
Abstract
Background:
Indocyanine green (ICG) fluorescence lymphography is widely used to diagnose lymphedema. There is little consensus on the appropriate injection method for ICG fluorescence lymphangiography. We used a three-microneedle device (TMD) for skin injection of ICG solution and investigated its usefulness.
Methods and Results:
Thirty healthy volunteers were injected with ICG solution using a 27-gauge (27G) needle in one foot and a TMD in the other foot. Injection-related pain was evaluated using the Numerical Rating Scale (NRS) and Face Rating Scale (FRS). The skin depth of the injected ICG solution was evaluated by injecting the solution into the skin of amputated lower limbs using a 27G needle or TMD using ICG fluorescence microscopy. The median and interquartile range of the NRS scores was 3 (3–4) and 2 (2–4) in the 27G needle and TMD groups, respectively; that of the FRS scores was 2 (2–3) and 2 (1–2) in the 27G needle and TMD groups, respectively. Injection-related pain was significantly lower with the TMD than with the 27G needle. The lymphatic vessels were similarly visible using both needles. The depth of the ICG solution varied for each injection with a 27G needle (400–1200 μm) and was consistent at ∼300–700 μm below the skin surface using the TMD. Injection depth was significantly different between the 27G needle and the TMD.
Conclusions:
Injection-related pain decreased using the TMD, and ICG solution depth was consistent on fluorescence lymphography. A TMD may be useful for ICG fluorescence lymphography.
Clinical Trials Registry (UMIN-CTR; ID: UMIN000033425).
Introduction
Lymphatic circulation plays an important role in maintaining homeostasis in the body's fluid balance and immune system. 1 Lymphatic transport is often interrupted by cancer surgery, trauma, filariasis infection, or insufficiency in the development of lymphatic vessels. 2 Interruption of lymphatic transport causes stasis of lymphatic fluid and lymphedema. Therefore, evaluating lymphatic circulation is important for diagnosing lymphedema.
Blood circulation is a closed system. However, lymphatic circulation is an open system that starts from the periphery and is thus difficult to evaluate. Moreover, lymphatic fluid is colorless; therefore, injection of a contrast agent into peripheral lymphatic vessels is required to evaluate lymphatic circulation. Direct lymphography 3 and lymphatic scintigraphy 4 have been used to evaluate lymphatic circulation for decades. However, direct lymphography 5 is invasive, and lymphatic scintigraphy 4 is unsuitable for evaluating thin lymphatic vessels.
We previously reported the usefulness of fluorescence lymphography in evaluating lymphatic circulation. 6 Indocyanine green (ICG) is used as an optical tracer agent, and its solution is injected into the peripheral skin. The fluorescence signals of ICG are observed using a near-infrared camera. 6 Due to its safety, simplicity, and real-time observation capabilities, ICG fluorescence lymphangiography is widely used to diagnose lymphedema or to observe lymphatic vessels during surgery. 6
The fluorescence images obtained during ICG fluorescence lymphangiography depend greatly on the quality of the cameras used during imaging. 7 In the time since the first report of ICG fluorescence lymphography for lymphedema, 6 near-infrared cameras have dramatically improved in terms of the number of pixels and color images. 8 Improvements in the injection methods have been suggested, such as mixing ICG with a local anesthetic agent 9 or using a cryogenic numbing device. 10 However, there is little consensus on the appropriate injection method for ICG fluorescence lymphangiography. The ideal technique for injecting ICG solution must be painless, should have broad diffusion with fewer complications, and should be consistently applied.
A three-microneedle device (TMD) (UNIEVER; Unisis Corp., Saitama, Japan) has been developed, and its usefulness in local anesthesia has been reported.11,12 Needlestick pain is reportedly significantly lower while using a TMD than while using a conventional 27-gauge (27G) needle. 12 We hypothesized that the use of TMD might reduce the invasiveness of the ICG solution injection and might enable stable injection during ICG fluorescence lymphography. Therefore, this study aimed to investigate the usefulness of TMD in ICG fluorescence lymphography.
