
Abstract
Objective:
The occurrence of breast cancer-related lymphedema (BCRL) in postoperative breast cancer survivors is described and the independent risk factors of BCRL are analyzed. A BCRL nomogram prediction model is constructed, and its effectiveness is evaluated to screen out high-risk patients with BCRL.
Methods:
A univariate analysis was carried out to determine the risk factors possibly related to BCRL, and a logistic regression analysis was utilized to determine the independent risk factors related to BCRL. A BCRL nomogram prediction model was built, and a nomogram was drawn by R software v4.1.0. The area under the curve (AUC) of the receiver operating characteristic (ROC) and the Hosmer–Lemeshow test were used to evaluate the efficacy of the constructed model to assess its clinical application value.
Results:
The risk factors independently associated with BCRL were body mass index (BMI), handedness on the operation side, no BCRL-related rehabilitation plan, axillary lymph node dissection (ALND), taxane-based chemotherapy, and radiotherapy (all p < 0.05). The BCRL nomogram prediction model was built on this basis, and the results of the efficacy evaluation showed a good fit: AUC = 0.952 (95% confidence interval: 0.930–0.973) for the ROC and χ2 = 6.963, p = 0.540 for the Hosmer–Lemeshow test.
Conclusions:
The risk factors for BCRL included higher BMI, handedness on the operation side, no BCRL-related rehabilitation plan, ALND, taxane-based chemotherapy, and radiotherapy. In addition, the BCRL nomogram prediction model accurately calculated the risk of possible BCRL among breast cancer survivors and effectively screened for high-risk patients with BCRL. Therefore, this prediction model can provide a basis for rehabilitation physicians and therapists to formulate early and individualized prevention and treatment programs.
Introduction
Breast cancer is one of the most common malignant tumors in females, and its incidence rate has increased rapidly in recent decades. As treatment technology and in-depth research have developed, the cure rate of breast cancer and patients' overall survival rates have increased. Breast cancer-related lymphedema (BCRL), one of the complications caused by breast cancer and its treatment, is a chronic lymphatic system disorder that can initially occur in the 1st month after breast cancer surgery and increases in incidence over time; nearly 80% of BCRL diagnoses occur within 3 years of surgery. There is significant heterogeneity in the incidence of BCRL, ranging from 5.6% to 63.4%, depending on factors such as intervention modality, means of monitoring and duration of follow-up treatment. 1
The onset of BCRL is usually hidden until the patient notices subtle signs of swelling. Although arm swelling itself is not life-threatening, it can lead to symptoms such as heavy numbness, stiffness, limited movement, and repeated limb infection. It may also cause negative emotions, which can seriously affect the patient's quality of life (QoL). 2 The QoL of BCRL patients is significantly lower compared with non-BCRL patients, especially in terms of physical function and social psychology. 3 The more distressing symptoms of lymphedema (heaviness, numbness, tightness, increased skin temperature, or skin reddening) are always accompanied by a worse QoL. 4 Therefore, to avoid the development of BCRL and to maximize the QoL of patients and their families, clinical medical staff should increase their early identification skills of BCRL risk factors, symptoms, and signs and pay attention to the early detection, screening and primary prevention of BCRL.
However, there is still no reliable method to distinguish high-risk BCRL patients. Studies have reached a consensus on some risk factors of BCRL, such as axillary lymph node dissection (ALND),5,6 radiotherapy (especially regional lymph node radiotherapy),6,7 higher body mass index (BMI),8,9 and the number of lymph nodes removed.10,11 Other risk factors that may be related to BCRL, such as age,12,13 whether patients have received rehabilitation education on BCRL-related risk factors and preventive measures, 14 chemotherapy (especially taxane-based chemotherapy),15,16 hypertension,17,18 postoperative inflammatory infection (e.g., cellulitis, chest infection),19,20 and genetic susceptibility, 21 have yielded less consistent results in different studies.
