
Abstract
Introduction:
The reported incidences of breast cancer-related lymphedema (LE) affecting the arms vary greatly. Reason for this variability includes different diagnostic techniques used across studies. In the current study, we compared the accuracy of indocyanine green lymphography (ICG_L) and bioimpedance spectroscopy (BIS) in detecting LE before presentation of clinical signs.
Methods and Results:
Patients with no initial detectable signs of clinical LE of their arms after axillary lymph node dissection or removal of >5 lymph nodes on sentinel lymph node biopsy were included. Subclinical LE was defined as BIS values outside the normal range [(≥7 units (or >10 units)] or a 7-unit (or 10 unit) change between two measurements. We tracked ICG_L and BIS measurements for 133 potentially affected arms (n = 123). ICG_L detected signs of lymphatic flow disruption in 63 arms (47%). Based on the BIS value of 7 units, 60 arms (45%) had values outside the normal range. When using ICG_L-identified LE cases as true positives, BIS had a 54% accuracy (area under the curve [AUC] = 0.54) in detecting LE. Accuracy was 61% for subclinical LE symptoms when compared with ICG_L (AUC = 0.62). Both BIS and subclinical LE symptoms had <0.70 AUC-receiver characteristic operator curve, suggesting that BIS and development of subclinical LE symptoms are not adequate for identifying patients with subclinical LE.
Conclusion:
ICG_L is a reliable diagnostic tool for detecting early signs of lymphatic flow disruption in subclinical LE. Utilizing ICG_L to diagnose subclinical LE followed by a personalized treatment plan may provide patients the best chance of preventing disease progression.
Introduction
Breast cancer mortality has been decreasing over the years as developments and improved outcomes in diagnosis and treatment continue to emerge. 1 Therefore, more patients are living with treatment consequences after the disease. Breast cancer-related lymphedema (BCRL) is among the most common complications of treatment and is associated with discomfort, fullness, heaviness, tightness, and decreased range of motion of the upper extremity, causing functional impairment, chronic disability, decreased quality-of-life, and psychological distress.2,3 Treatment-related, disease-related, and patient-related factors have been shown to increase the risk of impairing the drainage function of the lymphatic system.4–12 Unfortunately, despite recent advances for surgical interventions to prevent and treat lymphedema (LE), such as lymphovenous bypass or lymph node transfers, there is a lack of evidence and consensus on efficacy of these procedures on BCRL to allow patients to return to their presurgical status.13–15
The incidence of BCRL is highly variable, with a range of 0%–94% among different studies 16 and an estimated average of 21.4%, 17 and increases over time.18,19 Although the extent and modality of breast cancer therapies and duration of follow-up have had a major impact on the incidence of LE, high variability among studies is also a result of different diagnostic techniques and lack of a standardized definition of clinical LE. Accurate and early diagnosis of LE, even before the onset of clinical symptoms, is crucial to allow surveillance and development of personalized and timely interventions to prevent progression to symptomatic LE.20–22 However, diagnosis can be particularly challenging in patients without signs or only minimal clinically detectable signs of lymphatic flow disruption and increases in the extracellular fluid.
