
Abstract
Background:
Breast cancer-related lymphedema (BCRL) is a debilitating chronic illness. Early management and prevention of disease progression rely on lymphedema monitoring and assessment. At present, lymphedema monitoring systems are costly and do not promote remote monitoring. Thus, a low-cost, portable, mobile-based bioimpedance lymphedema monitoring system (Mobilymph) was developed to ensure continuous lymphedema surveillance.
Method and Results:
Forty-five healthy and 100 BCRL participants were recruited in this study. Mobilymph bioimpedance measurement was validated with a Quadscan 4000 on healthy participants' arms. The interarm bioimpedance ratio was determined to evaluate the discriminatory capability of Mobilymph to detect BCRL. Mobilymph's bioimpedance results show no significant difference compared to Quadscan 4000. The interarm bioimpedance ratios were significantly different (p < 0.001), between participants in healthy and Stage 1, Stage 0 and Stage 1, and Stage 1 and Stage 2. Healthy and Stage 0 participants had similar interarm impedance ratios (p = 0.63).
Conclusion:
The bioimpedance results show that Mobilymph bioimpedance measurement is comparable to Quadscan 4000 and can detect BCRL arms. Thus, Mobilymph lymphedema monitoring system offers a feasible solution for early lymphedema diagnosis and treatment monitoring.
Clinical trial registration number: MREC ID No.: 2020316-8181
Introduction
Breast cancer-related lymphedema (BCRL) is a chronic progressive disease resulting from breast cancer treatments or metastatic breast cancer. Eight percent to 56% of breast cancer survivors are at risk of developing secondary lymphedema.1,2 Lymphedema is the accumulation of protein-rich fluid in the interstitial space due to interruption of the lymphatic system. 3 The accumulated fluid causes swelling in the upper extremity of the affected side. Stage 0 or latency stage comprised at-risk breast cancer patients with damaged lymphatic system, but shows no clinical signs of lymphedema. The early onset of swelling is seen in Stage 1, whereby elevation reduces swelling. In Stage 2, elevation does not resolve swelling.
As the disease progresses to Stage 3, lymphostatic elephantiasis, severe fibrosis, hypertrophic skin, and nonpitting edema occur. The circumferential volume difference between arms increases as BCRL progresses. 4 Early detection and management of BCRL at Stage 0 and 1 are essential as it is reversible.5,6 Lymphedema becomes chronic and irreversible as the disease progresses to Stage 2 and Stage 3. 7
Postoperative breast cancer patients must regularly attend lymphedema rehabilitation clinics on a weekly to monthly cycle for 3 years as this is the prevalent timeframe for the onset of lymphedema.8,9 Previous studies have reported the association of BCRL patients with decreased quality of life, physical impairment, increased financial burden, elevated depression, and anxiety rates. 10
Various diagnostic and measuring tools are used to identify and manage lymphedema. These include circumferential measurement, water displacement, medical imaging techniques, and bioelectrical impedance analysis (BIA). Circumference measures of the limbs are the most common physical assessment in clinical settings as it is inexpensive and easily accessible. However, circumference measurement identifies lymphedema at a late stage and requires a trained health care provider. 11 Water displacement is seldom used because it is unhygienic, cumbersome, unsuitable for home usage, and associated with risks of infection. 12 Medical imaging is sensitive and accurate for early lymphedema diagnosis. Nevertheless, it could not be used for regular lymphedema measurements as it involves radiation and is a costly method. 13
Previous findings have established BIA as a reliable and sensitive lymphedema diagnostic and monitoring tool. BIA is a fast, easy-to-use, and noninvasive procedure that can monitor subtle lymphatic fluid changes in at-risk breast cancer patients providing an opportunity for early diagnosis and prevention of lymphedema progression.14–16 BIA assesses lymph fluid change by transmitting a small current at a low frequency through the body region of interest and measures the bioimpedance in the extracellular space. In unilateral BCRL assessment, the bioimpedance values of the affected arm with reference to the nonaffected arm are utilized to detect lymphedema. The interarm ratio of a normal healthy population is used as a threshold for lymphedema detection. A BCRL interarm ratio that exceeds the normative population threshold indicates the presence of lymphedema.14,17
However, the detection of lymphedema in bilateral cases applies a different bioimpedance ratio technique. In bilateral BCRL assessment, the bioimpedance values in extracellular and intracellular spaces of the affected arms are compared to detect lymphedema.18,19 As such, for cases of unilateral BCRL, the interarm ratio can be monitored prospectively and used to determine lymphedema treatment effectiveness.2,20
Self-monitoring of BCRL using BIA has been found to be promising approach for early detection and management of the disease. A study by Ridner et al. evaluated the use of BIA in self-monitoring of BCRL in breast cancer survivors. The study found that self-measurement of bioimpedance was a reliable method for detecting early changes in lymph fluid and that self-care adherence was improved when patients were actively involved in their own care. 21 This suggests that self-monitoring using BIA can be effective tool for early detection and management of BCRL.
