
Abstract
Background:
Lymphaticovenular anastomosis (LVA) has recently become a mainstream surgical treatment for lymphedema and is a useful treatment option in addition to conservative therapies such as compression therapy, exercise therapy, and lymphatic drainage. We performed LVA with the goal of stopping compression therapy and report the effect of LVA on secondary lymphedema of the upper extremities.
Methods and Results:
The participants were 20 patients with secondary lymphedema of the upper extremities categorized as stage 2 or 3 according to the International Society of Lymphology classification. We measured and compared the upper limb circumference at six locations before and 6 months after LVA. Significant decreases in circumference after surgery were observed at 8 cm proximal to the elbow, the elbow joint, 5 cm distal to the elbow, and the wrist joints, but not at 2 cm distal to the axilla or the dorsum of the hand. At more than 6 months postoperatively, eight patients who had been wearing compression gloves were no longer required to wear them, and three patients who had been wearing both sleeves and gloves were no longer required to wear them.
Conclusions:
LVA is effective in the treatment of secondary lymphedema of the upper extremities, particularly in improving elbow circumference, and is one of the treatments that contributes significantly to the improvement of quality of life. For severe cases with limited range of motion of the elbow joint, LVA should be performed first. Based on these results, we present an algorithm for upper extremity lymphedema treatment.
Introduction
Lymphedema of the extremities is most often secondary. In some cases, it may be primary where the cause is unknown, such as in congenital lymphedema. 1 Its main causes are lymph node dissection and radiation therapy associated with procedures for breast, uterine, and ovarian cancers in women and prostate cancer in men. The most common cause of upper extremity lymphedema is breast cancer surgery, and one-fifth of breast cancer survivors suffer from lymphedema. 2 In addition, the long-term symptoms are diverse and include pain, skin hardening, infection, fibrosis, deformity, functional impairment, sensory disturbance, increased upper limb weight, distress, and depression, among others.3–5 Since lymphedema is a chronic progressive disease, symptomatic treatment is the mainstay of therapy. Poorly controlled edema reduces patient quality of life. 6
Conservative therapy is the first-line treatment for lymphedema. However, if conservative therapy fails and cellulitis develops, lymphaticovenular anastomosis (LVA) is an effective treatment option.7–9 LVA is a safe treatment because it is minimally invasive and poses no serious complications.10,11 In secondary lymphedema, LVA effectively reduces the volume of edema and improves symptoms. 12 Furthermore, the use of LVA for lymphedema prophylaxis has recently been reported.
The effect of lymphedema treatment is often evaluated according to the change in limb circumference before and after treatment, and many reports use the change in circumference or volume of the entire upper or lower extremity as an indicator of treatment success. However, few reports have evaluated treatment success by changes in limb circumference at multiple sites. In this study, we assessed the effect of LVA on secondary lymphedema of the upper extremities at multiple anatomical sites and evaluated the effect of discontinuation of compression therapy.
Materials and Methods
All participants in the study provided written informed consent for the publication of this study and agreed to the scientific use of their data. The study was conducted retrospectively in accordance with the Declaration of Helsinki and was approved by the institutional ethics board of Toyama Nishi General Hospital (approval no. 22-02; ClinicalTrials.gov). The participants were 22 patients with secondary upper limb lymphedema who underwent LVA from 2017 to 2022 at Toyama Nishi General Hospital. Those with a medical cause for edema such as heart failure were excluded from the study. Of the 22 cases included, the causes of lymphedema were axillary lymph node dissection for breast cancer in 21 cases and resection of a supraclavicular lymph node with metastasis from gastric cancer in one case.
Two of these cases were excluded: one patient with multiple systemic metastases of breast cancer and one patient with cardiac disease. Patients were diagnosed with lymphedema by preoperative indocyanine green (ICG) lymphangiography and were categorized as stage 2 or 3 according to the International Society of Lymphology (ISL) classification. 13 Patients who had received conservative therapy for more than 3 months with no prospect of further improvement or who had deteriorated with conservative therapy alone underwent LVA and were followed up for more than 6 months after surgery.
Measurements
We measured the circumference of the upper extremity in 20 cases. Before and 6 months after surgery the same lymphedema therapist measured the limb circumference at six locations: 2 cm distal to the axilla, 8 cm proximal to the elbow, at the elbow joint, 5 cm distal to the elbow, at the wrist joint, and at the dorsum of the hand.
Surgical procedures and compression therapy
The surgeries were performed under general anesthesia with a brachial plexus block. ICG lymphangiography was performed immediately before surgery to confirm the location of the lymphatic vessels. We injected 0.1 mL of ICG subcutaneously between the first and fourth fingers on the dorsal surface of the hand and drew in real time the flow of ICG through the lymphatic vessels, marking the site where the dermal backflow 14 first appeared on the lymphatic vessels. Furthermore, by echocardiography, we located a vein with a diameter of ∼1 mm just distal to the mark and close to that lymphatic vessel, which we designated as the anastomosis site.