Early diagnosis and measurement of LE severity can be based on objective measurements of volume or extracellular fluid or subjective assessments of physiological lymphatic vessel function. 23 Standard techniques used to measure limb volume include circumferential tape, water displacement, and perometry.8,16,24 Bioimpedance spectroscopy (BIS) is a measurement of the extracellular fluid in an extremity and its use has been described in diagnosing LE at an early stage.25–27 This technique is incorporated into routine breast cancer clinical practice to detect subclinical LE and has the advantage of being objective and noninvasive.21,28,29 Recently published stratified, randomized, international trial also demonstrated the value of BIS over tape measurements on identifying patients likely to benefit from an early compression intervention. 30 However, frequent measurements every 3 to 6 months are recommended, especially in the first 5 years following surgery, to diagnose subclinical LE using BIS.31,32
In contrast, lymphoscintigraphy had been considered the gold-standard for evaluating physiological lymphatic function, as it allows visualization of flow through deep and superficial lymphatics and lymph nodes using radioactive tracing.33–35 Indocyanine green lymphography (ICG_L) is a more recently developed method that uses indocyanine dye to assess lymphatic function and is used for detailed visualization of the physiological lymphatic flow. ICG_L is a minimally invasive procedure that has often been performed in an office setting and yet is flexible enough to be performed at any time.36–38 Contraindications include patients with iodine allergy and patients in dialysis. Abnormal or reflux patterns seen on ICG_L have been shown to correlate well with abnormal changes in other limb volume measurements for diagnosing LE.39–41
When compared with lymphoscintigraphy, ICG_L has increased diagnostic value, is less invasive, costs less, and poses no radiation exposure risk to the patient.42,43 In addition, a water-based ICG solution can travel faster within the lymphatic channels compared with the technetium 99 used in lymphoscintigraphy, allowing real-time, high-resolution imaging. 44
Improved detection of subclinical LE may allow early intervention when LE is most easily treated and will lead to a decrease in the development of clinical LE. In this study, we aimed to compare the sensitivity and specificity of ICG_L and BIS in prospectively monitored patients who underwent axillary lymph node dissection (ALND) or had more than five sentinel lymph nodes (SLNs) removed. We hypothesize that ICG_L is more sensitive and specific for the diagnosis of subclinical LE compared with BIS and subclinical LE symptoms.
Patients and Methods
Between October 2018 and December 2021, patients who had ALND or had more than five SLNs removed were enrolled in the Magee-Womens Hospital Breast Cancer Center Lymphedema Education, Monitoring, Early Detection, and Prevention Program prospective database. This study was approved by the University of Pittsburgh Institutional Review Board. Age, surgery type, number of removed lymph nodes, LE stage, ICG_L stage, outcomes, and follow-up time were recorded.
Based on our clinical protocol, patients received postoperative education for prevention of LE. All patients' arms were measured bilaterally using circumferential tape immediately after surgery and monitored every 3 to 6 months for the first year after the surgery; afterward, measurements were made annually for 5 years. Girth was measured circumferentially using a tape measure at predetermined sites on the involved and the uninvolved limbs. Measurements were taken starting at the tip of the fourth finger and proceeding proximally in 5 cm intervals along the limb for six consecutive points. 21 The L-Dex® U400 or SOZO (Impedi Med limited and ImpediMed, Inc.) was used for BIS measurements.
BIS measurements were performed at the same timepoints as the tape measurements as immediately after surgery and monitored every 3 to 6 months for the first year after the surgery. Subclinical LE was defined as either L-Dex® values outside the normal range (between −7 and +7 units) or values that changed ±7 L-Dex® units from baseline, with no detectable signs of clinical LE. Subclinical LE symptoms were defined as patient-reported symptoms such as discomfort, heaviness, or fullness without detectable swelling. We also considered 10 L-Dex® units or 10-unit changes as abnormal L-Dex® measurements. Clinical LE was defined as having (1) a girth difference of ≥2.0 cm in the involved limb versus the uninvolved limb, (2) visible swelling, or (3) texture changes in visual examination.