The commercially available bioimpedance analyzers for lymphedema measurement are L-Dex U400 (ImpediMed Limited, Australia), 22 Quadscan 4000 (Bodystat, Isle of Man), 23 and SOZO (ImpediMed Limited). 24 Although BIA is a suitable technology for lymphedema management, the current commercially available bioimpedance analyzers are expensive, bulky, do not promote remote monitoring, and are unsuitable for a community-based environment such as homes or offices.
According to our knowledge, no work has been published in developing a low-cost, portable, and mobile-based lymphedema monitoring system. This study aims to evaluate the validity of the developed lymphedema device (Mobilymph) with the commercial Quadscan 4000 and determine whether Mobilymph can discriminate lymphedema status in healthy and BCRL participants. Mobilymph is a low-cost, portable (5 × 14 × 8 cm), and mobile-based lymphedema monitoring system (Fig. 1). Mobilymph measures the bioimpedance of the arms and transmits the measured data wirelessly via Bluetooth to an Android smartphone application.

Mobilymph lymphedema diagnosis and monitoring system.
Materials and Methods
Ethical approval
This study was conducted with approval from the Medical Research Ethics Committee, University of Malaya Medical Centre (MREC ID No.: 2020316-8181). All participants provided written informed consent.
Participants
Two groups of women were recruited in this study. Healthy group (n = 45) and unilateral breast cancer (UBC) patients who were referred to the outpatient clinic of the University of Malaya Medical Centre (UMMC) for lymphedema treatment. The breast cancer patients recruited were Stage 0 (n = 55), Stage 1 (n = 27), and Stage 2 (n = 18).
This study included participants older than 18 years of age. Participants who were pregnant or had cardiac or metal implants in the upper limbs were excluded. Specifically, the exclusion criteria for healthy participants are women with history of breast cancer, BCRL, and any medical conditions that could influence upper limb fluid volume. For the UBC participants, women who are diagnosed with bilateral BCRL were excluded from this study. The participant characteristics and UBC clinical characteristics are described in Tables 1 and 2.
Participant Characteristics
Unilateral Breast Cancer.
Dominant: Nondominant.
Unilateral Breast Cancer Participant Clinical Characteristics
Protocol
To obtain a standardized bioimpedance assessment, participants were asked to abstain from exercise, caffeine, alcohol, and meals 4 hours before the measurement. All jewelry was removed and the skin at the electrode sites was cleaned with an alcohol wipe before Ag–AgCl electrodes placement. Participants were seated comfortably throughout the assessment. The shoulder of the participants was flexed to 90° with forearm pronated, wrist in neutral, and fingers extended as shown in Figure 1. The measurement electrodes were placed at the mid-wrist of the ulnar styloid and the head of the humerus. The drive electrodes were positioned 8 cm distal to the measurement electrodes. The electrodes placement was chosen in preference to the standard shoulder to wrist sites. 25
Bioimpedance of healthy participants was measured using Mobilymph and commercial bioimpedance analyzer Quadscan 4000. The bioimpedance results collected from the two bioimpedance analyzers will be statistically analyzed. If there is no significant difference between the analyzers, only Mobilymph will be used to measure UBC participants' bioimpedance.
In this study, the protocols were specifically designed to evaluate the accuracy of Mobilymph bioimpedance measurements on healthy participants compared to the commercial Quadscan 4000. The second protocol is to determine the Mobilymph's sensitivity to distinguish between healthy and lymphedematous limbs participants. However, this study does not include the self-assessment of participants to use the Mobilymph at home.
Bioimpedance analyzer benchmarking
Mobilymph bioimpedance measurement was benchmarked with the commercial bioimpedance analyzer Quadscan 4000. The bioimpedance of the healthy participants' arms was measured at the frequency of 5, 50, 100, and 200 kHz. The measurements were collected using Quadscan 4000. After an interval of 5 minutes, participants were measured using Mobilymph.