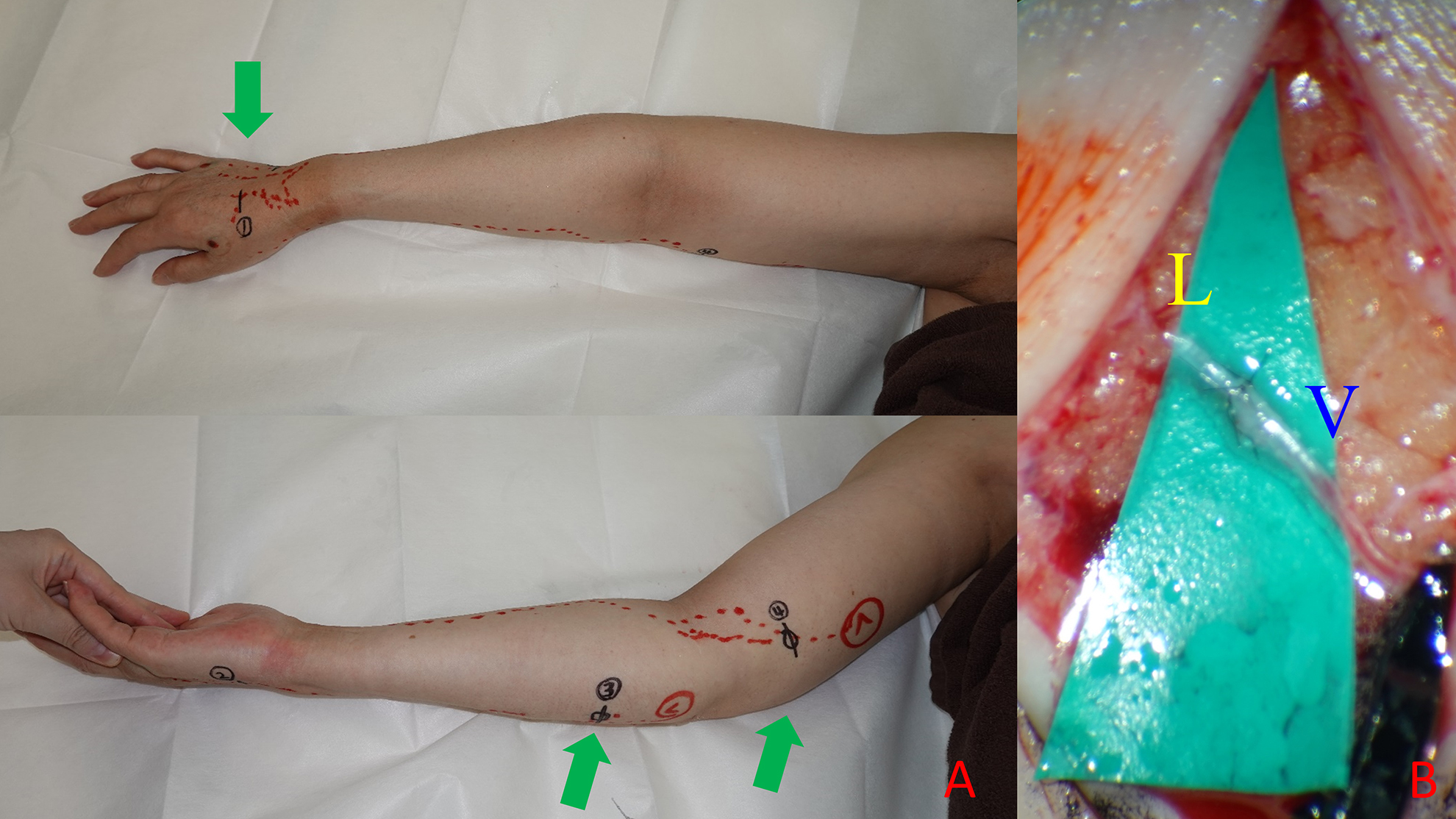
The anastomotic sites included the dorsum of the hand, forearm, and upper arm; these sites varied according to the site of dermal backflow appearance in the upper extremity of each patient (Fig. 1). In stage 3, we injected additional ICG around the wrist and elbow joints where there was less skin hardening to delineate the lymphatic vessels. If the lymphatic vessels still could not be delineated, we sometimes made incisions on the dorsum of the hand or around the wrist and elbow joints and identified the lymphatic vessels under the microscope.
Patients resumed compression therapy with a sleeve (and glove) the day after surgery until 6 months postoperatively. In severe cases, they wore a sleeve and glove during the day and performed a multilayered bandage technique at night on days when they had severe edema. The following three criteria were used to terminate compression therapy: (1) there was no worsening of circumferential diameter even after compression was stopped, (2) the dorsal veins of the hands could be seen on the healthy side as well as the operative side, and (3) the patient did not have subjective symptoms.