Multiple factors contribute to the occurrence of BCRL, including local and systemic treatment schemes, the ability of patients to form collateral lymphatic pathways after injury, and potentially changeable risk factors. Therefore, it is of great significance to identify the risk factors of BCRL for its early prevention, treatment, and rehabilitation. Multiple risk factors may occur in patients at the same time, so it is impossible to speculate on the occurrence of BCRL only by single or individual factors. 22
Therefore, a rehabilitation medical team can better predict and identify high-risk patients by establishing an evidence-based BCRL prediction model that integrates multiple variables to estimate an individual's risk as a single value. This study investigates and analyzes the risk factors of BCRL in postoperative breast cancer survivors and builds a nomogram prediction model to screen out the high-risk patients for BCRL after breast cancer surgery. This study's goal is to provide a more appropriate and individualized postoperative rehabilitation treatment plan, as well as make early prevention and intervention measures available to reduce the occurrence of BCRL.
Methods
Data collection procedures
A total of 345 unilateral, single-focus female patients with breast cancer were selected for this study, who were treated from January 2014 to March 2021, in two tertiary hospitals in Hebei province. Of those 345 patients, 42 were excluded according to the exclusion criteria. Therefore, a total of 303 patients were included, with an effective rate of 87.83%. Inclusion criteria were as follows: (1) Patients were able to complete the questionnaires; (2) the diagnosis of unilateral and single-focus breast cancer was confirmed by pathology, and the patient underwent an operation for it within 3 months of diagnosis; and (3) informed consent was given. Exclusion criteria were as follows: (1) The patient had local or systemic infection; (2) trauma and other critical diseases; and/or (3) other malignant tumors or serious chronic diseases in the past. This study was approved by the ethics committee of Hebei General Hospital (Approval ID: 2022060).
Analytic variables
All participants were required to complete a unified questionnaire23,24 that included the following information: General patient data (age, follow-up time, height, weight, whether the side operated on was the patient's dominant side, daily physical exercise status, and last year's annual family income); disease data (whether there were postsurgical infection events, whether the patient received BCRL-related rehabilitation education, whether they have high blood pressure, and whether they have diabetes); and whether the difference between the arm circumferences of the five positions of the upper limbs was >2 cm (for patients surveyed in person, the investigators used the same tape measure to measure and record the patients' arm circumferences at the five positions of the upper limbs.
For the patients interviewed by telephone and WeChat, the investigators trained the patients or their families to measure the patients' arm circumferences at the five positions of the upper limbs before they left the hospital to standardize the process. The tapes utilized were bought by centralized purchasing and given out in the hospital, and if needed, the patients or their families did the measurements at home. Patients with any arm circumference difference exceeding 1.5 cm were required to go to the hospital for in-person measurement).
The investigators carefully consulted the patient's electronic medical records to complete the treatment information, including the type of surgery, axillary lymph node management, lymph node metastasis grade and the use of sentinel lymph node biopsy, radiotherapy, postoperative chemotherapy, taxane-based chemotherapy, endocrine therapy, and targeted therapy.
Evaluation of BCRL events
Patients diagnosed with breast cancer underwent an in-hospital arm volume measurement using a perometer, with each patient having their preoperative baseline and lymphedema quantified. The process of diagnosis of lymphedema by arm circumference measurement was as follows: A soft ruler was used to measure the arm circumference at five positions of both upper limbs (at the ulnar styloid process and at 10, 20, 30, and 40 cm above the ulnar styloid process). Whether it is was at home or in the hospital, three replicated measurements were taken, and any difference between the affected side and the healthy side of >2 cm was diagnosed as lymphedema. 25 If the patients received measurements at home, any arm circumference difference exceeding 1.5 cm required the patient to go to the hospital for in-person measurement.
Statistical analysis
All data were organized and statistically analyzed using SPSS 22.0 software. Continuous data, in accordance with normal distribution, were presented as the mean ± standard deviation (x̄ ± SD). Categorical variables were summarized as frequencies and percentages. A chi-square test and Mann–Whitney U test were used to conduct the between-group comparisons. Univariate and multivariate logistic regression analyses were used to select the predictive features from the primary cohort. Candidate variables with significance (p < 0.05) under the univariate analysis were selected and input into the multivariate analysis model using stepwise logistic regression.
