty and included women irrespective of body mass index (BMI) or breast size. Images were excluded if the women had undergone autologous or implant reconstruction. Demographic information was extracted from medical records (by C.S.) including age at the time of image capture, operated side, and history of radiotherapy and/or chemotherapy treatment at the time the image was taken. The images were then deidentified and saved for analysis.
Before volume analysis, breast images were excluded by one assessor (N.F.) if the degree of ptosis was 3 (i.e., nipple below the level of the inferior mammary fold) 17 or if the inferior mammary fold could not be visualized on the image from any view due to the position of the breast. These factors have been reported to potentially impact on the ability of the software to accurately create the chest wall and, therefore, accurately measure breast volume. 18
Volume measurement protocol and training
A standardized measurement procedure, based on the protocol by O'Connell et al. 13 and standard clinical practice at Westmead Hospital, was developed and followed. Before data extraction, three training sessions on the use of both software programs were completed to train three novice assessors. All assessors then practiced the volume calculation procedure using 10 individual breast images. Templates of the breast border for VAM and landmarks for Breast Sculptor were also developed and referenced during the assessment process (Fig. 1a). After training, each assessor independently quantified breast volume using the standardized procedures outlined hereunder. For each image, VAM software was first used followed by Breast Sculptor.

Breast border template.
Measurement of volume technique
VAM software
VAM software required the assessor to manually outline the region of interest. To facilitate this process, a grid was positioned over the image of the thorax with the y axis midline at the level of the suprasternal notch and the z axis aligned with the pen mark at the anterior axillary line. The region of interest was selected for each breast separately using the lasso function. As depicted in Figure 2, a horizontal line at the level of one grid square (2 cm) below the suprasternal notch ran across and then curved to follow the rim of the glenoid humeral cavity/delto-pectoral groove to meet with the anterior axillary line at the z gridline.
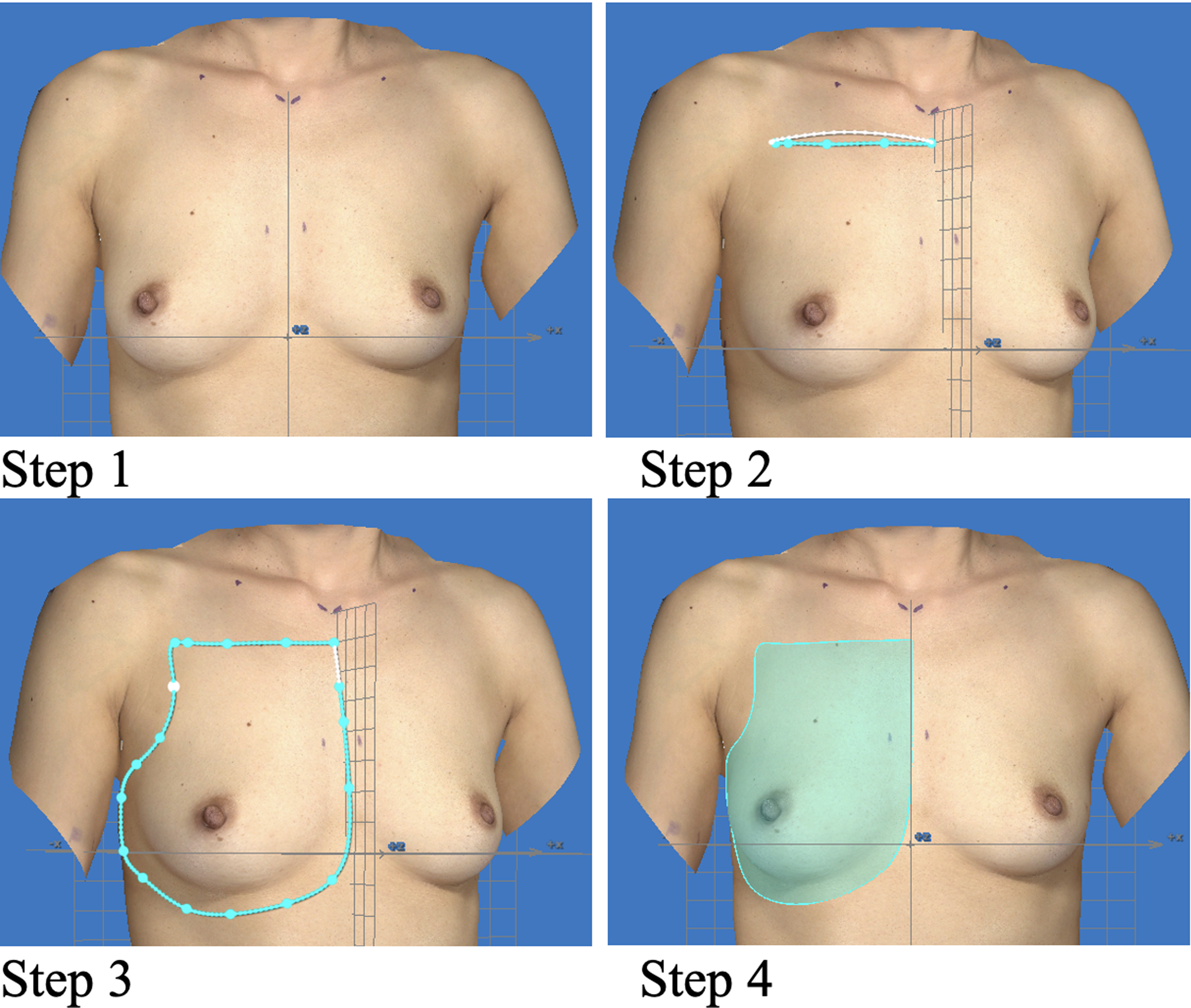
VAM breast border selection procedure. VAM, VECTRA® 3D Analysis Module.
