
Abstract
Background:
Learning self-care for lymphedema is essential for patients to maintain their quality of life; however, it is sometimes difficult and stressful. There are only few studies about the psychological changes in patients hospitalized for conservative therapy. The purpose of this study was to evaluate the psychological changes in patients admitted for conservative therapy and training in self-care for lymphedema.
Methods and Results:
Nine patients who were hospitalized for conservative treatment of lymphedema of the lower limbs were administered the Profile of Moods States questionnaire twice: day of admission or the following day and after 5 days of hospital stay. Eight female patients and one male patient were included in this retrospective study. The mean age was 67.2 years. We provided standard compression therapy, manual lymph drainage, and exercise therapy to the patients. The Profile of Moods States 2nd edition, Japanese version of the Profile of Moods States, was used as an evaluation method of the psychological state. The results of the psychological tests were evaluated by a certified public psychologist. The scores for negative mood (anger or hostility, confusion or bewilderment, depression or rejection, fatigue or inertia, and tension and anxiety) were all lower on the fifth day of hospitalization compared with those at admission. In particular, the tension or anxiety scores decreased significantly (p = 0.019). However, the vigor or activity scores tended to increase.
Conclusions:
It was found that inpatient conservative therapy for lymphedema had a positive effect on the psychological state of the patients. Despite stressors such as a change in environment and introduction of new treatments (compression therapy and exercise therapy), the improvement in edema helped elevate the mood of the patients by the fifth day of hospitalization.
Introduction
Lymphedema is a disease in which lymph accumulates in the subcutaneous adipose tissue. Complete decongestive treatment, including compression therapy, manual lymph drainage (MLD), and exercise with compression therapy, is a standard treatment.1,2 When the improvement is insufficient, various surgical treatments are performed.3–7 There is no curative treatment for lymphedema yet, and self-care by the patients themselves is important for maintaining quality of life (QOL).8–10 When training in self-care is difficult through outpatient clinics, patients may be hospitalized for self-care guidance.
The first phase in the conservative treatment for lymphedema is intensive care to achieve volume reduction. After the edema improves and the volume of the affected limb is decreased, maintenance care is provided in the second phase. The duration required to reach the second phase varies from patient to patient. The length of hospitalization in our hospital can be as long as 1–4 weeks. Long-term hospitalization and the introduction of new treatments can put a strain on the patient's psychological state, and it is often difficult to determine how much burden of self-care can be tolerated by the patients. In our experience, some patients start to complain about fatigue or anxiety 5–7 days after hospitalization. There are also reports that surgical treatment for lymphedema improves QOL and mental health.11,12 However, so far, few studies have examined the psychological changes in patients hospitalized for conservative therapy.
In this study, we used a simple questionnaire to assess the psychological changes in patients admitted for the purpose of conservative therapy and training in self-care for lymphedema. This tool can help predict psychological changes in hospitalized patients as well as those receiving outpatient self-care training and, therefore, improve the success rate of the treatment. The purpose of this study was to evaluate the psychological changes in patients admitted for conservative therapy and developing self-care skills in the management of lymphedema.
Methods
Seventeen patients who were hospitalized for conservative treatment of lymphedema of the lower limbs, from November 2020 to July 2021, underwent psychological evaluation using a questionnaire, the Profile of Mood States (POMS). Among them, nine were administered the POMS questionnaire twice. The first POMS was to evaluate the psychological state at the time of admission and performed on the admission day or next day, and the second POMS was to evaluate mood changes after the treatment progressed, which was evaluated after the fifth day. The other eight were excluded because they took the POMS test only once.
In this retrospective study, eight women and one man were included. The mean age was 67.2 (range 30–87) years. Four of them had secondary lymphedema after uterine cancer treatment, and the other five patients had primary lymphedema. The mean duration of lymphedema was 18.4 (range 2–34) years. The severity of lymphedema as classified on the basis of the International Society of Lymphedema stages was stage 1 in one limb, stage 2a in four limbs, stage 2b in seven limbs, and stage 3 in four limbs. The remaining limbs were not affected by lymphedema. The average duration of hospital stay was 17.0 (range 7–29) days.