During the 6-month postoperative period, gradual compression relief was initiated. First, if the patient was provided compression at night, it was discontinued. If the criteria were met a few months after that, the gloves were then removed during the day. If the criteria were then met again after a few months, the sleeve was also removed. If criteria were not met at any point, the compression regimen was returned to that of the previous phase.
Analyses
Categorical variables are presented as the count and percentage for each category. To compare the effect of weight change on limb circumference, the affected limb's circumference was calculated as a percentage of the unaffected limb's circumference. The limb circumferences (as a combination and at each individual point) before and 6 months after surgery were compared using a paired t-test. In addition, 10 patients with stage 2a in the ISL staging were designated as the early-stage group and 10 patients with stage 2b and stage 3 as the severe-stage group, and the improvement rate of circumferential diameter values was compared between the two groups using a two-sample t-test. All statistical tests were two-sided and evaluated at an α of 0.05.
Results
The mean age of the patients was 55.6 years (range: 42‒77 years), with an average time since the onset of edema of 3.5 years (range: 4 months to 25 years). According to ISL classification, 10 limbs were categorized as stage 2a, 5 limbs as stage 2b, and 4 limbs as stage 3. The average number of anastomoses was 2.9 (range: 1‒6) (Table 1). Two of the four stage-3 patients in whom lymphatic vessels could not be identified by preoperative ICG lymphangiography had one anastomosis. The sum of the limb circumferences at the six anatomical sites improved significantly at 6 months postoperatively. Each individual site showed an improvement in mean values. However, significant differences were observed only at 8 cm proximal to the elbow, the elbow joint, at 5 cm distal to the elbow, and the wrist joint, but not at 2 cm distal to the axilla or the dorsum of the hand (Table 2).
Patient Demographic and Clinical Characteristics
Categorical variables are presented as n (%). Continuous variables are presented as mean ± standard deviation (range).
ISL, International Society of Lymphology.
Comparison of Limb Circumference Before and After Surgery
Statistical significance.
Compression therapy was simplified after LVA (either the sleeve or glove was no longer worn) in 8 out of 20 patients (40%). Five patients did not require gloves before surgery. The criteria for determining that the sleeve or glove did not need to be worn were that the individual was not aware of edema and there was no worsening of circumferential values when not wearing the sleeve or glove. In 8 of 15 cases (53%), patients who had been wearing gloves were no longer required to wear them after surgery (Table 3). Both sleeves and gloves were no longer worn after surgery in 3 of 20 cases (15%).
Percentage of Patients for Whom Compression Therapy Could Be Simplified 6 Months After Lymphaticovenular Anastomosis
We considered these three cases as cured (Fig. 2). The number of anastomoses, the anastomotic site, and the course of compression therapy are listed for each patient in Table 4. A comparison of the pre- and postoperative improvement rates in the mild and severe groups showed improvement in all areas. The overall improvement rate was higher in the severe group than in the mild group, but there was no significant difference in the improvement rates between the two groups. Both groups had the highest improvement rate in circumference at the elbow joint, but there was no significant difference in the improvement rate between the two groups (Table 5).

A case of left upper limb lymphedema. Measurement results before surgery
Surgical and Compression Therapy Details of Patients
Comparison of Limb Circumference Improvement Rates Between Mild and Severe Groups
We developed an algorithm taking into account the location and severity of edema (Fig. 3). Cases complicated by cellulitis are strongly indicated for LVA. Even without cellulitis, edema of the hand is a strong indication for LVA. If edema around the elbow is observed and joint contracture is present or is likely to occur in the future, LVA should be performed first, followed by conservative treatment, such as exercise therapy under compression. If edema is present only in the proximal upper arm or if there is no possibility of joint contracture, surgical treatment should be considered if the disease worsens during follow-up. Liposuction 15 should also be kept in mind for patients with subcutaneous fat deposits corresponding to stage 3 in the ISL classification.

Proposed algorithm for treatment of upper limb lymphedema, taking into account the location and severity of the edema.
