
Abstract
Background:
Breast cancer-related lymphedema (BCRL) is a common complication of breast cancer treatment. Anecdotal and qualitative research suggests that heat and hot weather cause an exacerbation of BCRL; however, there is little quantitative evidence to support this. The aim of this article is to investigate the relationship between seasonal climate variation and limb size, volume, fluid distribution, and diagnosis in women following breast cancer treatment.
Methods and Results:
Women older than the age of 35 years who had undergone treatment for breast cancer were invited to participate. Twenty-five women aged between 38 and 82 years were recruited. Seventy-two percent received surgery, radiation therapy, and chemotherapy as part of their breast cancer treatment. Participants completed anthropometric, circumferential, and bioimpedance measures and a survey on three occasions: November (spring), February (summer), and June (winter). Diagnostic criteria of >2 cm and >200 mL difference between the affected and unaffected arm, and a positive bioimpedance ratio of >1.139 for a dominant arm and >1.066 for nondominant arm was applied across the three measurement occasions. No significant correlation between seasonal variation in climate and upper limb size, volume, or fluid distribution were found in women diagnosed with or at risk of developing BCRL. Lymphedema diagnosis depends on the season and diagnostic measurement tool utilized.
Conclusion:
There was no statistically significant variation in limb size, volume, or fluid distribution in this population across spring, summer, and winter, although there were linked trends in these values. The diagnosis of lymphedema, however, varied between individual participants throughout the year. This has important implications for the implementation/commencement of treatment and management. Further research with a larger population in different climates is required to explore the status of women with respect to BCRL. The use of common clinical diagnostic criteria did not result in consistent diagnostic classification of BCRL for the women involved in this study.
Introduction