Materials and Methods
Setting and sample
This retrospective study consisted of two parts. First, we evaluated the injection-related pain associated with the injection of the ICG solution using a TMD during fluorescence lymphography. In the second part, we histologically investigated the depth of ICG injection in skin tissues using the TMD. Healthy volunteers participated in this study between November and December 2014. Volunteers with edema in the lower extremities and those with a history of iodine allergy were excluded from this study. Written informed consent was obtained from all participants. A standard questionnaire that included complaints of leg edema, body weight, height, and body mass index (BMI) was provided.
Study approval
The study protocols were approved by the Ethics Review Board of the Hamamatsu University School of Medicine (approved number 18-062) and were registered with the UMIN Clinical Trials Registry. Written informed consent was obtained from all participants.
Structure of a TMD and conventional needle
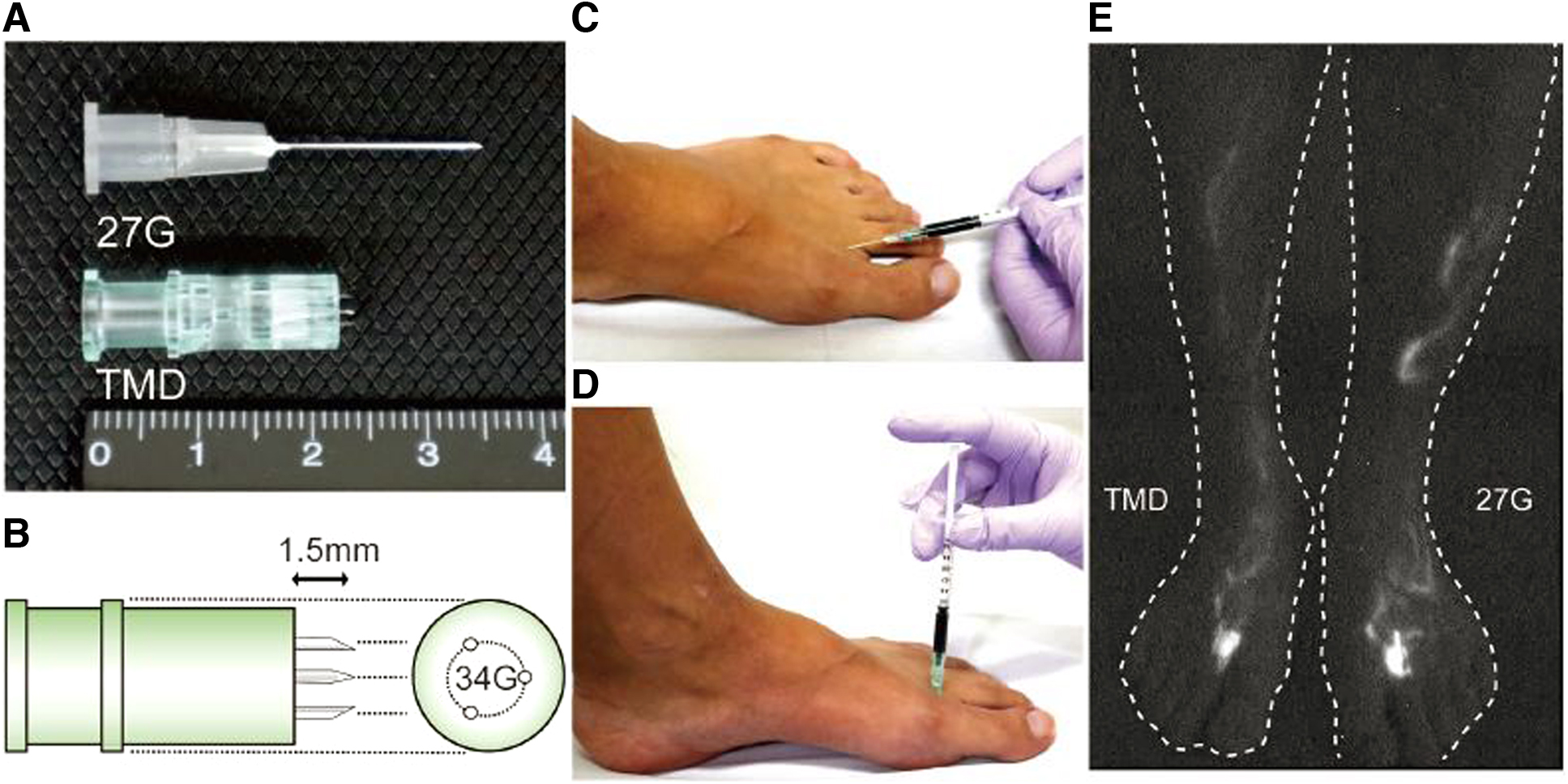
The TMD has three stainless-steel needles. The outer diameter of each needle was 0.16 mm (34-gauge) with an exposed length of 1.5 mm (Fig. 1A). Three stainless-steel needles were arranged in a circular manner, and the bevel angle was 12°, facing outward (Fig. 1B).11,12 The 27G needle has an outer diameter of 0.40 mm, an exposed length of 19 mm, and a short bevel angle of 18° (Fig. 1A).
Fluorescence lymphography using a TMD.
A 27G needle was affixed to a conventional 1-mL syringe, the needle was tilted, and ICG solution was injected into the skin (Fig. 1C). A TMD was affixed to a conventional 1-mL syringe, and ICG solution was injected into the skin perpendicularly (Fig. 1D).
ICG fluorescence lymphography
ICG (Daiichi Pharmaceutical, Tokyo, Japan) was used as an optical tracer, and a near-infrared camera (Photodynamic Eye; Hamamatsu Photonics K. K., Hamamatsu, Japan) was used for fluorescence observation. The Photodynamic Eye camera has a light-emitting diode and activates ICG with emitted light at a wavelength of 760 nm. ICG fluorescence was detected using a charge-coupled device camera, which filters out light with a wavelength below 820 nm. 13 ICG fluorescence lymphography was performed on both feet for all participants.