In our protocol, ICG_L was used to screen for and diagnose LE, and all patients in the study had ICG_L measurements (Fig. 1). ICG_L was performed once at any time postoperatively. In patients receiving radiotherapy, ICG_L was performed after the radiotherapy was completed. The near infrared camera system (PDE; Hamamatsu Photonics K.K.) was used for this study. ICG injection, USP (25 mg; Patheon Italia S.p.A) was diluted with 10 mL of saline. To evaluate lymphatic flow in the arm, three injection sites were used in the distal aspect of the upper limb on the affected side: the first, second, and fourth web spaces, and when necessary, additional wrist or elbow regions. MD Anderson Cancer Center LE classification was used for staging based on ICG_L findings. 45
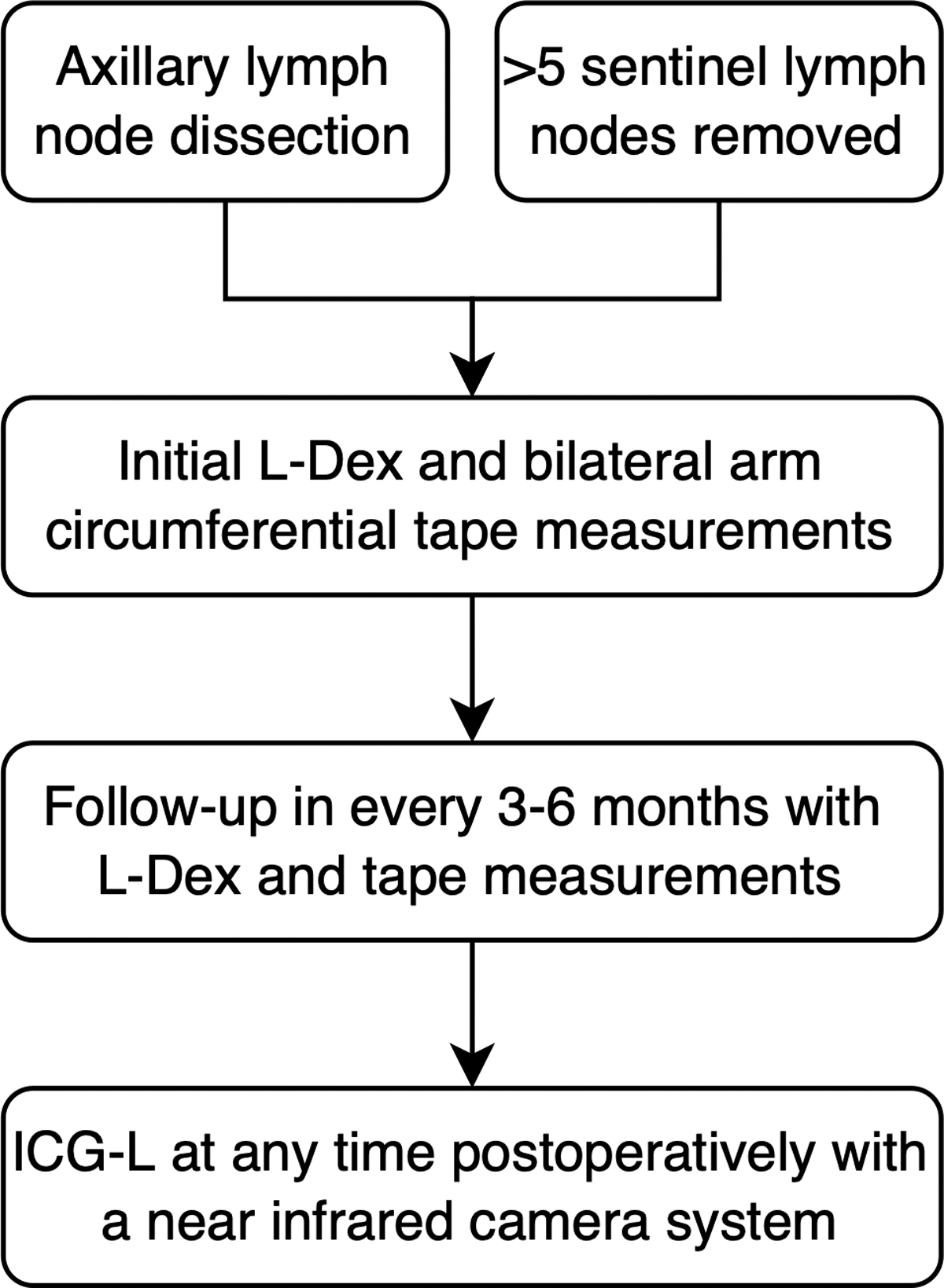
Flowchart of the patients included in the study.