As compression treatments, multilayer bandaging, Velcro elastic bandaging, and elastic stockings were selected depending on the patient's condition and ability to understand (Fig. 1). Moreover, certified lymphedema therapists performed MLD four to five times per week. Especially at the beginning of the treatment, when the patient's affected limb was edematous and stiff, MLD was performed for about 30 minutes, and as the treatment progressed and the affected limb became softer, MLD time was shortened. Instead, this phase focused on teaching compression therapy. The physiotherapists also instructed the patients in exercise therapy 20–40 minutes a day. To maintain good control of lymphedema after discharge, training was given in self-care that patients can continue at home, so that they did not remain dependent on treatment by medical staff alone.
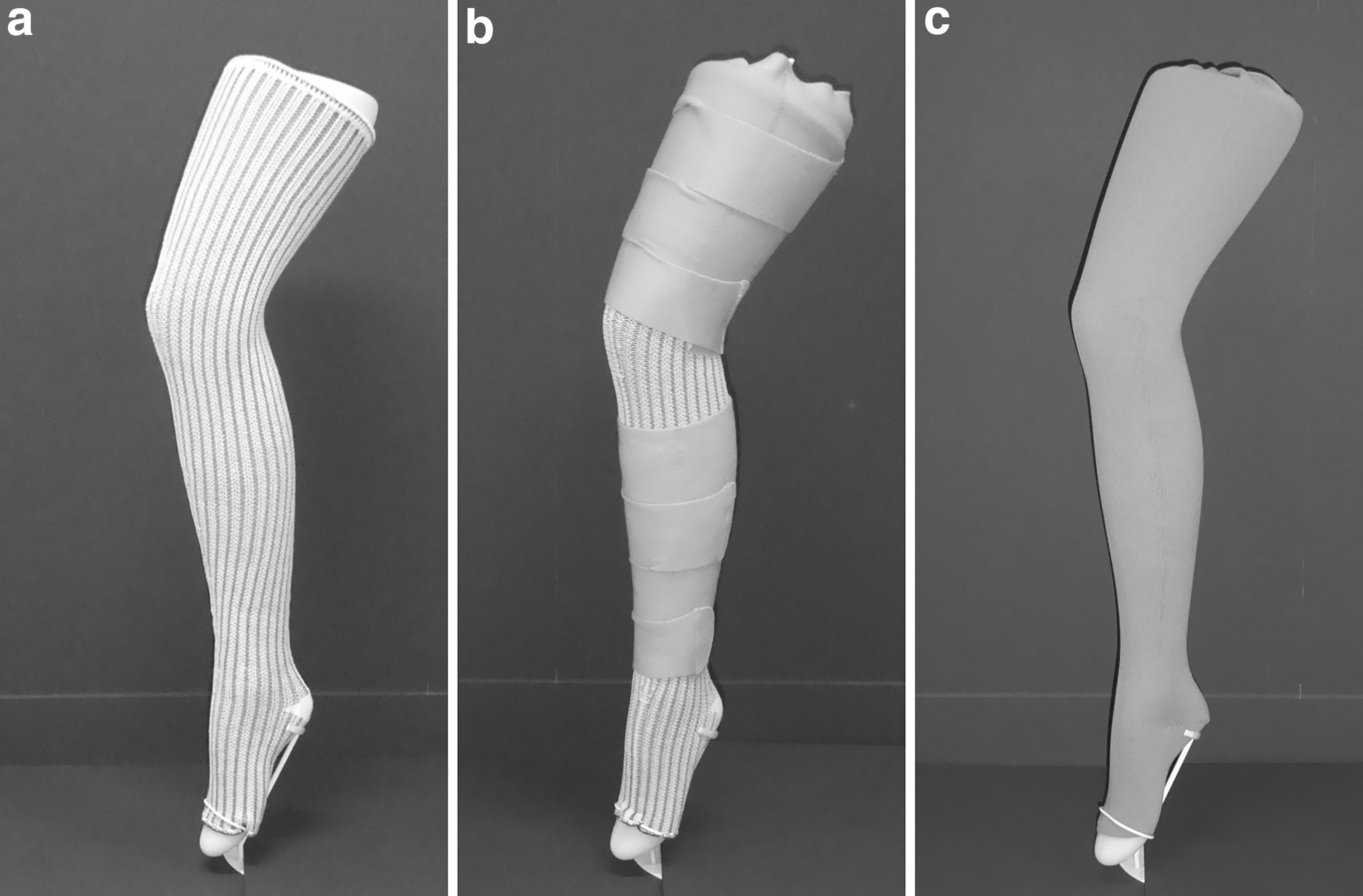
Examples of the items that are used for the compression therapy.