Evaluation of injection-related pain
We used a TMD or 27G needle to inject the ICG solution. A TMD was used for one foot, and a 27G needle was used for the other. The leg (left or right) receiving the TMD injection was randomly selected, and participants were blinded to this during the injection. ICG was dissolved in a 5% glucose solution, and 0.1 mL of 0.5% ICG solution was injected at two points (the first web space and lateral border of the Achilles tendon) per foot. Injection-related pain was evaluated using the Numeric Rating Scale (NRS) 14 and Face Rating Scale (FRS), 15 and these values were compared between the TMD and 27G needles.
Evaluation of the injection depth
Human lower limbs were harvested after amputation due to critical limb ischemia and used in this study. ICG was dissolved in a 5% glucose solution, and 0.1 mL of 0.5% ICG solution was injected at each skin site immediately after lower limb amputation. A TMD or 27G needle was used to inject at 10 skin sites. The injected skin sites were excised from the surrounding subcutaneous and adipose tissues. The skin tissues were fixed in 10% formalin at room temperature for 24 hours and embedded in paraffin. Tissues were cut into 4-μm sections, and hematoxylin and eosin staining was performed.
To observe the depth of ICG injection, near-infrared fluorescence microscopy was performed 16 using an upright epifluorescence microscope (Eclipse 80i; Nikon Instruments, Inc., Tokyo, Japan) with a microscope near-infrared camera (Photometrics Evolve 512; Nippon Roper, Tokyo, Japan); ICG fluorescence filter (ICG-B-000, excitation wavelength 769 ± 20.5 nm, emission wavelength 832 ± 18.5 nm; Opto-Line, Tokyo, Japan); and 4′,6-diamidino-2-phenylindole (DAPI) fluorescence filter (excitation wavelength 375 ± 28 nm, emission wavelength 460 ± 60 nm; Nikon Instruments, Inc.). Fluorescence images were obtained with an antifade reagent (ProLong Gold antifade reagent with DAPI; Life Technologies, Japan, Tokyo, Japan) and an exposure time of 200 μs. Pseudocolor images were generated using a computer image analysis system (Lumina Vision version 3.0; Mitani Corp., Tokyo, Japan). The central depth of injected ICG solution range was measured using an image analysis system (Lumina Vision) for each skin sample.