The nomogram for predicting BCRL was drawn by R Software v4.1.0 and was constructed based on the independent risk factors that resulted from the multivariate logistic regression analysis. A receiver operating characteristic (ROC) curve was drawn, and the area under the curve (AUC) value was calculated to measure the discrimination of the BCRL nomogram. There is a positive correlation between the AUC and prediction accuracy: An AUC value <0.7 is judged to have no clinical application value, a value of 0.7–0.8 is determined to have a certain value, and a value above 0.8 indicates that the model has good prediction accuracy and good clinical application value. 26
The Hosmer–Lemeshow goodness-of-fit test was used to verify the agreement between the actual probability of BCRL occurrence in patients and the predicted probability of BCRL occurrence in the model. In the Hosmer–Lemeshow χ 2 goodness-of-fit test, a p value of >0.05 indicated that the predictive calibration was good.
Results
Characteristics of the primary and validation cohorts
The mean duration of disease in the 303 patients with complete data, who met the inclusion criteria, was 25.15 (3–82) months, and the mean age was 49.46 (20–76) years. Regarding diagnoses, 154 (50.83%) patients had lymphedema and 149 (49.17%) patients did not have lymphedema. Nineteen factors in general demographic data, in clinical data, and in the univariate analysis results of the two groups were determined as possibly associated with the occurrence of BCRL and were entered into the multivariate analysis (Tables 1 and 2). Most of these factors were related to the breast cancer diagnosis and the resulting surgery and therapy. The other factors were related to the disease and disease history of patients (e.g., diabetes demonstrated whether patients had diabetes or its complications, and cardiovascular disease indicated that the patients had coronary heart disease or arterial disease).
Comparison of Demographic Data of Research Subjects Between Different Groups
Note: p < 0.05 is considered statistically significant.
BMI, body mass index; RMB, China's legal tender.