POMS 2nd edition, a Japanese version of the POMS, was used as a method of evaluation of psychological state. 13 POMS is a questionnaire with 65 questions about mood and is based on a 5-point scale ranging from “not at all” to “extremely.” It usually takes 10 minutes to complete the questionnaire and seven scales are evaluated (Table 1). The first POMS test was performed on the day of admission or the following day. The second time was performed 6.8 days (range 5–13 days) on average after admission. The results of the psychological test were evaluated by a certified public psychologist (CPP), and a 60-minute interview was conducted on the patients. Student's t-test was performed by comparing the values of first and second POMS. The significance level was set at p < 0.05. This study was approved by the institutional ethics committee and written informed consent was obtained from each patient (approval number: 30-8).
Seven Scales in Profile of Mood States
Results
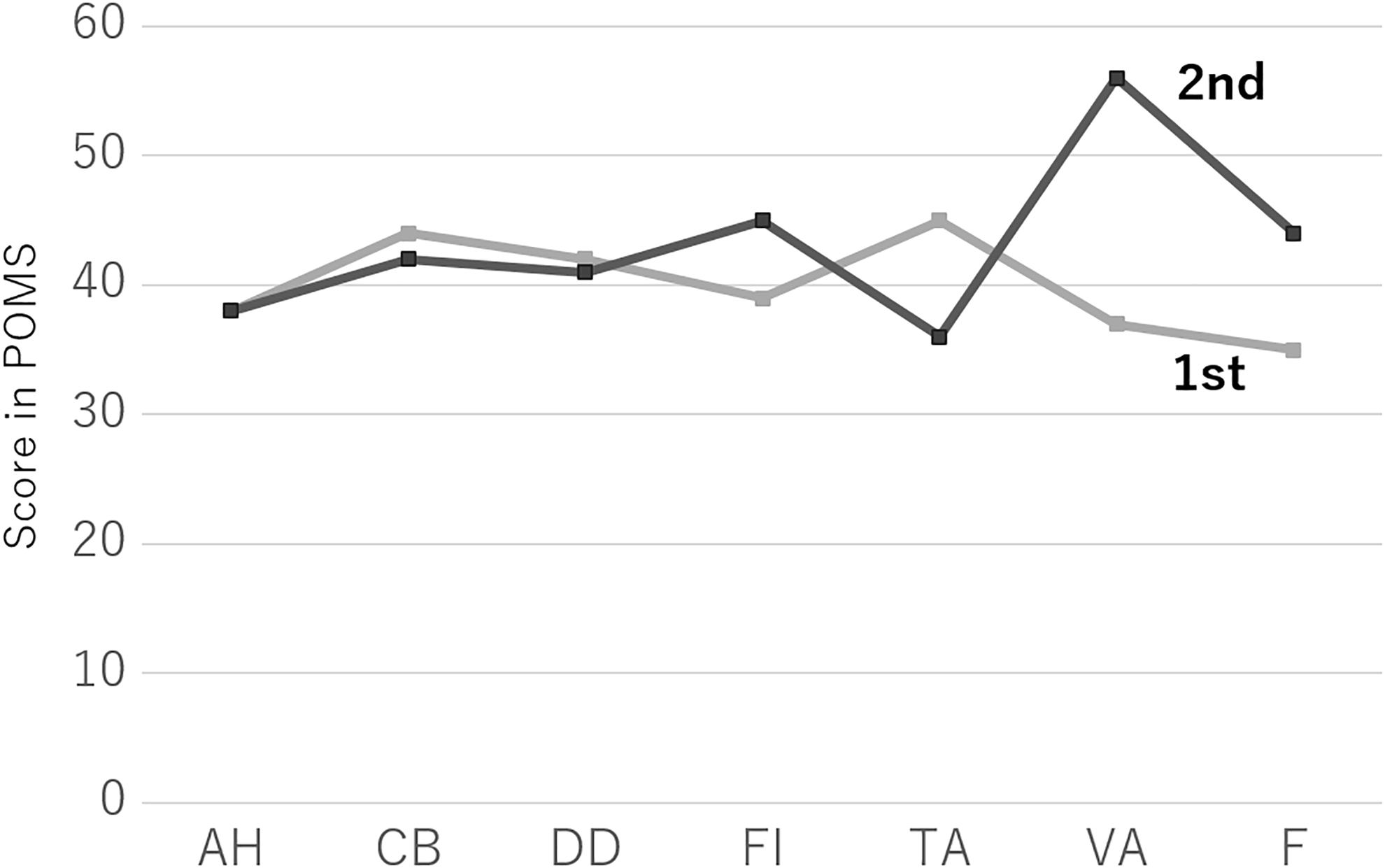
Figure 2 shows the average values of the two POMS tests. The scores of Anger or Hostility (AH), Confusion or Bewilderment (CB), Depression or Dejection (DD), Fatigue or Inertia (FI), and Tension or Anxiety (TA), which show negative mood, were all lower in second POMS than first. In particular, the TA decreased significantly (p = 0.019). Vigor or Activity (VA) showing a positive mood tended to increase from the first to the second time (p = 0.53), although there was no significant difference. Friendliness (F) tended to decrease from the first to the second (p = 0.20). A CPP evaluated that the environmental changes after hospitalization and burdens such as compression therapy and exercise therapy might be expressed as high scores of AH, CB, DD, FI, or TA, and as the treatment progressed, it was considered that the joy of improving edema was manifested as a drop in the scores.