Statistical analysis
NRS, FRS scores, and the central depth of injected ICG solution range are presented as the median and interquartile range. Differences in NRS or FRS scores between the TMD and 27G needles were compared using the Wilcoxon signed rank test. The difference in the central depth of injected ICG solution range was compared using the Wilcoxon rank sum test. A p-value of <0.05 was considered statistically significant. All analyses were performed using IBM SPSS version 25.0 software (IBM Corp., Armonk, NY).
Results
Volunteer characteristics
In total, 30 volunteers were enrolled in this study, of which 21 were men and 9 were women. The average age of the participants was 23.5 years (range 18–34 years), the average height was 1.68 m (range 1.56–1.81 m), the average weight was 62.6 kg (range 40–92 kg), and the average BMI was 21.9 kg/m2 (range 16.2–31.8 kg/m2).
The visualization for ICG fluorescence lymphography was similar using both needles (Fig. 1E). Collecting lymphatic vessels were easily visible from the feet to the knees.
Evaluation of injection-related pain
The NRS score was significantly different between the 27G needle and TMD groups (p = 0.017) (27G needle: 3 [3–4] vs. TMD; 2 [2–4]; Fig. 2A). The FRS score was also significantly different between the 27G needle and TMD groups (p = 0.021) (27G needle: 2 [2–3] vs. TMD; 2 [1–2]; Fig. 2B).

Comparison of injection-related pain between two types of needles. Injection-related pain during ICG fluorescence lymphangiography is compared using the
Evaluation of injection depth
The injected ICG solution appears red on fluorescence microscopy (Figs. 3 and 4). Using 27G needles, the depth of ICG solution ranged from the dermis to the subcutaneous area (Fig. 3). The injection depth varied from 400 to 1200 μm and was different for each injection using a 27G needle. In contrast, the depth of ICG injection was observed mainly between 300 and 700 μm from the skin surface using a TMD (Fig. 4). Figure 4 shows that the injection depth was consistent when using the TMD. The range of the central depth of injected ICG solution was significantly different between the 27G needle and TMD groups (p = 0.029) (27G needle: 525.8 [517.6–889.6] vs. TMD; 428.9 [425.4–441.4]; Fig. 5).

Fluorescence microscopy of ICG-injected skin using a traditional 27G needle. ICG solution was injected using a traditional 27G needle, and skin samples were obtained. Fluorescence microscopy of the skin samples. Red: ICG, Blue: DAPI. Hematoxylin and eosin staining of skin samples. The depth of the injected ICG solution differed for each sample. Scale bar: 100 μm. DAPI, 4′,6-diamidino-2-phenylindole.