Comparison of Clinical Data of Subjects in Different Groups
Note: p < 0.05 is considered statistically significant.
ALND, axillary lymph node dissection; BCRL, breast cancer-related lymphedema; SLNB, sentinel lymph node biopsy.
In the multivariate analysis, six factors were identified as independent predictors of BCRL (p < 0.05). A significant increase in the risk of developing BCRL was found in women with a higher BMI and who had surgical treatment on their dominant side, ALND, taxane-based chemotherapy, or radiotherapy. A decreased risk of developing lymphedema was found in those who had received BCRL-related rehabilitation education. The specifics of the predictors of BCRL are presented in Table 3.
Results of Multivariate Logistic Regression Analysis of Risk Factors for Breast Cancer-Related Lymphedema
Note: p < 0.05 is considered statistically significant.
CI, confidence interval; OR, odds ratio; SE, standard error.
Development and validation of the BCRL nomogram
A model incorporating the above independent predictors was developed and presented as the nomogram (Fig. 1). A total point is the sum of all points for each variable, and the probability of BCRL is the corresponding number of the total points in the nomogram. Rows 2 through 7 represent the variables. A vertical line is drawn between each variable and the points' axis to determine the effect of each variable by a defined number of points, which is then summed and placed in row 8 (total points). A vertical line should be made between rows 8 and 9 (risk of lymphedema) to obtain the predicted probability of BCRL.
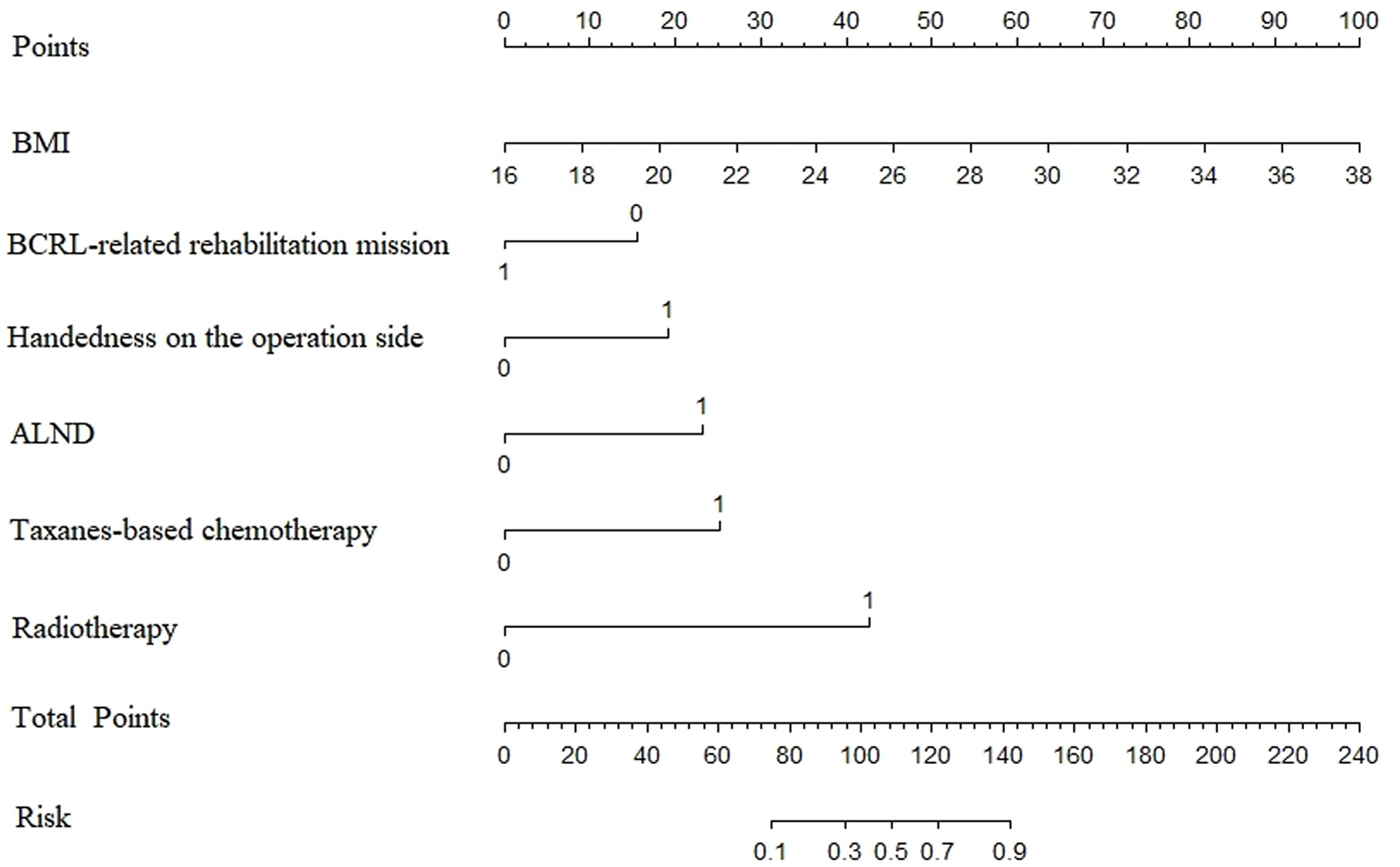
Nomogram for predicting the probability of lymphedema. Note: 0 = No and 1 = Yes. ALND, axillary lymph node dissection; BCRL, breast cancer-related lymphedema; BMI, body mass index.
For example, a female patient with breast cancer who was postoperative had a BMI of 26, no BCRL-related rehabilitation plan, dominant handedness on the operative side, no ALND, and no taxane-based chemotherapy, but did undergo radiotherapy, had a nomogram score of 45 + 15 + 19 + 0 + 0 + 42.5 = 121.5, and predicted risk of lymphedema of 70% (Fig. 2).