The average values of the two POMS tests. Seven scales including AH: Anger or Hostility, CB: Confusion or Bewilderment, DD: Depression or Dejection, FI: Fatigue or Inertia, TA: Tension or Anxiety, VA: Vigor or Activity, and F: Friendliness were evaluated. The score of AH, CB, DD, FI, and TA, which show negative mood, were all lower in second POMS compared with the first POMS. Especially, TA decreased significantly (p = 0.019). VA showing a positive mood tended to increase from the first to the second, and F tended to decrease. POMS, Profile of Mood States.
In the interview with a CPP, patients' background including childhood, daily life, things they feel joyful or feel painful about, things they want to do in the future, and so on were evaluated. From the contents of the answers to the questionnaire and the interview, some characteristics, such as “cannot ponder,” “cannot do multiple things at the same time,” “not good at verbalizing emotions,” and “cannot think about the causal relationship between emotions and causes,” were identified, and we were able to use them for subsequent self-care guidance. For introverted patients, we were able to understand their feelings through the questionnaires and the interviews with psychologists.
Case Report
An 82-year-old-woman underwent surgical treatment for varicose veins in her legs. After the treatment, edema occurred in the left leg, and the patient was referred to our department. We performed lymphoscintigraphy, and dermal backflow was observed in the left leg. She was diagnosed with lymphedema. As she was old and had difficulty coming to the hospital frequently, we decided to treat conservatively with the patient hospitalized. Because she had a weak grip, she performed compression therapy by layering medical elastic stockings and general low-pressure stockings. She also underwent exercise treatment. After compression therapy and exercise started, the edema in the left leg improved (Fig. 3).

Clinical picture of a patient before admission and 1 week after admission. Lymphedema improved after compression therapy, and exercise was started.
Comparing the first POMS with the second POMS filled out 5 days later, it was found that the FI was higher and that the patient was tired of hospitalization and new treatment (Fig. 4). However, as TA decreased and VA increased, it was clear that she realized the therapeutic effect and felt positive.