Breast cancer-related lymphedema (BCRL) is a complication of breast cancer treatment, which can lead to a significantly reduced emotional wellbeing and poorer general health compared to women who do not develop BCRL.1,2 Radiation and surgery for breast cancer have the potential to damage the lymphatic system in the arm and axilla3–5 and the risk of developing BCRL is higher when the patient receives both interventions.6–8 Although the lymphatic system is damaged during these interventions, there is some residual capacity to maintain the balance between lymph fluid production and drainage as well as capacity for regeneration of lymphatic vessels. 9 This residual capacity explains why ∼27% of people who have had axillary clearance and radiation therapy develop BCRL and only 3%–5% who have just had sentinel nodes removed. 10 Secondary lymphedema will develop when the lymph load exceeds the transport capacity of the remaining lymph vessels. 11
Heat and humidity have been self-reported as aggravating factors of lymphedema symptoms as well as a major contributor to noncompliance in wearing compression garments. 12 This aggravation is thought to be a result of increased blood flow, that subsequently increases the volume of lymph produced, 13 as well as increased discomfort from garment use.14,15 In addition, other aggravating factors for BCRL include infection, injury, and strenuous exercise as they may overwhelm the compromised lymphatic system.13,16,17
Previous studies have provided qualitative evidence that hot weather aggravates symptoms of BCRL,13,18,19 with the percentage of women with BCRL who report aggravation of arm swelling due to heat and hot weather varying from 27% 20 to 58%. 21 However, there are only two quantitative studies published that address this topic. 12 One study of healthy women and women with BCRL was completed in Sydney Australia. 19 It identified a correlation between average maximum temperature and measures of the lymphedematous arm; however, no such relationship was identified in the healthy population. 19 Matthews et al 22 investigated the effect of seasonal variations in climate and upper limb (UL) measures in a healthy population in a tropical climate. Measurements were completed on three occasions, which represented three different seasons according to the Thom's Discomfort Index (TDI) (Fig. 1).23,24
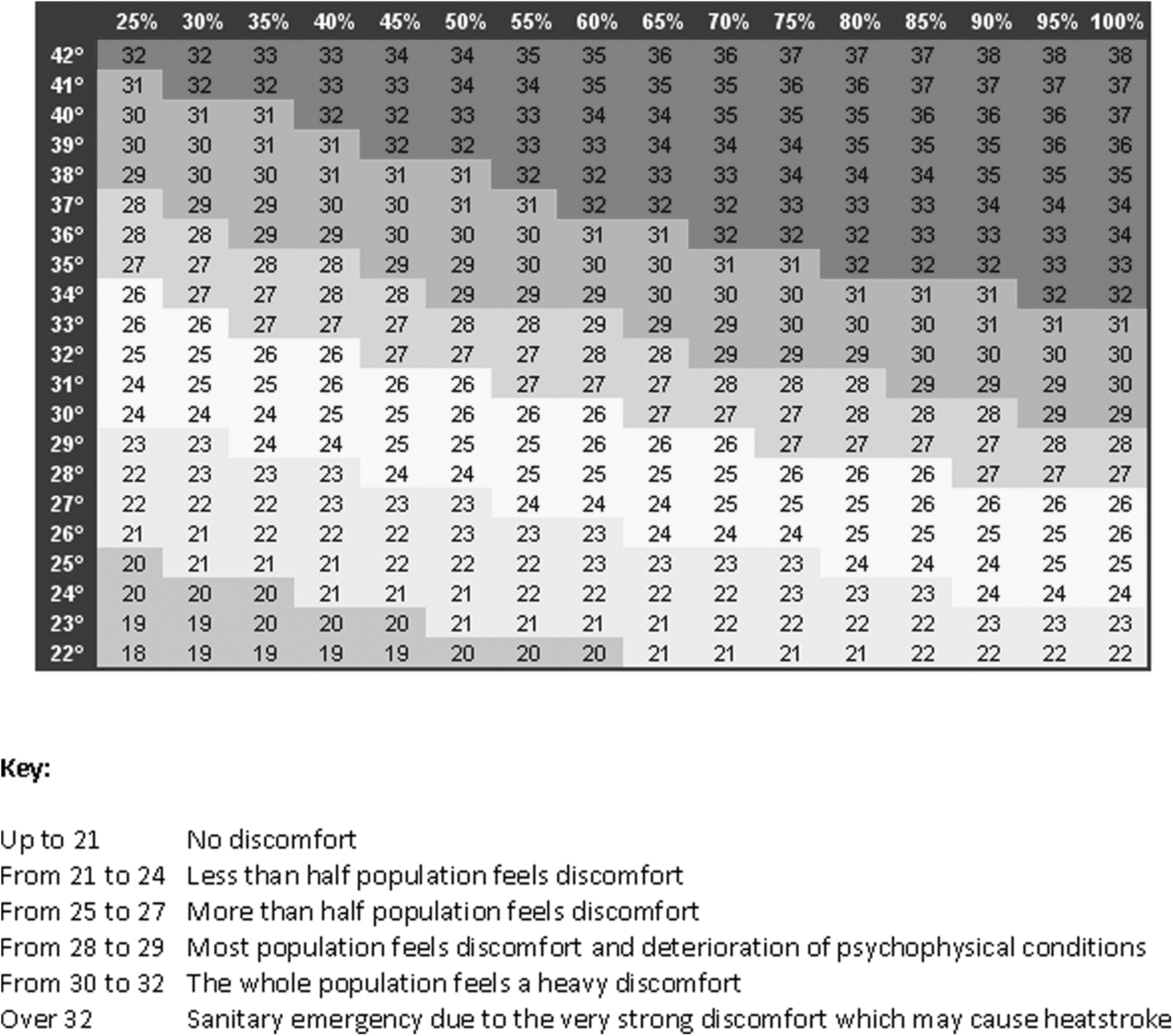
The Thom's Discomfort Index.
A statistically significant increase in gross UL size, as measured by sum of anatomical circumferences (SOAC), was found in spring compared to summer and winter. It was suggested that higher temperatures with low humidity were responsible. 22 However, while lymphatic function is compromised following breast cancer treatment, this is not so for a healthy population, thus these findings are not relevant to women after breast cancer treatment.