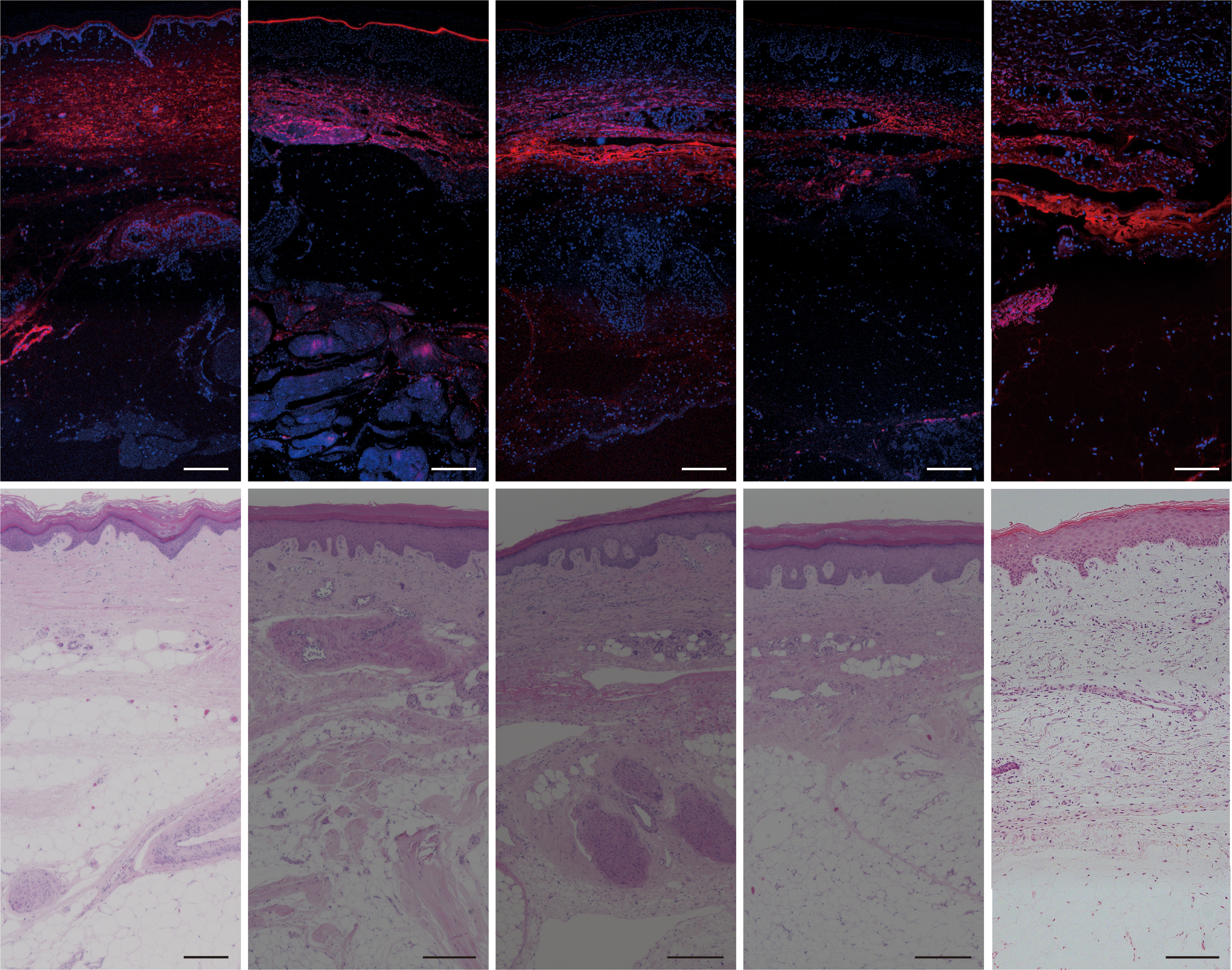
Fluorescence microscopy of ICG-injected skin using a TMD. ICG solution was injected using a TMD, and skin samples were obtained. Fluorescence microscopy of the skin samples. Red: ICG, blue: DAPI. Hematoxylin and eosin staining of skin samples. The depth of the injected ICG solution was kept constant for each sample. Scale bar: 100 μm.