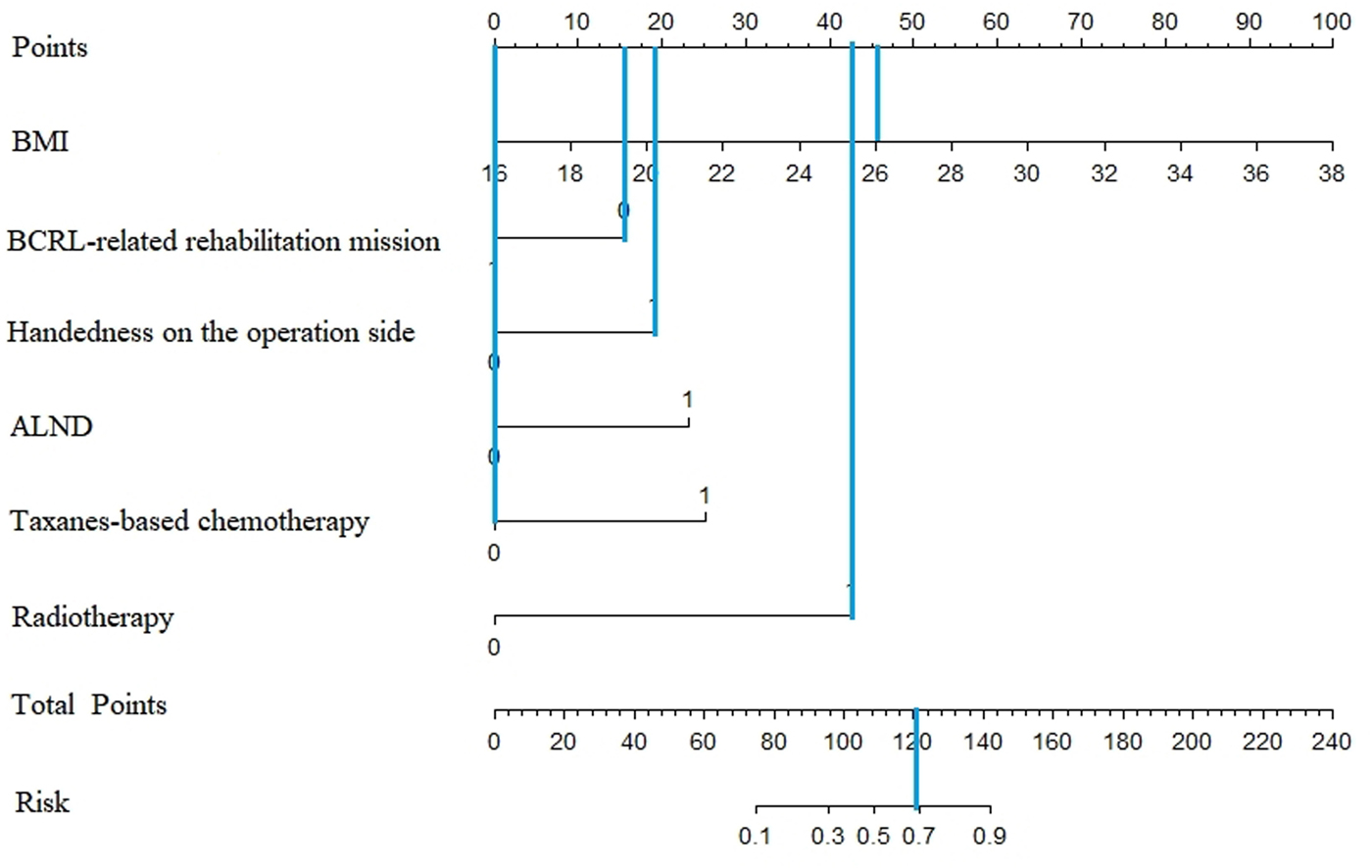
An example diagram of the nomogram for predicting the risk of BCRL.
The ROC curve for BCRL screening was obtained by assigning a value of 0 to “no BCRL” and a value of 1 to “BCRL” using the total score of the nomogram as the test variable and the total score of the occurrence of breast cancer survivors as the status variable (Fig. 3). The AUC for the nomogram in the primary cohort was 0.952 (95% confidence interval [CI]: 0.930–0.973), corresponding to a cutoff value of 0.490, a specificity of 91.9% and a sensitivity of 86.4%. The test results showed a good fit by the Hosmer–Lemeshow goodness-of-fit test: χ 2 = 6.963, p = 0.540.