The line was continued vertically down the anterior axillary line to the level one grid square below the lower contour of the breast and then followed the lower curve of the breast horizontally, maintaining a one grid square distance to the chest midline (y axis). Lastly, the line was extended vertically up the midline y axis to meet the starting point below the suprasternal notch. The interpolating surface was created, and the volume of selected breast area was calculated using the measure function. This procedure was repeated for the opposite breast.
Breast Sculptor software
Breast Sculptor software was an automated process in which both breasts were assessed at the same time (Fig. 1b). Landmark points were automatically positioned on each breast at the following landmarks: inframammary fold, nipple, areola, lateral mammary margin, medial mammary margin, suprasternal notch, and midclavicle. The positions of these landmark points were adjusted to match the marks that had been marked by nursing staff at the time of the image at the suprasternal notch, bilateral clavicle, medial mammary, and lateral mammary margins. The assessment function was used to calculate volume in both breasts.
All images were saved once the region of interest (VAM) or landmark points (Breast Sculptor) were selected, and volume calculation displayed on the image for data checking. Study data were collected and managed using REDCap electronic data capture tools.19,20 All assessors were blinded to the results of the other assessors or results from the first assessment for the repeated measured by the same assessors. Volume measures were calculated for images in VAM and Breast Sculptor programs using the same computer.
Data analysis
Descriptive statistics were used for participant characteristics and breast volume results using mean and 95% CIs, and breast cancer treatments were reported as frequencies and percentages (Table 1). Paired t-tests were performed to explore the extent to which the breast volumes calculated with the two software programs were significantly different for each assessor. Lin's concordance was used to assess the extent to which the breast volume measures calculated by the two software programs were identical.21,22 Lin's concordance was interpreted as follows: >0.99 almost perfect agreement, 0.95–0.99 substantial agreement, 0.90–0.95 moderate agreement, and <0.90 poor agreement. 23
Participant Characteristics, Where Breast Volume was Calculated Using Three-Dimensional Surface Imaging
SD, standard deviation; WLE, wide local excision.