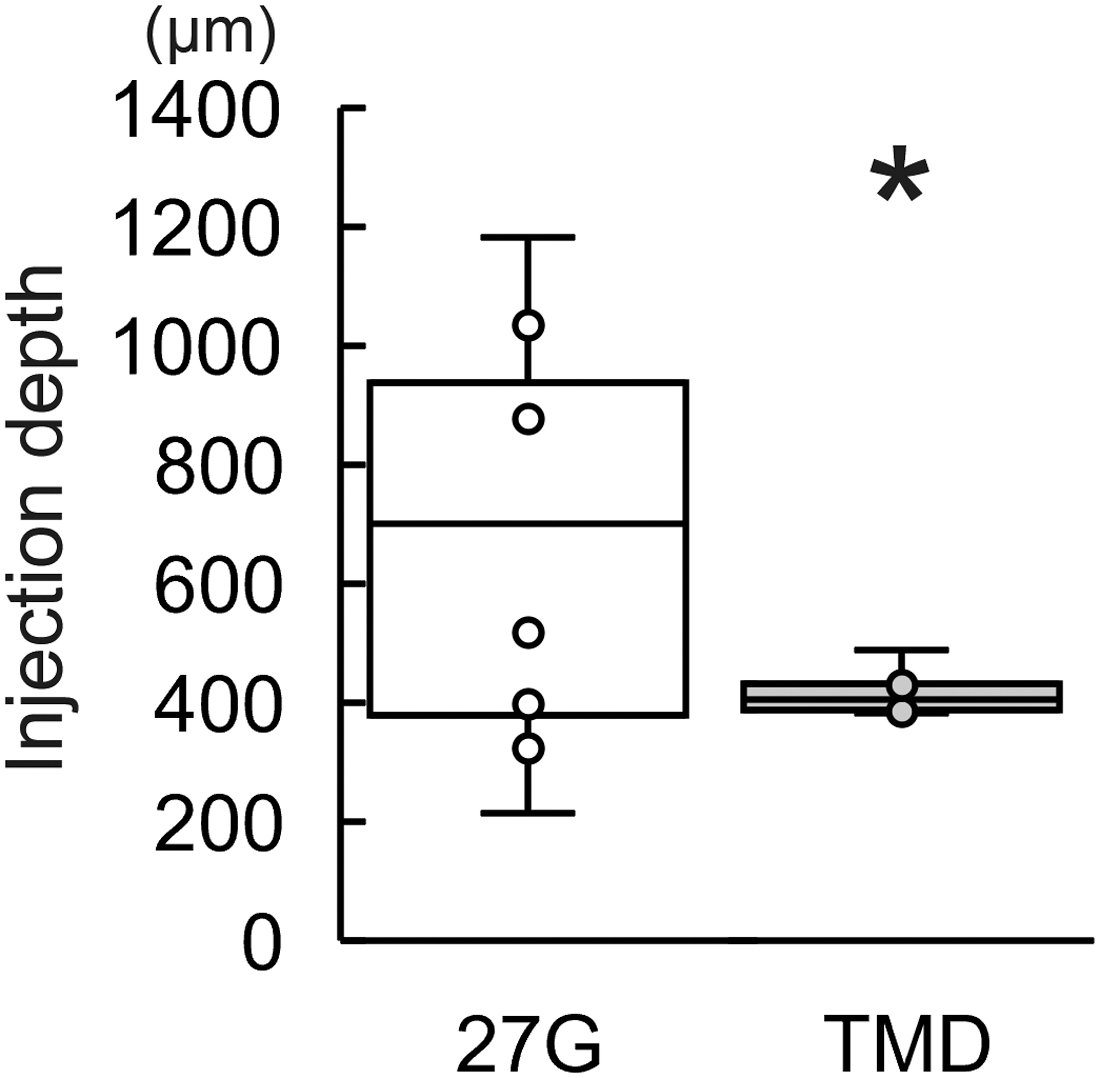
Comparison of injection depth of ICG solution between two types of needles. The central depth of the injected ICG solution range was measured, and the median was compared using a traditional 27G needle and a TMD. *p < 0.05.