Discussion
LVA, developed by Koshima et al. in the 1990s, has recently become a mainstream surgical treatment for lymphedema of the extremities. 16 It has also been shown to have long-term beneficial effects that have not been seen with previous surgical procedures.17–20 Conservative therapy such as compression with elastic bandages and gowns and manual lymphatic drainage are common treatments for lymphedema of the extremities. In addition to these conservative therapies, LVA is a useful treatment option.8,21
According to the results of this study, LVA is particularly effective in cases of severe edema around the elbow, as it improves the circumference of the elbow joint significantly. This suggests that LVA may be effective even in severe cases involving limited range of motion of the elbow joint and that edema can be improved without the use of multilayer bandages during the day. The reduced time spent using the multilayer bandage allows for more efficient exercise therapy. The thickness of the bandage makes it difficult to perform exercise therapy, which may result in joint contractures and muscle weakness. 22
Therefore, severe cases that require multilayer bandaging may be better treated with LVA as early as possible, rather than persisting with conservative therapy. The advantages of preceding LVA in conjunction with exercise therapy may result in further improvements in edema. Furthermore, the results of this study showed that the improvement rate of circumference was not significantly different between the severe and mild groups, but the improvement rate tended to be higher in the severe group, especially at the elbow joint. LVA is considered to be more effective when performed in the early, rather than late, stage of the disease,4,23,24 but the results suggest that LVA is effective not only for mild lymphedema but also for severe lymphedema.
Some articles have shown the effectiveness of LVA for severe lymphedema of the lower extremity,25,26 and LVA is similarly effective for severe lymphedema of the upper extremity. In contrast, when LVA is performed with the goal of stopping compression, it is more likely to achieve this goal in mild than in severe cases; none of the patients with stage-3 lymphedema were able to stop compression. To stop compression, LVA should be performed as early as possible.
The lack of significant improvement in limb circumference 2 cm distal to the axilla is thought to be due to fat deposition in the upper arm. 27 In such cases, LVA alone is not sufficient and must be combined with liposuction or other procedures to reduce adipose tissue.15,28 In contrast, measurements of the dorsum of the hand showed improvement in the postoperative period in most cases but failed to reach statistical significance. This can be attributed to the following two problems. One is that the original circumference value is small, and the other is that the glove is sometimes removed for handwashing or water work, making it difficult to stabilize the measurement value.
Another reason is that the gloves may have been removed more frequently than before surgery, as more than half of the cases no longer required gloves at 6 months postoperatively. Since abnormal sensation and decreased grip strength are the main symptoms affecting the fingers, dorsum of the hand, and palm, multifaceted evaluation indices, such as skin hardness, sensation, joint range of motion, and grip strength, are required in addition to circumference.3,20 The mandatory wearing of gloves decreases the quality of life and causes patients to resist compression therapy. Based on the results of this study, LVA is one of the treatments that contribute significantly to the improvement of quality of life, since 53% of the cases did not require gloves after surgery. Therefore, cases of edema of the dorsum and palms are strong indications of LVA.
In this study, one patient showed no improvement due to external factors. The patient was a user of corrective underwear, which caused pressure at the shoulder joint, resulting in unstable measurements. After being advised against wearing corrective underwear, the circumference of the unaffected and affected limbs became almost equal at 1 year after surgery. In four severe cases categorized as stage 3, edema of the dorsum of the hands and palms was marked, and skin sclerosis was also observed.
Although the number of anastomoses created was small, the surgery was effective, and in two of the cases, a second surgery was performed and further improvement was observed. The remaining patient had a poor course due to breast cancer recurrence. The number of anastomoses does not correlate with surgical outcome, and it is important to select effective lymphatic vessels with high flow. 29 Although the choice of surgical procedure is difficult and standardized indications have not yet been established, it is important to understand the pathophysiology of the patient and present a suitable surgical option.30,31
In our proposed algorithm (Fig. 3), the first step is to check for cellulitis, as this condition is quite detrimental to quality of life, and LVA can reduce cellulitis. The next step is to check for hand edema; edema of the hands may cause a patient to wear gloves and interferes with work and daily activities. The results of this study indicate that LVA can contribute to ceasing the wearing of gloves. The next step in our algorithm is to check for severe edema in the elbow joint that may cause joint contracture. The results of this study indicate that LVA is effective in reducing edema in the elbow joint and that subsequent physical therapy is facilitated by preceding LVA. In the absence of cellulitis, hand edema, or severe edema surrounding the elbow, the patient should be followed up with liposuction as an option where fat deposits are present.
Conclusions
LVA was shown to be effective in the treatment of secondary lymphedema of the upper extremities. Since it is especially effective in improving the circumference of the elbow, it can be performed without interfering with exercise therapy. Therefore, if edema around the elbow and joint contracture are observed or are likely to occur in the future, LVA should be performed first, followed by conservative treatment, such as exercise therapy under compression. Furthermore, LVA is one of the treatments that contributes significantly to the improvement of quality of life as in many cases, gloves are no longer needed. Further multifaceted evaluation methods should be proposed for small circumferential areas, such as the dorsum of the hand, which are difficult to evaluate.
Footnotes
Acknowledgments
We thank Ms. Shizue Nogami and Ms. Yuka Hayashi of the Department of Lymphedema Treatment for their assistance with body measurements.
Authors' Contributions
E.H., S.O., and T.S. contributed to the study design. E.H. and S.O. contributed to the writing and revision of the article. E.H. performed surgery and data analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.