The scores of the two POMS tests. Seven scales including AH: Anger or Hostility, CB: Confusion or Bewilderment, DD: Depression or Dejection, FI: Fatigue or Inertia, TA: Tension or Anxiety, VA: Vigor or Activity, and F: Friendliness were evaluated. Comparing the first POMS with the second POMS filled out 5 days later, it was found that the FI was higher and that the patient was tired of hospitalization and new treatments. However, as TA was decreasing and VA was increasing, it was clear that she realized the therapeutic effect and felt positive.
Discussion
In this study, POMS was used to assess patient mood during conservative inpatient treatment for lymphedema. The results showed that patients' negative mood became better, and the positive mood also became better as the treatment progressed. So far, it has been reported that individuals with lymphedema who are postmastectomy patients are more likely to have negative emotions. 14 There are also reports that surgical treatment for lymphedema improves QOL and mental health.11–12 However, few studies have evaluated the psychological changes in patients during conservative therapy.
In this study, the second POMS was administered at an average of 6.8 days after admission. Generally, in the early stage of lymphedema treatment, the volume of the affected limb was significantly reduced by the start of treatment, so the patients' joy was great and it was easy to maintain motivation. However, after 5–7 days, the speed of volume reduction slowed down, and the patients felt tired of living in an unusual environment such as the hospital, which may have caused their motivation to decline. In fact, around this time, we had the impression that negative comments from patients such as “I don't want to exercise,” “I have a pain in my knee,” and “I can't learn self-care” were increasing. However, the POMS results in this study showed that the negative mood improved in the second POMS and tended to be more vibrant than immediately after admission. In particular, TA scores were significantly reduced.
Immediately after admission, there was anxiety, tension, and confusion about the start of new treatment in a new environment, which may not have been expressed verbally to the medical staff. There was a possibility that, after a week, when the relationship with the medical staff was established, it became possible to express negative emotions in words, and the impression from the medical staff was that it seemed to be a negative feeling at this time. With that in mind, the patient's negative remarks may be regarded as proof of “relaxation of tension” and “safety.”
From immediately after admission to the second time point, the F scores tended to decrease. Especially for sociable patients, it was thought that the decrease in opportunities to talk with others during hospitalization had a negative effect. It is probable that this effect was caused because interaction with other patients is not recommended currently due to the coronavirus pandemic, and there are also restrictions on visits by the family or friends.
POMS was developed by McNair, Droppleman, and Lorr in 1971 with the aim of approaching human emotions from subjective aspects such as mood, emotions, and emotions. 15 A simple questionnaire can objectively evaluate a patient's psychological state. Currently, it is used in a wide range of fields such as cancer treatment, sports, and smoking cessation.16–18 In Japan, in the early 1990s, Yokoyama et al. translated it into Japanese and verified its reliability and validity. 13
In the area of lymphedema treatment, scientific evidence has recently been created by visualizing the pressure of compression therapy and echo imaging of the subcutaneous tissue during the course of treatment.19–22 By quantifying the psychological aspect of the patient, it will also be possible to adjust the load of self-care practice accordingly. In addition, when assessing POMS, the CPP interviewed patients to evaluate patients' backgrounds and concerns that did not appear in the questionnaire, especially in patients with severe lymphedema. Support from a professional psychologist was considered to be desirable, including helping patients understand and accept themselves, or cognitive-behavioral therapy.
The limitation of this study is the small number of cases. In addition, the value of negative emotions tended to decrease and vitality increased during hospitalization, but it is unclear from this study what kind of changes will occur after returning to daily life after discharge. Moreover, in this study, we evaluated POMS at admission and after 5 days of admission. We believe that further research is needed to assess mood after the end of treatment with a larger number of the patients and a longer follow-up.
Conclusion
It was found that inpatient conservative therapy for lymphedema tends to have a positive effect on the psychological aspects of patients. Although there are stresses due to changes in the environment after hospitalization and burdens such as compression therapy and exercise therapy, it was considered that the joy of improving edema was greater. By practicing self-care while objectively evaluating the patient's psychological state, it was thought that the load amount and speed suitable for the patient could be adjusted, and more appropriate and effective guidance could be provided.
Footnotes
Authors' Contributions
Conception, data collection, critical revision, approval of the article, accountability, and statistical analysis by H.H., H.M., and M.M. Analysis by H.H. and H.M. Writing article by H.H.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.