The extent of the reliability for use of each software program was assessed with ICC (ICC2,1,/ICCagreement) and displayed graphically with Bland–Altman plots. The ICCs were interpreted as follows: 0.95 or above indicated excellent reliability, 0.75–0.94 indicated substantial reliability, 0.4–0.74 indicated moderate reliability, and ≤0.4 indicated poor reliability. 24
Data from the ICC were used to calculate the error associated with the measurement of breast volume and the amount of change required that is greater than the error of the tool. Standard error of measurement (SEMagreement), SEM percent (SEM %), as well as the SDC (SDCagreement) and SDC percent (SDC%) were used to assess the variation between the assessment occasions.25,26
The following equations, based on guidance in Measurement in Medicine,
26
were used to calculate reliability and measurement properties:
The mean in Equations (4) and (5) is mean of all the volume measures calculated by three assessors (inter-rater) or one assessor on two assessment occasions (intra-rater).
IBM SPSS Statistics (online version no. 27) was used for statistical analysis.
Results
Images from 51 women resulting in 100 individual breast images were included in this study. Two women had one breast that was not eligible for inclusion, one due to a ptosis rating of three on the unoperated breast and one where an area of breast had not been captured by the Vectra-XT cameras. Breast volumes were measured using both VAM and Breast Sculptor software by all three assessors, blinded to the other assessor's measures. One assessor (N.F.) measured the volumes twice, 1 week between assessment, without reference or recall to the previous results.
Participant characteristics
Participant characteristics are given in Table 1. Seventy percent of images were taken preoperatively. Of those whose images were taken postoperatively (n = 15), wide local excision was performed in all women, with four women also undergoing a mammoplasty and one a mastopexy.
The breast volumes determined from the two software programs were not significantly different for two assessors (p = 0.4) but were significantly different for one assessor (p = 0.009). The mean difference in breast volume between the two software programs ranged from −9.42 to 33.07 cc (Table 2). Lin's concordance was <0.90 for all assessors, indicating poor agreement between the two software programs.
Breast Volume (cc) Measured Using Breast Sculptor and Vectra 3D Analysis Module Software