The primary aim of our study was to investigate the relationship between climate and UL size, volume, and fluid distribution in two groups of women, one comprising women who had developed BRCL and the other who were at risk of developing BCRL. The secondary aim was to explore the relationship between diagnostic criteria and climate for women diagnosed with or at risk of developing BCRL.
Methods
Ethics
Ethical approval was received from the James Cook University Human Research Ethics Committee and subsequently from the Townsville Health Service District Human Research Ethics Committee (HREC/10/QTHS/113 and Site-Specific Assessment SSA/10/QTHS/150) before commencing data collection.
Timing of measures
Measurements were undertaken in Townsville, Northern Australia, in November 2010 (spring), February 2011 (summer), and June 2011 (winter). Timing was chosen based on the TDI. The TDI is a weather index that takes into account average maximum temperature and relative humidity to evaluate the percentage of the population that will feel discomfort due to the climate. 25 It is a simple approach that uses readily available data and has been shown to be a valid measure of human thermal comfort.23,25 Based on historical data and the TDI (Fig. 1), in November (TDI rating 25–27), more than half the population would feel discomfort due to heat and humidity, in February (TDI rating 28), most of the population would feel discomfort and deterioration of psychophysical conditions due to heat and humidity, and in June (TDI rating 23–24), less than half the population would feel discomfort due to heat and humidity. 26
Recruitment
Potential participants were invited from the list of patients accessing services following breast cancer treatment at The Townsville Hospital, Australia. Participants were included if they were women older than 35 years of age who had undergone treatment for breast cancer and either developed BCRL (diagnosed with BCRL group) or had >10 lymph nodes removed placing them at increased risk of BCRL (at risk of developing lymphedema group).18,27 Women were excluded if they were still receiving active breast cancer treatment, if they were currently pregnant, if they had an implanted electrical stimulation device (such as a pacemaker), or were unavailable on all three measurement occasions.
Outcome measures
Participants completed a short survey at the beginning of the first measurement occasion to collect demographic information, which included age, occupation, dominant hand, and affected side. In addition, at each measurement occasion, questions regarding confounding factors for arm swelling and bioimpedance measures were asked. These included if they had traveled in the last 3 months, if they had done any physical activity or deliberate exercise in the last 24 hours, if they had eaten any food in the last hour, if they had consumed any alcohol in the last 24 hours, and how much fluid they had to drink that day. Further, they were asked if they had been diagnosed with BCRL, their management regime, if they had experienced any swelling in the last 3 months, and if so, what they felt were the triggering factors for swelling.
To establish consistency of overall body size across the three occasions of measurement, participant's weight, hip, and waist measurements were taken. Height was measured using a stadiometer.28,29 Weight was taken in light day clothes and with shoes off using a set of bathroom scales. Hip and waist measurements were completed using a retractable tape measure with the participant in standing with their feet together. Waist circumferences were taken at the narrowest part of the torso. 28 Hip circumferences made with the tape measure placed over both anterior and superior iliac spines. All anthropometric measurements were completed by the principal investigator on all three occasions. Body mass index (BMI) was calculated (weight in kg/height in metres 2 ) for each occasion using the height and weight measurements collected. 30
Circumferential measurements were completed by the principal investigator on all three occasions. Measurement was undertaken according to the Australasian Lymphology Association's national standards for measuring lymphedematous limbs. 31 Based on circumferential measurement of the arm, a >2 cm difference between the affected and unaffected limb, or a >2 cm increase over time of the affected limb at any specific measurement point, is indicative of lymphedema,3,13 although limb dominance may affect these differences.