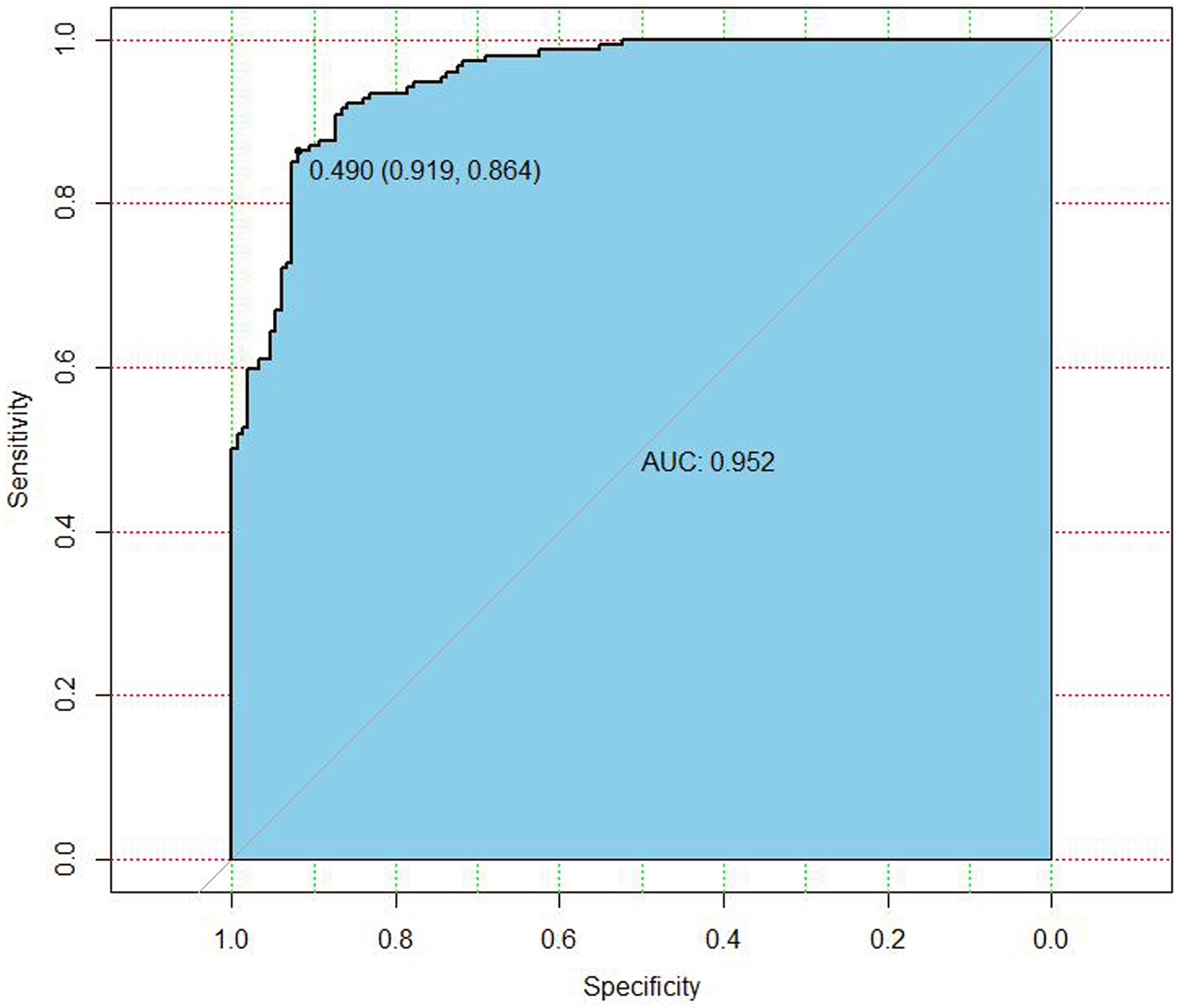
The receiver operating characteristic curve for nomogram in predicting the risk of BCRL. AUC, area under the curve.
Discussion
This study found that the prevalence of BCRL in breast cancer survivors was 50.83% in the primary cohort, which is higher than that reported in previous studies; this discrepancy may be explained by differences in the monitoring mean. 27 The arm circumference measurement method used in this study, although a portable and easy-to-perform diagnostic method, may be affected by right and left limb dominance, muscle strength, fibrous tissue deposition, or weight changes, resulting in differences in its sensitivity. However, it still reflects overall trends.
A univariate analysis was performed on the general, disease, and treatment data of patients, and then a multivariate logistic regression analysis was carried on the factors with statistical significance (p < 0.05). Finally, six independent risk factors of BCRL were determined (p < 0.05): Higher BMI, operation on the dominant side, no BCRL-related rehabilitation plan, ALND, taxane-based chemotherapy, and radiotherapy. Two predictors that have been less well studied in previous studies were included and found: Dominant handedness on the surgical side and no BCRL-related rehabilitation education.