cc, cubic centimeters; CI, confidence interval; SD, standard deviation; VAM, VECTRA® 3D Analysis Module.
VAM measurement properties
Volume calculation using VAM software had excellent intra-rater reliability (ICC = 0.991, 95% CI: 0.986–0.994) and inter-rater reliability (ICC = 0.958, 95% CI: 0.939–0.972); Fig. 3), with inter-rater bias ranging from −1.0% to −5.6% between assessors The intra-rater SEM was 20.2 cc (SEM% = 4.1%), with a SDC of 56 cc (SDC% = 11.3%). The inter-rater SEM was 42.4 cc (SEM% = 8.7%) and SDC was 117.4 cc (SDC% = 24.1%) (Table 3).
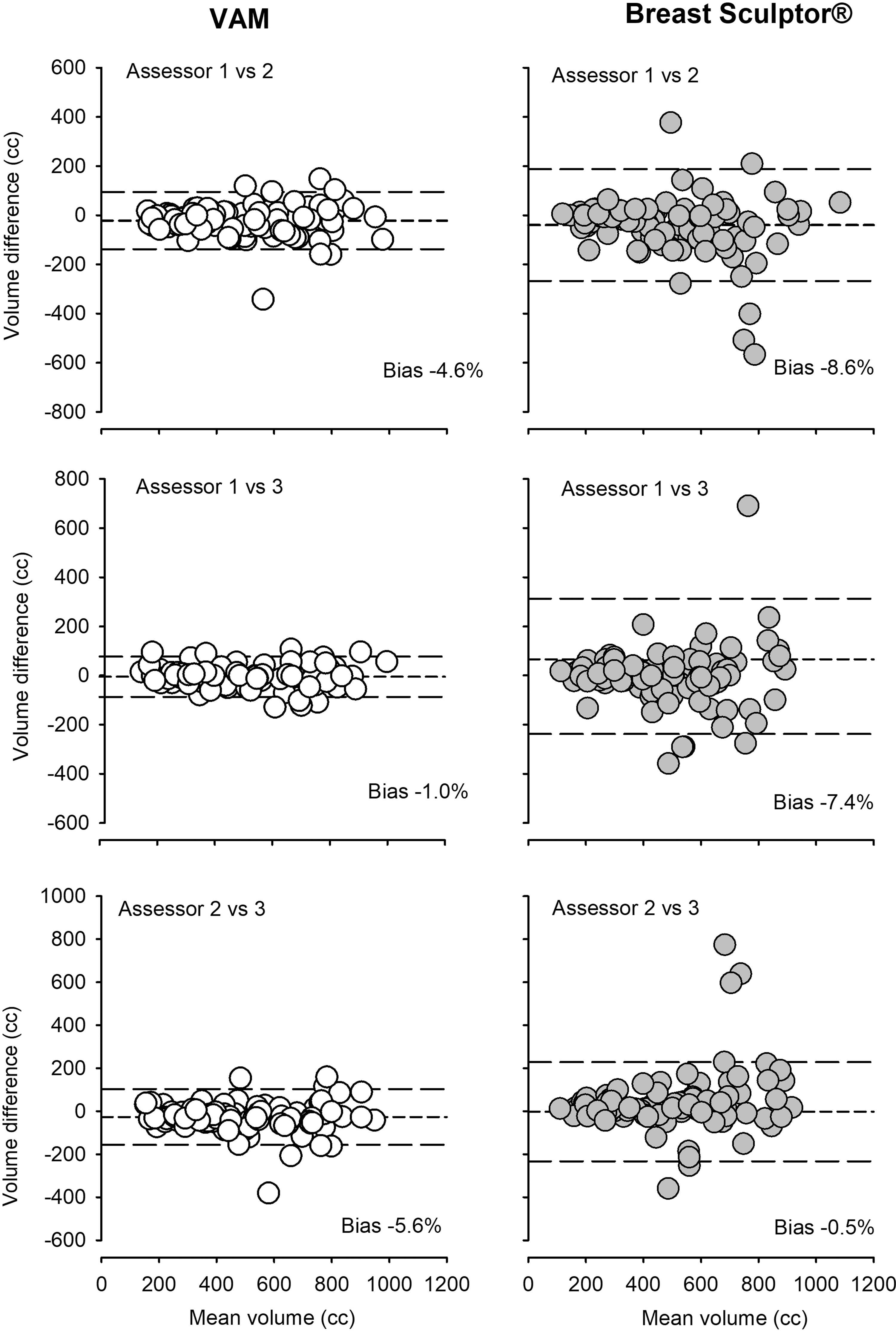
Bland–Altman plots showing the averages of breast volumes from VAM (left) and Breast Sculptor® (right) against the differences between the measurements by two assessors. The short-dashed line represents the mean and the long-dashed line represents 1.96 the standard deviation of the difference between two assessors.
Reliability, Standard Error of Measurement and Smallest Detectable Change of Breast Volume Measurement Using Three-Dimensional Surface Imaging
ICC, intraclass correlation coefficient.
Breast Sculptor measurement properties
Reliability of volume calculations using Breast Sculptor was substantial for intra-rater reliability (ICC = 0.908; 95% CI: 0.866–0.938) and inter-rater reliability (ICC = 0.830; 95% CI: 0.771–0.877) Table 3, with inter-rater bias ranging from −0.5% to −8.6% between assessors. Intra-rater SEM was 74.3 cc (SEM% = 14.5%), whereas the inter-rater SEM was 90.9 cc (SEM% = 19.1%). The SDC for measurement of breast volumes was 206.2 cc (SDC% = 40.2%) for a single assessor and 252.1 cc (SDC% = 52.9%) when multiple assessors were used (Table 3).
Discussion
Measurement of breast volume of women using the VECTRA-XT 3D surface imaging device and two available software analysis programs was performed by three novice assessors trained in a standardized measurement technique. We found substantial to excellent intra- and inter-rater reliability for the assessors using the software programs. Although both programs were highly reliable, there was poor agreement between the measures of each assessor, demonstrated by the low Lin's concordance.
Furthermore, measurement error varied considerably between the programs. A single assessor using the VAM software had the least measurement error, whereas the greatest/highest measurement error occurred when multiple assessors used Breast Sculptor software. Breast Sculptor and VAM, therefore, cannot be used interchangeably, and VAM is the preferred tool for assessment of clinical measures of breast volume.