Limb size was calculated using the SOAC, which is the total of the metacarpophalangeal, ulna styloid, olecranon, and acromion circumferential measures A difference of >5 cm between the affected and unaffected arm is indicative of lymphedema. 32
Limb volume was calculated using the frustum formula. Four frustums were calculated for each arm and total limb volume was calculated by adding the four frustums together. 33 The frustum formula for limb volume calculation has been shown to be superior to cylindrical, rectangular, solid and trapezoidal solid formulas, as it has the highest correlation with measures from the water displacement method. 34 A difference of >200 mL between the affected and unaffected arm, or a change of >200 mL of the affected arm on different occasions, indicates the presence of lymphedema. 35
Bioimpedance involves passing an unnoticeable electrical current through body tissues to estimate the amount of intracellular and extracellular fluid in a limb36,37 and has been shown to be a sensitive, specific, and reliable clinical measure of lymphedema.36–38 An ImpediMed SFB7 unit was used to collect bioimpedance data of the limbs and measurements followed the manufacturer's guidelines. 39 A bioimpedance ratio was calculated by dividing the intracellular fluid by the extracellular fluid (Ri/Re). 40 Then, using this ratio, a diagnostic ratio was calculated by dividing the unaffected arm by the affected arm. If the dominant arm is the affected arm, a positive diagnostic ratio is >1.139. If the nondominant arm is the affected arm, a positive diagnostic ratio is >1.066. 40 Manual records of Ri and Re were completed at the time of measures and cross referenced with downloaded electronic data before being included in data analysis.
Preliminary reliability
Intrarater reliability for circumferential measurements was completed concurrently with each collection occasion. Before the initial measurement occasion, and during the second and third measurement occasions, both arms of five volunteers were measured twice to ensure that circumferential measures were reliable before participant data collection took place.
Data analysis
IBM SPSS Statistics 19 was used for all data analyses. All data were analyzed separately for those diagnosed with BCRL and those at risk of developing BCRL.
Intrasubject comparison across three occasions of measurement was completed using a Repeated Measures Analysis of Covariance (ANCOVA) to establish if significant change had occurred between the three measurement occasions for each of the following variables: SOAC, total limb volume, and the bioimpedance ratio. The confounding variables; if the participant had traveled within the last 3 months, if they had completed any physical activity or deliberate exercise in the last 24 hours, if they had felt heaviness or swelling in the last 3 months, if they had consumed food in the last hour or alcohol in the last 24 hours, and how much fluid they had to drink that day were each analyzed independently and in conjunction with each other for each variable. A p-value of <0.05 was considered significant.