There is a difference in the functions performed by the dominant and nondominant sides in daily life, and this study found that the risk of BCRL was 3.351 times higher for those who had surgery performed on their dominant side (95% CI = 1.453–7.728; p = 0.005). This is consistent with the results of Mayrovitz et al., 19 who found that dominant-side surgery was associated with moderate to severe lymphedema. In addition, the incidence of dominant-side lymphedema was found to be 18% in a study by Ivens et al. 28 compared with 2% on the nondominant side. The reason for this may be the obstruction of the axillary lymphatic reflux due to surgery.
If the operation side is dominant, patients will habitually, inadvertently, and frequently use that side in their daily life and work (e.g., scrubbing, pushing and pulling, cooking and lifting). These activities can easily induce lymphedema of the affected limb or aggravate the symptoms. The “Guidelines and Norms for Breast Cancer Diagnosis and Treatment of the Chinese Anti-Cancer Association (2021 Edition),” proposed by the Breast Cancer Professional Committee of the Chinese Anti-Cancer Association, clearly states that the above activities should be avoided with the affected limb, which also suggests that rehabilitation medical staff should strengthen their education of patients on preventive behaviors to enhance their awareness of protecting the affected hand and avoid excessive use of the affected hand in their daily activities to prevent the occurrence of BCRL. 29
Early recovery education and risk management education for patients have been shown to reduce the incidence and severity of lymphedema in cancer survivors.14,30 This study found that the incidence of lymphedema in patients who had received BCRL-related rehabilitation education was 41.38%, while that in patients without rehabilitation education was 70%. The multivariate analysis revealed that whether they had received rehabilitation education was an independent risk factor for the occurrence of BCRL (odds ratio = 0.332; 95% CI = 0.128–0.865; p = 0.024).
Similar conclusions were reached by Zhang; they found that the level of patient awareness of the disease and the implementation of preventive measures were associated with the occurrence of BCRL. 31 In addition, many women in Deveci et al.'s study received a plan from the rehabilitation medical team, and they found that patients who received a BCRL rehabilitation plan had higher self-care practice scores and a correspondingly lower incidence of lymphedema than those who did not. 32 In the study by Ridner et al., 33 65% of patients believed that self-care education during BCRL treatment was effective, and it was found that most of the BCRL population wanted further lymphedema education. 34
Therefore, it is believed that the gap in lymphedema management may be attributed, in part, to the lack of patient awareness of BCRL self-care and the implementation of preventive behaviors. 35 Patients should receive lymphedema education in a timely manner during preoperative and postoperative rehabilitation visits, and it needs to be included in the patient's care plan, which should be implemented not only by rehabilitation physicians, nurses, and physical therapists but also by medical and nursing staff from the breast surgery and radiation therapy departments. One of the goals of lymphedema rehabilitation outreach should focus on improving the ability of the rehabilitation team to make appropriate referrals and communicate with other specialists in a multidisciplinary approach to improve outcomes in the management of lymphedema.
Since the occurrence of diseases is usually the result of the interaction of multiple etiologies, statistical models can be established to predict the probability of a certain clinically relevant outcome or event occurring in the future in a population with certain characteristics. Based on this study's multivariate logistic regression analysis results, a BCRL nomogram prediction model was established, which converted complex risk factor indicators into simple numerical values and carried out personalized analysis and prediction of clinical events. This model realized a visualization and analysis of regression analysis results.
Graphically, it can effectively predict the risk of BCRL in patients and provide a basis for patients to receive more appropriate and timely rehabilitation guidance. 36 The postevaluation of efficacy revealed that the AUC of the ROC curve was 0.952, the 95% CI was 0.930–0.973, the Hosmer–Lemeshow test results were χ 2 = 6.963 and p = 0.540, and the fit was good. These results suggest that this nomogram has good prediction accuracy regarding the probability of future BCRL in cancer survivors, can screen out high-risk patients with BCRL and can provide a reference for the rehabilitation medical team. This will allow the development of early, effective, and individualized prevention and treatment plans.