Discussion
In this study, we showed that using a TMD in fluorescence lymphography reduced injection-related pain and enabled the injection of the ICG solution at a consistent depth. Injection-related pain consists of needle insertion and infiltration pain and is recognized by cutaneous nociceptors. 17 Cutaneous nociceptors are important warning systems that activate two types of nerve fibers: A-δ and C-fibers. 17 A-δ fibers are associated with sharp pain, whereas C-fibers are associated with dull pain. 15 Needle insertion activates A-δ fibers and causes sharp pain, whereas infiltration of the solution activates C-fibers and causes dull pain.17,18 Several approaches have been reported to minimize injection-related pain.10,17,18
To minimize needle insertion pain, a smaller diameter needle, 19 perpendicular insertion, 20 and tactile distraction are recommended. 17 Other stimuli, such as pressure or touch, are perceived near the insertion area close to the pain gate by the A-δ fibers.21,22 Therefore, skin stimulation by pinching, stretching, or pressing near the needle insertion sites reduces needle insertion pain. 23 This “tactile distraction” is especially effective in areas with loose skin, which can be easily pinched. 17 However, tactile distraction is difficult to use during ICG fluorescence lymphography since ICG solution is often injected at the tips of extremities, such as the feet or hands, which have tight skin.
Needle insertion pain is also minimized by perpendicular insertion. 20 The nerve fibers with endings for pain are similar to those of leaves on a tree. 17 The inserted needles can pass through dull pain fibers through perpendicular insertion. 21 Perpendicular insertion reduced needle insertion pain compared with 45° insertion during local anesthesia. 20 Based on these reports, we considered that using a smaller diameter needle and perpendicular insertion might effectively minimize needle-insertion pain during ICG fluorescence lymphography. A TMD with 34G needles is inserted perpendicularly and might be an ideal device for ICG fluorescence lymphography. In fact, we observed lower injection-related pain with a TMD than that with traditional 27G needles in this study.
To minimize infiltration pain, adjustment of the injected solution, stabilization of the syringe, and slow injection have been recommended. 17 In this study, stabilization of the syringe and slow injection were performed similarly for both needles. Adjusting the solution's pH and osmotic pressure ratio is important for minimizing infiltration pain. 24 According to the literature, adjusting pH to a physiological pH of 7.425,26 and osmotic pressure ratio to 1.0,27,28 as well as injecting a small amount of solution, 18 minimizes infiltration pain. In a previous report, an ICG solution at 0.25%–0.5% concentration and 0.05–0.3 mL per injection site was used for fluorescence lymphography.29–33
Sterile distilled water, 34 physiological saline, 35 or 5% glucose solution 36 was used as a solvent for the ICG solution. Although we did not evaluate which solvent was better to adjust the ICG solution and minimize infiltration pain, the adjusted ICG solution may result in improved tolerance to infiltration pain. On dilution of the ICG in sterile distilled water, the osmolarity is very low, 37 and infiltration pain may consequently be high. The pH and osmotic pressure ratio in the 0.5% ICG solution are similar to those in physiological saline (pH: 7.15, osmotic pressure ratio: 1.02) and a 5% glucose (pH: 6.64, osmotic pressure ratio: 0.935) solution. 37 However, the absorbance spectra are higher in the ICG in a 5% glucose solution compared with that in physiological saline. 37 Therefore, the ICG in a 5% glucose solution might have high fluorescence intensity and low infiltration pain.
Further studies are needed to investigate the ideal adjustment of the ICG solution to minimize infiltration pain and impact on fluorescence findings.
In previous studies, local anesthetic injection,29,32 mixing ICG with a local anesthetic agent, 10 or using a cryogenic numbing device 10 has been suggested to minimize injection-related pain during ICG fluorescence lymphography. These methods might be useful; however, there are concerns about side effects of the anesthetic agent or device cost. Visconti et al reported that injection-related pain was scored from 8 to 10 for the injection of the ICG solution without a local anesthetic agent group and from 1 to 3 for that with a local anesthetic agent group on a visual analog scale. 9
In this study, the median of NRS and FRS was 2 in the TMD group. Thus, we achieved pain reduction only using TMD and adjusting the ICG solution without a local anesthetic agent. Local anesthesia has a vasodilation effect and may impact the lymphatic uptake. In addition, the uptake of anesthesia into lymphatic vessels may compete with the uptake of the ICG solution. The effect of local anesthesia during ICG lymphography remains unknown.