Although arm dominance has been shown to affect the size, shape, and bioimpedance of the limb,41,42 this study did not account for arm dominance in data analysis, as all comparisons were intrasubject across three occasions. However, it was considered with respect to diagnostic classification using bioimpedance.
Results
Reliability
Excellent reliability for all circumferential measures was established before and during this research with concordance correlation coefficients range between 0.992 and 0.999.
Participant retention
Twenty-five participants attended all three measurement occasions and only these data were included in data analysis. A participant flowchart with reasons for drop out is provided in Figure 2.
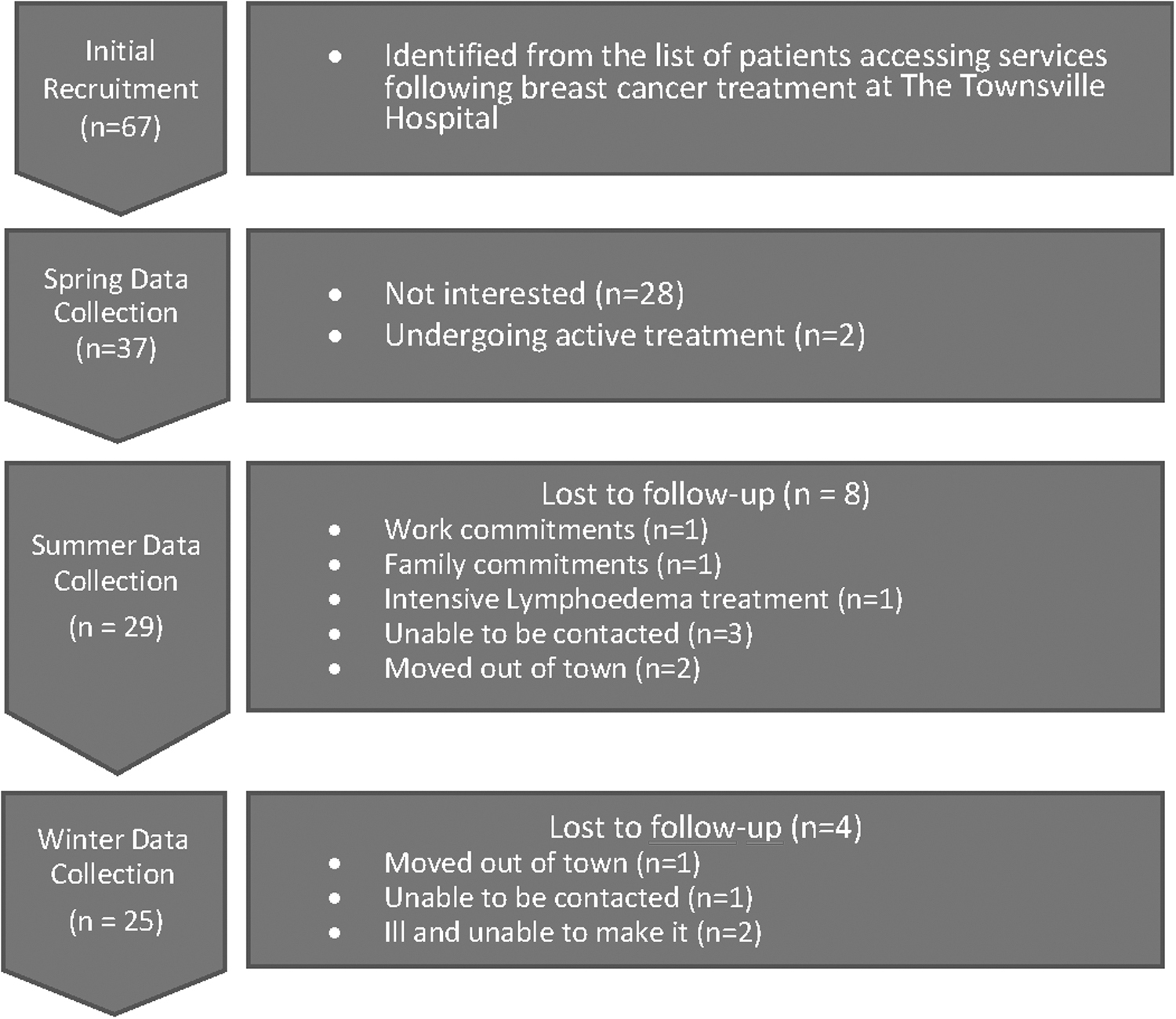
Participant recruitment and retention.
Climate
According to the prediction of the TDI, each measurement occasion constituted a different level of discomfort according to heat and humidity (Table 1).
Climate for Each Measurement Occasion 26
Participant demographics
The median age of participants was 57 years (range 39–82 years). The majority (72%) of participants had undergone chemotherapy, radiation therapy, and surgical intervention as part of their breast cancer treatment. Twelve percent of participants had undergone surgery and chemotherapy, 8% had undergone surgery alone, and 4% had undergone radiation only and surgery and radiation, respectively. On the final measurement occasion, 56% (n = 14) of participants had been diagnosed with BCRL, however, this altered over the 8 months of the study with one more participant diagnosed at each measurement occasion by an external source. Most participants were right hand dominant (88%) and had the left side affected by breast cancer (60%).
The mean BMI of participants was above 30 on all three occasions, which is considered obese. 30 Waist measurements and hip measurements of the participants were also considered to be at the overweight level (Table 2). 43 None of the participants' anthropometric measurements changed significantly over the 8 months between measurement occasions, so changes in limb size were not related to overall change in body weight.
Anthropometric Measures
The highest number of participants reported feeling heaviness in their arm or hand in spring (56%) compared to summer or winter (48% on both occasions). The most reported aggravating factors for a feeling of heaviness were exercise, hot weather, and rest (Table 3). The number of participants reporting swelling in their arm or hand was higher in spring and summer (48% and 52%, respectively) than in winter (28%).