Stage 1 was defined as many patent lymphatic vessels, with minimal, patchy dermal backflow; stage 2 as a moderate number of patent lymphatic vessels, with segmental dermal backflow; stage 3 as few patent lymphatic vessels, with extensive dermal backflow involving the entire arm; and stage 4 as no patent lymphatic vessels seen, with severe dermal backflow involving the entire arm and extending to the dorsum of the hand. 45 In addition, ICG was injected into the axillary, breast, and chest wall regions to detect any abnormal lymphatic flow or dermal backflow pattern in these regions. Patients diagnosed with subclinical LE based on ICG_L results were prescribed a personalized compression treatment plan and were followed for progression every 6 months.
For the analysis, ICG_L was considered the gold standard diagnostic method to demonstrate anatomical lymphatic flow disruption in the patients. Results from ICG_L were compared individually with BIS measurements and with having subclinical LE symptoms to determine sensitivity and specificity of the diagnostic methods. In addition, positive predictive value (PPV), negative predictive value (NPV), Pearson's R values, and area under the curve (AUC) of receiver characteristic operator curve (ROC) were used to compare diagnostic methods. AUC values of the ROC ranged from 0.5 for no diagnostic ability to 1.0 for the highest diagnostic ability. Thus, an AUC of 0.7 would mean that the test would correctly diagnose 70% of the time. In this study, an AUC value of 0.7 was considered the diagnostic cutoff.
Statistical analysis was conducted using IBM SPSS Statistics Version 27. Categorical values were analyzed using chi-square test, and numerical variables were analyzed using Student's t-test and reported as means with standard deviations. p < 0.05 was considered statistically significant.
Results
We enrolled 123 patients, which accounted for 133 arm ICG_L and BIS measurements in our prospectively maintained database (Table 1). The mean patient age was 54.89 ± 12.04 years old. Breast surgery type included segmental mastectomy in 46 patients (35%), total mastectomy in 86 patients (65%), and other surgery in one patient (1%). SLNB was performed in 57 patients (43%), ALND was performed in 74 patients (56%), and 2 patients had a history of other axillary surgery. The median (with interquartile range [IQR]) follow-up period was 6.28 [9.12] months.
Demographics and Surgical Details of the Patients
ALND, axillary lymph node dissection; IQR, interquartile range; SLNB, sentinel lymph node biopsy.
ICG_L detected signs of lymphatic flow disruption in 61 patients (49.5%) and 63 arms (47%). Forty-six patients out of 123 had subclinical LE symptoms. In 48 patients (37%), there was a discordance between subclinical LE symptoms and ICG_L, where 15 patients (25%) had no subclinical LE symptoms but were positive with ICG_L, and 33 (42%) had subclinical LE symptoms but had no detectable lymphatic flow discretion based on ICG_L images. The specificity and sensitivity of having subclinical LE symptoms as a reference to the ICG_L were 47% and 75%, respectively, with an AUC of 0.62 and an R value of 0.23 (Table 2).
The Diagnostic Value of Lymphedema Symptoms and Bioimpedance Spectroscopy Measurements Versus Indocyanine Green Lymphography
AUC, area under the curve; BIS, bioimpedance spectroscopy; ICG_L, indocyanine green lymphography; LE, lymphedema; NPV, negative predictive value; PPV, positive predictive value.
Considering the value of 7 L-Dex® units as the cutoff, 60 patients (49%) had positive BIS results. Among these 60 patients with results >7 L-Dex® units, 31 patients (52%) had LE based on ICG_L images. PPV was 52%, NPV was 56%, and accuracy was 54% (Table 2). Among these 31 patients, 12 patients (39%) also had lymphatic flow disruption at the axillary, breast, or chest wall regions detected by ICG. In the remaining 29 patients (48%), ICG_L did not detect any signs of lymphatic flow disruption despite a positive BIS result. Among these 29 patients with a high L-Dex® number, 11 (38%) had lymphatic flow disruption at the axillary, breast, or chest wall regions detected by ICG_ L.