Only the lymphatic vessels in which ICG solution is drained or pooled are visible in ICG fluorescence lymphography. 6 Therefore, not only is it important to reduce injection-related pain, but also to inject enough ICG. The ideal amount of ICG has not been determined and remains controversial. Diffusion of ICG solution is also important for visualizing lymphatic vessels. 6 Extensive ICG diffusion might enable the observation of more lymphatic vessels. The TMD has circularly arranged needles with the bevel angle facing outward; this enables the simultaneous injection of the same amount of solution through the three needles. 11 These factors contribute to a larger and more homogeneous diffusion area compared with a conventional needle. 11
Ishikawa et al reported that the volume of anesthetics is significantly lower with a TMD compared with conventional needles with the same range of local anesthesia owing to the greater diffusion with a TMD. 12 Hence, the ICG solution might diffuse more using a TMD than using conventional needles, and using a TMD might be useful in the diffusion of ICG solution during fluorescence lymphography.
The thickness of the skin in the human lower extremities is ∼1200 μm, 38 and lymphatic vessels form networks in the skin at a depth of 250–1000 μm. 39 In this study, we showed that a TMD allows the injection of ICG solution to a stable skin depth, and that the injection depth ranges from ∼300 to 700 μm using a TMD. According to the literature38,39 and our results, a TMD may enable the injection of a ICG solution to a stable depth, at which lymphatic vessels form networks.
ICG fluorescence lymphography is less invasive than direct lymphography 5 ; therefore, it is often repeatedly performed for follow-up or to evaluate changes in lymphatic function over time by treatment. However, the findings of ICG fluorescence lymphography are influenced not only by lymphatic function but also by other factors such as the illuminance of the experimental room, distance between the emitting light and skin, brightness of the emitting light, performance of the camera system, amount of injected ICG, and the location of the injected site.6,29 The injection depth of ICG solution might also influence the findings of ICG fluorescence lymphography. It is desirable to minimize the above factors and perform ICG fluorescence lymphography under the same conditions to evaluate changes in lymphatic function over time. A TMD enables the injection of ICG solution to a stable skin depth and may be useful for performing ICG fluorescence lymphography under the same conditions.
This study has some limitations. First, it was difficult to compare the fluorescence images between the TMD and 27G needles on the same foot, as the fluorescence of ICG persisted for ∼1 month. Second, the obtained human skin samples were derived from amputated limbs with critical limb ischemia and might not have the same qualities as skin from healthy limbs. Third, this study was performed on healthy volunteers with normal lymphatic function. In lymphedema patients, the skin condition changes with skin fibrosis, 40 increased adipose tissues, 41 and decreased skin elasticity. 42 Changes in the skin condition might influence the injection depth. Further studies are needed to adjust the ideal ICG injection to enhance its usefulness in lymphedema patients. Future studies can be designed to overcome such limitations to determine the efficacy of using TMDs over conventional 27G needles.
Conclusions
We demonstrated the usefulness of a TMD during ICG fluorescence lymphography. The TMD enabled the reduction of injection-related pain during fluorescence lymphography and injection of ICG solution at a stable depth.
Footnotes
Acknowledgments
We thank Ms. Yayoi Kawabata and Ms. Naomi Suzuki (Hamamatsu University School of Medicine) for their technical assistance. We would like to thank Editage for English language editing.
Authors' Contributions
Y.E., M.S., T.K., and T.S. conceived and designed the study. Y.E., M.S., T.K., T.S., K.K., Y.Y., H.Ts., N.I., and E.N. acquired the data. Y.E., M.S., T.K., and T.S. analyzed and interpreted the data. Y.E. and M.S. wrote the article. K.I., H.Ta., and N.U. supervised this project. All authors critically revised and approved the article and agreed to be accountable for all aspects of this work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by JSPS KAKENHI (grant number 15K21052 awarded to Masaki Sano and grant number 21K16493 awarded to Takafumi Kayama).