Reasons Provided by Participants for a Feeling of Heaviness in the Arm or Hand (More Than One Symptom Reported for Some Participants)
There was no significant difference in limb size (SOAC), limb volume, (calculated Frustum) or fluid distribution (bioimpedance) across the measurement occasions in participants diagnosed with BCRL or participants at risk of developing BCRL.
BCRL, breast cancer-related lymphedema; SOAC, sum of anatomical circumferences.
Of those diagnosed with BCRL, most (83% in spring, 77% in summer, 86% in winter) used a combination of the following management techniques at home, compression garments, self-massage, and circulation exercises. Most of these participants reported maintaining the same management regime all year round (spring 66.7%, summer 76.9%, winter 78.6%).
Climate and outcome measures
Data were collected on a range of possible confounding variables. Each of these was included in the ANCOVA for both participants diagnosed with BCRL and those at risk of developing BCRL. There was no significant difference in limb size (SOAC), limb volume (calculated Frustum), or fluid distribution (bioimpedance) across the measurement occasions in participants diagnosed with BCRL or participants at risk of developing BCRL (Tables 4 and 5).
Limb Size, Limb Volume, and Fluid Distribution in Participants Previously Diagnosed with Breast Cancer-Related Lymphedema
ANCOVA, analysis of covariance.
Limb Size, Limb Volume, and Fluid Distribution in Participants Considered “at risk” of Developing Breast Cancer-Related Lymphedema
Diagnostic results
Diagnostic criteria for circumferential measures, calculated limb volume, and the bioimpedance ratio were applied to each participant at each measurement occasion (Table 6). This identified that, of the 14 participants with a diagnosis of BCRL at the final measurement occasion, only 11 would have been diagnosed on any measurement occasion using the circumferential criteria, 5 would have been diagnosed on any measurement occasion using the volumetric criteria, and 5 would have been diagnosed on any measurement occasion using the bioimpedance criteria. One woman diagnosed with BCRL before the initial measurement occasion met the diagnostic criteria for the bioimpedance ratio on only one occasion and all other diagnostic criteria were negative at each measurement occasion, and one woman did not meet any diagnostic criteria on any occasion despite a previous diagnosis of BCRL.
Number of Participants Who Would Have Been Diagnosed by Each Diagnostic Criterion at Each Measurement Occasion
Of those 11 participants at risk of developing BCRL, 7 would have been diagnosed on one or more occasion using the circumferential measure criteria, 3 would have been diagnosed using the volume criteria, and 2 would have been diagnosed on one or more occasion using the bioimpedance criteria.
Discussion
No relationship was identified between seasonal variation in climate and UL size, volume, or fluid distribution in participants following breast cancer treatment. However, the survey data collected supports feelings of increased swelling and heaviness in hot weather. The lack of quantitative change differs from the findings in a similar demographic, healthy population in Townsville 22 and in healthy women and those diagnosed with BCRL in the Sydney area. 19
Although there was no significant correlation between seasonal variation and UL size, volume, or fluid distribution, there was a trend both in women diagnosed with and at risk of developing BCRL, to have larger measures in spring compared to summer and winter. This is in concordance with measures of a healthy population in the same region on similar measurement occasions. 22 The relatively small sample size of this study will have caused the study to lose the power to detect a significant difference even if there was one there 44 and studies with larger sample sizes are indicated in the future.
The difference in weather conditions between Sydney and Townsville may explain the differing results between this study and Czerniec et al. 19 Sydney is situated ∼2100 km south of Townsville and it therefore experiences a larger change in temperature between summer and winter months. The average maximum temperatures in Townsville during the three measurement occasions were 28.9°C (spring), 30.5°C (summer), and 24.8°C (winter). 26 Comparatively, Sydney has a cooler climate with average maximum temperatures of 23.5°C (spring), 28.4°C (summer), and 18°C (winter). 26
The survey data from this study support previous qualitative reports of increased arm swelling and heaviness in hot weather.20,21 Participants commonly reported a feeling of swelling in their arms in spring and summer (48% and 52% respectively) more than in winter (28%).