On BIS measurements, when the criterion included patients with L-Dex® values outside the normal range (
Twenty-seven patients (21%) had a follow-up period of >12 months (median [IQR] follow-up 17.00 [7.18] months). Among these, 18 (67%) had initial signs of lymphatic flow disruption on ICG_L. On their most recent follow-up, only 8 of these 18 patients (44%) had clinical LE symptoms and 10 (56%) did not have clinical LE symptoms.
Discussion
Early detection with surveillance and timely interventions are crucial in BCRL to prevent the development of an established LE with clinically apparent symptoms.20–22 BIS is currently utilized in routine clinical practice to detect subclinical LE.21,28,29 However, the accuracy of BIS has not been determined and current guidelines recommend that BIS results be considered along with other volumetric assessment methods. 46 ICG_L, on the contrary, is among the most sensitive measurements for LE, as it displays the function of the lymphatic vessels.39–41 To our knowledge, this is the first study to compare the accuracies of ICG_L and BIS in detecting subclinical LE. We determined that ICG_L is more accurate than BIS measurements in diagnosing subclinical LE.
In our study, both BIS measurements and subclinical LE symptoms had a <0.70 AUC-ROC when compared with ICG_L. Patients may be receiving lifetime treatment unnecessarily, considering that BIS-positive results are labeling around 50% of cases incorrectly. In contrast, around 50% of patients with negative BIS results had BCRL diagnosed with ICG_L and received LE treatment. The high false-negative rate of BIS is consistent with that reported in the literature. Qin et al. identified a 36% false-negative rate with BIS when compared with ICG_L and concluded that BIS is not sensitive enough to rule out LE if there is a negative result in LE patients. 47 Despite their study including patients with both upper and lower extremity LE, it was the first to compare the diagnostic accuracy of BIS using ICG_L as the reference standard.
Similarly, Qin et al. also assessed single and multisegment BIS measurements relative to ICG_L with a focus on bilateral LE. 48 Finding similarly high false-negative rates with both modalities versus ICG_L, the authors concluded that early changes in lymphatic flow disruption may not be reflected in BIS measurements without signs of detectable edema. Both studies included patients with multiple LE stages and did not solely focus on subclinical LE. Multiple studies comparing BIS with other diagnostic modalities also demonstrated the unreliability of BIS in detecting changes in the lymphatic system and subclinical LE.49,50 As shown with our results, minimally invasive ICG_L is proving to be a superior diagnostic tool for reliably diagnosing subclinical LE.
For BIS measurements, different L-Dex® unit change cutoff values have been described for the diagnosis of LE.21,27,31 A recent study concluded that 7 or more units should be used to indicate clinical LE and suggested that subclinical LE occurs at near 6.5 or more units. 31 In our study, we utilized both the 7 and 10 unit change cutoffs reported in the literature. Despite having a higher specificity with 10 units, this cutoff value also had a lower sensitivity at 29%. When the cutoff value of 7 was used, the sensitivity was higher at 49%, while both had similar low AUC values. In addition to demonstrating the low diagnostic value of BIS compared to ICG_L for subclinical LE, our study also highlights the need for well-defined criteria, specifically for this patient cohort.
In a recent large scale, long-term, randomized clinical trial, BIS with L-Dex® units of 6.5 or more was found to be more reliable than tape measurements for early interventions. 30 Upon diagnosis, compression treatments were initiated for patients and they were followed accordingly for disease progress. However, the patients included in the trial were not evaluated for underlying anatomical lymphatic flow disruption. It is possible that compression treatment was not initiated for patients with lymphatic flow disruption and no detectable signs of extracellular fluid change in the extremities. Although the major limitation of ICG_L is the need for a minimally invasive procedure performed in the operating room, the diagnostic value and importance of initiating early treatment could outweigh its limitations.