Clinical measurements
Clinical lymphedema measurements were conducted on UBC participants using Mobilymph. Clinical assessments and classification of lymphedema were performed by trained UMMC physiotherapists. The classification of lymphedema is based on the physical examination and comparison of the circumferential upper limb volume. Stage 0 exists after surgery or radiation due to a damaged lymphatic system. In this stage, UBC participants are asymptomatic and show no clinical signs of lymphedema. Stage 1 UBC participant is characterized with mild lymphedema and circumferential interarm volume differences of 2–3 cm. In Stage 2, UBC participant is presented with moderate lymphedema with circumferential interarm volume differences of 3–5 cm. 4
Mobilymph was used to measure the bioimpedance of healthy and UBC participants' arms. The interarm bioimpedance ratio for UBC participants was determined by dividing the bioimpedance values of unaffected and affected arms. As for healthy participants, the interarm bioimpedance ratio was evaluated by dividing bioimpedance values of nondominant and dominant arms.
Statistical analysis
The healthy arms bioimpedance values from Quadscan 4000 and Mobilymph were analyzed using paired t-test.
Independent t-test was applied to determine the significant difference of interarm ratios between participants in healthy and Stage 0 (Category 1), healthy and Stage 1 (Category 2), Stage 0 and Stage 1 (Category 3), and Stage 1 and Stage 2 (Category 4).
Results
The developed Mobilymph and Quadscan 4000 bioimpedance analyzers demonstrated negligible bioimpedance mean differences. The results imply that the bioimpedance measurements were equivalent for both analyzers. The significance values and bioimpedance mean differences between Quadscan 4000 and Mobilymph are presented in Table 3.
Bioimpedance Analyzers Benchmarking
Ohm.
The interarm bioimpedance ratios measured using Mobilymph have shown significant difference in Category 2 (p < 0.001), Category 3 (p < 0.001), and Category 4 (p < 0.001). The interarm bioimpedance ratios in Category 0 were comparable (p = 0.63) with overlapping confidence intervals (Fig. 2). Table 4 summarizes the categories significant values.
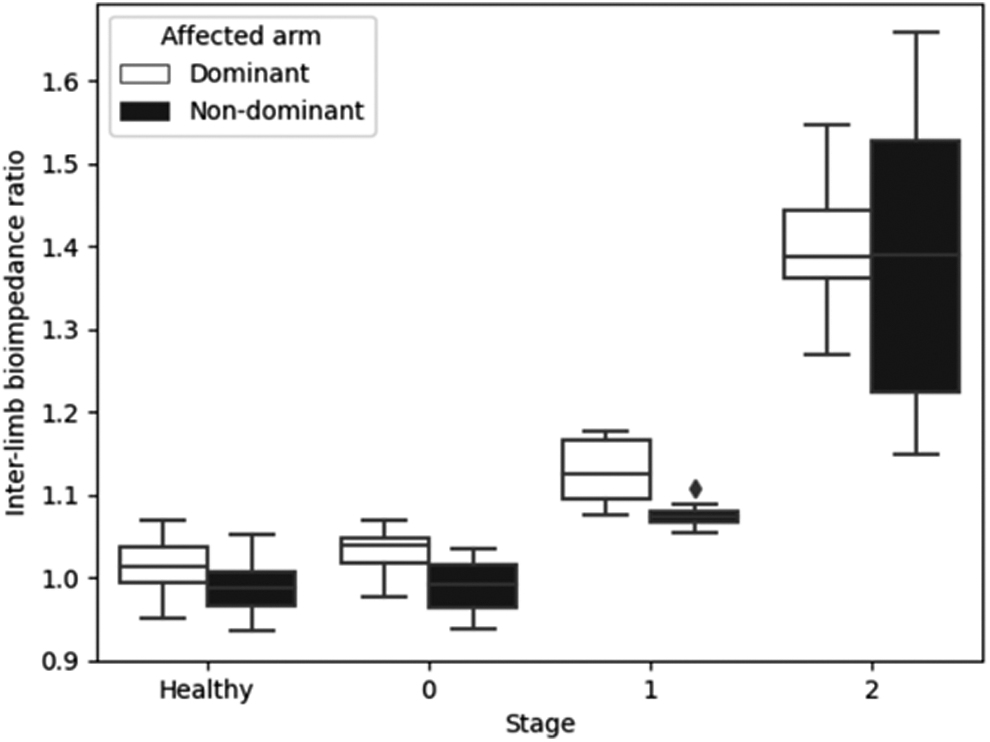
Upper limbs impedance ratios of healthy participants and UBC participants classified according to clinically assessed lymphedema stages. UBC, unilateral breast cancer.