A significant finding from this study related to the diagnosis of BCRL. The diagnosis of BCRL for participants in this study varied according to the diagnostic criteria used and the occasion of measure, leading to potential diagnostic misinterpretation. There was a low level of agreement between diagnostic criteria with only one participant meeting all three diagnostic criteria on one occasion. The circumferential criteria diagnosed more participants than the other two techniques in participants with and without a prior diagnosis of BCRL. This is the most commonly used diagnostic criteria in clinical practice, 45 and may result in a higher prevalence of BCRL than if other criteria were used.
Fluctuations in BCRL are more prevalent within the first-year postsurgery compared to longer term when secondary changes such as fibrosis are occurring, 46 which may explain the differences between data collection points. Secondary lymphedema will be in the acute stage when an initial diagnosis is made. More recent commentary indicates the blurring of diagnosis and management of chronic edema, lymphedema, and other vascular edemas.47–49 A verification measurement 3 or 4 months following the initial diagnosis may be required before initiating treatment, and patients should be counseled about the fluctuations expected in the acute phase, and the importance of early diagnosis and early management.46,50 The weather season and climate that the woman lives in also need to be considered, as the measures taken may also alter the diagnosis, as there is a trend for arm measures to be larger in hot seasons.
As previously stated, the small sample size of this study may have limited its ability to find statistically significant results. 44 There were 17 (20%) participants lost to follow-up. Future study designs should consider how to maintain retention to maximize power. Also, although participants were reminded before each measurement occasion to avoid certain confounding activities for circumferential measures and bioimpedance readings, it is likely that there was varying compliance. Increased control of these confounding factors may improve standardization and alter results.
Strengths of the study include that all measurement techniques completed were of high reliability and consistency. Circumferential measures were undertaken following the Australian national standard for measuring lymphedematous limbs, 31 which are still current. High concordance correlation coefficients were found for all measurement points on the arm on all three measurement occasions. Therefore, it could be concluded that any change in circumferential measures would be due to a change in arm size, not measurement error. Bioimpedance was conducted following the manufacturers guidelines, 39 which makes it safe and repeatable in other studies and confirms our ability to compare these results with other studies.
Conclusion
This study found no statistically significant change in arm size, volume, or fluid distribution due to seasonal variation in climate in a population of women older than the age of 35 years, living in the Townsville region, following breast cancer treatment. Our findings differ from previous research findings in healthy Townsville women and women with and without BCRL from Sydney. However, participants in this study did report feelings of arm heaviness more commonly in the warmer seasons, and seasonal limb volume differences appear to be biologically or perhaps practically significant.
The application of common clinical diagnostic criteria at the same time to women included in this study did not result in consistent diagnostic classification of BCRL. This has important implications for diagnosis and resultant implementation/commencement of treatment and management. Further research with a larger population in different climates is required to further explore its impact on the parameters examined in this study.
Footnotes
Acknowledgments
Sue Gordon for supervision guidance, perseverance, understanding, time, and effort. Jennifer Thompson and Nicola Cosgriff—for their support during the methodology's formation and during the participant recruitment phase. Jennifer Thompson and Helen Land—for support during data collection. Petra Buttner and Gary Williams—for support with statistical analysis. Sally Ruston—for support and organization. To all participants—thank you for your commitment and honesty, without you, this research would not be possible.
Authors' Contributions
J.P. was the primary researcher and author. S.G. provided supervisory guidance, including conceptualization, investigation, methodology, and analysis. She also contributed to writing—reviewing and editing. S.W. was involved in writing—original draft and writing—reviewing and editing. N.P. completed writing—reviewing and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was primarily completed in partial fulfilment of the requirements of the James Cook University degree of Bachelor of Physiotherapy with Honours. No additional funding was received to complete this project.