In addition, ICG_L is superior in detecting signs of lymphatic flow disruption in anatomical regions other than the wrist and arm, such as the axilla, breast, or chest wall. In our series, among 29 patients with a positive BIS (when a 7 unit cutoff value was used) and a negative ICG_L of the arm, 11 (38%) had a positive result with ICG_L of the axilla, breast, or chest wall. Therefore, when there is a lymphatic flow disruption, BIS can be misdiagnosing patients with arm LE, regardless of the anatomical location of the flow disruption, reducing the effectiveness of the diagnosis and potential patient-specific preventive measures.
In our study, we also compared the diagnostic value of the presence of subclinical LE symptoms to ICG_L measurements. We identified a 58% correlation between a patient with subclinical LE symptoms and a positive ICG_L result for LE. Wiser et al. identified ICG_L as the most sensitive test for LE, when compared with different diagnostic approaches. 40 In their study, all abnormal limbs with a volume of >10% also had abnormal ICG patterns; however, they could not determine the specificity of the test due to the lack of patients who did not develop clinical evidence of LE. We detected a similarly high sensitivity rate (75%) and a low specificity rate (47%) for ICG_L when compared with subclinical LE symptoms. ICG_L was able to accurately detect early signs of lymphatic flow disruption in patients following axillary surgery, even before clinically detectable signs were present.
These results show that BIS and subclinical LE symptoms are not the best tools to use in distinguishing between positive and negative patients for LE, when patients do not present with clinically detectable swelling. In patients at high risk for BCRL, however, the absence of subclinical LE symptoms is more accurate than a negative BIS. This finding is also similar to that from a recent study by Keeley, where limb volume measurements performed better than BIS for early detection of BCRL, suggesting the value of monitoring in early detection and prediction of subclinical LE. 51
Personalized approaches in the treatment of BCRL are expanding with potential benefits to prevent disease progression with early intervention. Therefore, the ability to detect even the earliest signs of flow disruption and having a specific plan for the patient's needs is critical. In addition to detecting disruption in flow, ICG_L allows visualization of the compensatory drainage regions, potentially enabling patients to benefit the most from directed compression treatments and manual lymphatic drainage. Although there is consensus that ICG_L should be widely used in the visualization of lymphatic structures, 37 it should be also highlighted that its application is still minimally invasive and may be limited depending on institutional resources. As described by Koelmeyer et al., personalized conservative management plans have shown benefit in patients with LE. 52 Utilizing a similar approach for subclinical LE patients, we prescribed personalized compression treatment plans in patients with detectable signs of flow disruption in ICG_L.
One limitation of our current study is the short follow-up duration. However, despite being diagnosed as having subclinical LE by ICG_L, 56% of the patients with follow-up data longer than 12 months did not advance to LE symptoms. With additional ongoing follow-up and advanced protocols to optimize the treatment approach, our study continues to prove the value of ICG_L in detecting patients earlier and providing the option to prescribe a personalized approach to LE treatment.
Conclusion
Minimally invasive ICG_L seems to be the best available reliable tool for diagnosis of LE. Adapting earlier stage ICG_L to the subclinical LE diagnosis protocol provides accurate diagnosis and the critical opportunity to start early treatment accordingly.
Footnotes
Acknowledgment
The authors thank Christine Burr, Scientific Writer from the University of Pittsburgh, for her assistance with language editing.
Authors' Contributions
A.S.: Writing – original draft (equal); writing – review and editing (equal); conceptualization (lead); formal analysis (equal); software (equal); and methodology (equal). F.B.B.: Writing – original draft (equal); writing – review and editing (equal); conceptualization (equal); formal analysis (equal); software (equal); and methodology (supporting). W.R.: Writing – review and editing (equal); conceptualization (supporting). M.Z.C.: Writing – review and editing (equal) and conceptualization (supporting). E.S.: Writing – review and editing (equal); formal analysis (equal); software (equal); and methodology (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.