In 2012, BeviLacqua et al. 37 constructed three nomogram prediction models: Before surgery (Model 1), within 6 months after surgery (Model 2), and more than 6 months after surgery (Model 3). These models could calculate and predict the incidence of BCRL in breast cancer patients at different periods. They were later validated for accuracy, and it was found that their predictive properties were good. The above models were subsequently externally validated by domestic researchers,38,39 and it was found that the accuracy and applicability of the BeviLacqua-2 nomogram prediction model (within 6 months postoperatively) were high for Chinese breast cancer patients, but its predictiveness for patients beyond 6 months postoperatively remains to be validated.
Byun et al. 40 applied the same method to construct nomograms of lymphedema probabilities at 2, 3, and 5 years after breast cancer surgery, which was later validated internally and externally and demonstrated good calibration and discrimination. This team recently conducted external validation on 1377 Asian patients, 22 and the results suggest a good predictive accuracy; however, its applicability to Chinese breast cancer patients remains to be investigated. As global attention on rehabilitation increases, there is a need to focus not only on the treatment of the disease itself but also on the early prevention and intervention of possible complications, such as prevention education, regular follow-up appointments, and effective monitoring.
The above two prediction models only explored the risk factors associated with oncologic treatment. They did not explore the effect of postoperative-related preventive and interventional behaviors and whether the development of BCRL is one sided. This study found that having received a BCRL rehabilitation plan was effective in avoiding lymphedema, and whether a patient received rehabilitation education was included in the construction of the nomogram. This study's nomogram had slightly better predictive accuracy than the previous nomograms when internal validation was checked; therefore, the nomogram constructed in this study may reflect modern breast cancer treatment protocols.
Dou 41 constructed a nomogram for the occurrence of lymphedema in Chinese breast cancer patients, and although it included patients' implementation of preventive behaviors, the population was limited to 1 year after surgery. However, the incidence of BCRL is 75% within 1 year and 80% within 2 years after surgery. 42 Thus, it is not effective to limit the follow-up population to only 6 months or 1 year after surgery. The follow-up time span in this study was longer (3–82 months after surgery), with a mean of 25.15 months, which is more representative and applicable to a wider population.
Limitations
This study has some methodological limitations. First, this is a retrospective study, and the accuracy of the information depends on the electronic medical record system and descriptions from the patients. Since the electronic medical records were completed by different clinicians, and the patients' measurements of bilateral arm circumferences of both upper extremities may be inaccurate, this study may be affected by information bias. Although the patients and their families were trained, it is hard to completely avoid a measurement deviation. Second, the BCRL nomogram prediction model constructed in this study had a small sample size and has not yet been externally verified. Therefore, it is necessary to increase the sample size and perform external validation to test the predictive efficacy of this model in future studies.
Conclusions
The six confirmed risk factors for BCRL are higher BMI, surgery performed on the dominant side, no BCRL-related rehabilitation plan, ALND, taxane-based chemotherapy, and radiotherapy. A BCRL nomogram prediction model was built to accurately calculate the risk of BCRL among breast cancer survivors to screen out high-risk patients for BCRL. This can provide a basis for rehabilitation physicians and therapists to formulate early and individualized prevention and treatment programs.
Footnotes
Acknowledgments
The authors thank all the women who participated in the study and the following institution for their assistance in collecting the data: Hebei General Hospital, The Fourth Hospital of Hebei Medical University.
Authors' Contributions
Conceptualization: H.L. Methodology: W.B.L., Z.X.S., and J.Y. Data collection: P.Y.L., C.X.L. and X.L. Formal analysis and investigation: Y.Y. and Z.B.Z. Writing-original draft preparation: H.L. and Z.B.Z. Writing-review and editing: All authors read and approved the final article.
Data Availability
The datasets generated during and/or analyzed during this study are available from the corresponding author on reasonable request.
Code Availability
The statistical analyses were conducted using SPSS 22.0 and R software version 4.1.0.
Ethics Approval
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Heibei General Hospital. Written informed consent was obtained from all participants. Ethics Approval NO.: 2020060.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This study was funded by 2018 government subsidized specialist capacity building and specialist leader training (specialist leader): Application of comprehensive detumescence therapy in the recovery of upper limb lymphedema after breast cancer surgery (No: 361003) and Application of manual lymphatic drainage combined with low-elasticity bandages in lymphedema after breast cancer surgery (project number: G2019076)-Hebei Province Medical Applicable Technology Tracking Project.