Although this study found that VECTRA-XT and VAM can reliably quantify breast volume, quantification of a small change in breast volume that likely occurs with breast lymphedema is likely outside the error of this measurement tool and approach. The SDC, that is, the change in volume beyond the measurement error, was smallest when VAM software was used but still equated to 11% of total mean breast volume. It is not currently known what volume of edema reduction is meaningful or clinically relevant. Other tools, such as patient-reported outcomes and ultrasound, which capture different signs and symptoms of breast lymphedema, could be used in combination with 3D-SI in clinical practice to ensure that other meaningful changes in breast lymphedema presentation are captured.
The SEM of an assessment tool has implications for its clinical utility. A 2015 Delphi study including surgeons, oncologists, lymphedema therapists, and consumers determined that the error for breast volume measurement using 3D-SI should be <5%. 27 However, whether this is achievable has been questioned. 15 In our study, the only circumstance in which this was achieved was when VAM software and a single assessor were used. This is because there are a number of places where error can be introduced when measuring breast volume with 3D-SI. First of all, although the importance of being able to undertake these measurements with little experience was identified in the Delphi study as preferable for use in clinical practice, novice assessors may introduce error.
However, with the use of rigorous training and a standardized protocol, we were able to achieve low error with novice assessors. Second, the identification of the landmarks and the breast border is difficult to standardize. In our study, we used a template image to assist with standardized demarcation of the borders. This was guided by the seven pen landmarks marked by clinical staff at the time the image was taken, however, assessors found that the upper lateral border close to the shoulder and lateral breast border difficult to define, especially when anatomical landmarks were less visible due to adipose tissue.
Techniques of palpation of the breast and additional marking on the skin at the time of image capture have been used in other studies to help with border identification with 3D-SI software programs, resulting in better accuracy and less measurement bias.5,28–30 To minimize error in future studies, recommended strategies include training of the assessor accompanied with a detailed protocol that includes additional and accurate marking of landmarks using palpation at the time of image collection.
There is debate in the literature about whether factors such as BMI, breast ptosis, and the interpolation method used affect the reproducibility of breast volume measurement using 3D-SI, with the impact of breast size being particularly controversial.5,11,15,18,31 Losken et al. found that there was more measurement bias with smaller breast sizes, 31 whereas Wesselius et al. found the opposite, with larger breasts having greater measurement error. 15 Moreover, Yip et al. found no difference in 3D-SI measurement error across a range of breast sizes. 30 Killaars et al. found that 3D-SI reliability was high regardless of breast size, but that there was an increasing difference between breast volume measured by MRI and 3D-SI as breast sizes increased. 12
In our study, images were not excluded based on the women's BMI or breast volume, but an image was excluded if the breast had grade 3 breast ptosis, or the inferior mammary fold could not be viewed on the image, as this was thought to impact on the interpolation of the chest border. 18 Error associated with measurement of ptotic versus nonptotic breast has not been fully explored, but one study has trialed a strategy to enable visualization of the inferior mammary fold in women with ptotic breasts, using a semireclined position for 3D-SI capture. 32
The interpolation method of creating the chest wall for breast volume measurement has also been compared with a statistical shape model (SSM) method using CT images in one study, 33 showing higher determination coefficient (R 2 = 0.737) with the SSM technique compared with the interpolation method (R 2 = 0.404). However, the requirement for CT in addition to 3D-SI increases the imaging burden impacting on clinical usefulness of 3D-SI. 33 Future research should investigate whether these or other strategies can improve SEM, across women of all body and breast shapes as well as sizes.
In conclusion, VECTRA-XT with VAM software shows promise as a reliable way to measure breast volume when novice assessors follow a standardized measurement technique. Reproducibility, measured by SEM, and SDC, however, may not be sufficient to detect change in breast volume to assess the outcomes of breast lymphedema interventions or change over time. Measurement error for this approach cannot be wholly evaluated without a definition of minimal important change, which has not yet been established. Further research using this measurement tool in women with breast lymphedema, in conjunction with other measurement approaches, is required to determine its usefulness in this population.
Footnotes
Acknowledgments
The authors thank Betty Schofield and Joyce Anderson Bequest for the funding provided.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by a Betty Schofield and Joyce Anderson Bequest grant.