Upper Limbs Impedance Ratios of Healthy Participants and Unilateral Breast Cancer Participants
Discussion
This investigation reveals that the developed Mobilymph bioimpedance measurements are equivalent to commercial Quadscan 4000 and that Mobilymph can distinguish between healthy participants (n = 45) and BCRL participants (n = 100) upper limbs.
Mobilymph capability to differentiate healthy and Stage 0 from Stage 1 participants' arms is crucial for early detection and immediate lymphedema treatment at an early and reversible stage.5,6 In contrast with healthy and Stage 0, the interarm bioimpedance ratios of Stage 1 and Stage 2 were more significant. The affected arm will have a smaller bioimpedance value than the unaffected arm due to the excess accumulation of lymph fluid in the affected arm. Therefore, the greater the lymph fluid accumulation in the affected arms the larger the interarm bioimpedance ratio 26 as shown in Figure 2.
The comparable interarm bioimpedance ratios between healthy and Stage 0 participants is expected as lymphedema is latent in Stage 0. Stage 0 BCRL patients will experience heavy sensations or numbness in the affected arm. However, swelling is not evident in the affected arm despite impaired lymph transport. 5 The results obtained in this study represent a clinically significant outcome, offering clinicians and patients the ability to use this approach for early lymphedema detection and treatment intervention.
A study by Ridner et al. showed that using BIA as a screening approach is effective in identifying BCRL patients in the early stage. The study found that early lymphedema treatment intervention was beneficial for patients identified using the BIA method and concluded that BIA is a standard method for prospective BCRL surveillance. 27 Soran et al. reported that early detection and care could reduce lymphedema incidence from 36.4% to 4.4%. 28 The efficacy of home monitoring and self-management for lymphedema may have beneficial impacts. This approach has been demonstrated to effectively prevent sequelae from several chronic diseases such as heart disease, diabetes, and obesity.29,30
Postoperative breast cancer patients in UMMC are required to regularly attend lymphedema rehabilitation clinics every week for the first 6 months. The visitation frequency will reduce to biweekly, monthly, and once in 3 months based on their clinical need. Lymphedema treatment can be highly costly and can give a negative impact on patients' quality of life. Despite technological advancement, people with low-to-middle incomes and those living in rural areas are unable to access affordable lymphedema monitoring systems. These highlight the need for accessible and affordable lymphedema monitoring system for breast cancer survivors. In this study, the developed bioimpedance analyzer Mobilymph has demonstrated its sensitivity in discriminating between healthy and lymphatics arms.
The Mobilymph system design has the potential to allow for self-measurement at home in the intervals between formal monitoring in the clinic. It can also be used in the clinical setting as a screening tool. The interarm bioimpedance ratio will be sent to physiotherapists and physicians to monitor lymphedema progression. This will allow BCRL patients to submit regular treatment feedback to the physiotherapists and enhance their commitment to self-management of lymphedema. 29 This approach could improve patient engagement in lymphedema management, ultimately reducing the costs associated with frequent clinic visits.
While the study demonstrates promising results, more research is needed to evaluate the long-term effectiveness of the Mobilymph system in preventing and managing lymphedema. Since this is a preliminary proof-of-concept study, the study did not consider various important factors such as patient's ability to self-measure and practicality of home use. However, these limitations will be addressed in the future study. Despite these limitations, the results of this study suggest that the Mobilymph system has the potential to be a valuable tool for early detection and management of lymphedema in breast cancer survivors. This could provide a low-cost treatment option and improve the quality of life for breast cancer survivors with lymphedema.
Conclusions
This study developed, tested, and validated a low-cost, portable, and mobile-based lymphedema monitoring system known as Mobilymph. The findings indicate that the bioimpedance measurements obtained using Mobilymph are comparable with the commercialized bioimpedance analyzer Quadscan 4000. Moreover, Mobilymph can differentiate between healthy and lymphedema limbs. Thus, the Mobilymph lymphedema monitoring system offers a new approach that enables early diagnosis and monitors the treatment efficacy at an affordable cost regardless of the environment.
Footnotes
Acknowledgment
The authors wish to thank the people who participated in this study.
Authors' Contributions
S.A.S.I.: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, and Writing—Original Draft.
F.I.: Conceptualization, Methodology, Formal analysis, Writing—Review and Editing, and Supervision.
N.A.M.T.: Conceptualization, Methodology, Resources, Writing—Review and Editing, and Supervision.
J.C.: Conceptualization, Software, and Writing—Review and Editing.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The research study was funded by RU—Geran University of Malaya Centre of Innovation and Enterprise (RU005A-2016 and RU007C-2017K).