
Abstract
Background:
Lymphedema and lipedema are debilitating conditions with no proven drug or surgical therapy. Effective treatment requires self-management through movement and compression to reduce limb volume and the incidence of cellulitis. The addition of personalized everyday physical activity (PA) could be transformative, increasing the therapy window to include all waking hours per week and enabling an increased dose of PA.
Aim:
This service evaluation aimed to determine the feasibility of LymphActiv as a treatment option for lymphedema and lipedema patients.
Methods:
This service evaluation followed an open observational cohort design, including 55 patients who participated in LymphActiv over 24 weeks. Patients wore an objective PA monitor and interacted with their data in an online dashboard, alongside remote mentor support. Primary outcomes were changes to PA, body weight, limb volume and quality of life. Clinical assessments occurred at baseline and after the 24-week program. Noncompleters were used as a quasi-control group for comparison.
Results:
Thirty-seven patients completed, of which 81% improved PA. On average, completers reduced their right and left lower limb volumes by −1.8% and −2.1%, respectively. Completers also experienced small average weight losses of −1.2 kg. Noncompleters experienced small average increases in each of these outcome measures.
Discussion:
These results establish the value of LymphActiv, providing benefit to patients who might otherwise have deteriorated. For services, this could lead to substantial cost-savings through reduced admissions, greater patient independence, and less need for community health care input. The next step is to undertake a randomized, controlled trial comparing the intervention with standard care.
Introduction
The lymphatic system is a network of vessels, independent of the blood circulation, connecting with lymph nodes. Changes in pressure generated by local muscle activity “massage” fluid both into and along the lymphatic vessels toward the lymph nodes. Movement and general body activity are critical for this process.
Lymphedema is fluid swelling of a part of the body resulting from a failure of lymph drainage. Lipedema is a condition characterized by disproportionate excess fat deposition not only on legs but also arms associated with pain and a lack of response to diet.
Lymphedema and lipedema can be extremely debilitating, and physical activity (PA) is a vital therapy to empower effective self-management of these conditions.1–3 Structured exercise alone is often daunting, and sometimes not appropriate, so the addition of personalized everyday PA can be transformative. 4
Obesity can promote lymphedema by impairing lymph drainage. 5 The worse the movement, the worse the obesity; the higher the weight, the worse the swelling; and the worse the swelling, the worse the movement, leading to a vicious circle. The same applies to lipedema.
This service evaluation looked at the value of monitoring PA and providing personalized feedback to the patient to empower them to understand what they need to do to be more active (and so stimulate their lymph drainage and burn calories). PA is defined as “any bodily movement produced by skeletal muscles which results in energy expenditure.” 6 As such, PA is not as daunting to patients as might be “exercise” or “sport.”
The intervention, known as LymphActiv, is a technology-enabled intervention designed for lymphedema patients. Data collected using a wrist-worn PA monitor were combined with personalized feedback displayed in an online dashboard and direct support from a remote human mentor. The power of the technology is not just to inform professionals but also to inform the patient. 7 It is felt that personalized feedback can empower the patient to make sustainable PA behavior change. It is not necessarily about conducting exercise, but simply keeping on the move, changing lifestyle, and reducing sedentary periods.
The aim of the evaluation was to determine the feasibility of LymphActiv as a treatment option to improve treatment outcomes in lymphedema. The hypotheses were as follows:
The use of LymphActiv will improve PA levels and reduce sedentary periods in lymphedema patients. The use of LymphActiv will reduce swelling in lymphedema. The use of LymphActiv will reduce weight in lymphedema patients who are morbidly obese. The use of LymphActiv will improve quality of life (QoL) in lymphedema patients.
Materials and Methods
The intervention
LymphActiv is a personalized and guided digital service provided by KiActiv,® which empowers people to optimize everyday PA in the context of their condition. KiActiv's patented technology evaluates minute-by-minute PA data from a validated wearable monitor, which is displayed instantly in a personalized online dashboard, and is available 24/7 to provide meaningful and actionable feedback. Patients are also supported remotely by a dedicated KiActiv Mentor at 9 key time points during the 24-week program, to help them build an understanding of the value of their daily activities and the confidence to plan, monitor, and improve.
Patient recruitment
Patients seen within the Lymphedema Clinic at St. George's University Hospital (SGUH) in London were considered for enrolment. Patients most suited to recruitment were considered those with moderately severe lymphedema of lower limb(s), who did not exercise much, lacked motivation to exercise, and were overweight. These criteria were subjective, but suitable recruits were agreed on by the clinical team. Exclusion criteria were as follows: <16 years old; body mass index (BMI) <35; and regular wheelchair users.
Experimental design
The design was an open service evaluation of the effects of the LymphActiv service intervention on improving physical outcomes and QoL in patients with lymphedema and/or lipedema. Movement and PA are cornerstones of lymphedema management to stimulate lymph drainage, but are often not embraced by the patient. LymphActiv was considered a means by which the patient could improve their PA, with associated benefits to their limb volumes and weight. After obtaining written consent, baseline measurements, including demographic details, were recorded. Patients then received their wrist-worn monitor. Telephone calls took place to explain the procedure and support interpretation of the personalized data feedback as patients progressed through the program. The contextualized feedback of data was considered the main incentive to patients to change their lifestyle and activity levels.
Patients wore a wrist-worn PA monitor continuously for 7 days, while blinded to the data, to record information on their “typical” weekly PA behavior before receiving contextualized data feedback to support positive behavior change. The baseline PA data included information on an individual's performance in relation to four independent PA dimensions:
Moderate activity: moderate-intensity PA relates to all activity in which patients are burning 3 × or greater the number of calories burnt at rest.
Nonsedentary time: the average amount of time patients spent not sitting or lying down (above their sedentary threshold; >1.8 × calories burnt at rest).
Calorie burn: the average number of calories burned per day.
Moderate bouts of activity: the average time per day performing bouts, sustained for 10 consecutive minutes or more, of moderate-intensity PA.
Once the baseline assessment week had been completed, feedback to the patient was provided through the online dashboard (a suite of digital tools that visually tracked, analyzed, and displayed key information for the patient to self-manage their performance) and one-to-one mentoring by phone call. This intervention was intended to increase levels of everyday PA. Further data were collected over the next 23 weeks using the wrist-worn monitor.
Patients were assessed for limb volume and weight changes during a face-to-face clinic visit. QoL was assessed using A Quality of Life Measure for Limb Lymphedema (LYMQOL). 8 LYMQOL is a tool to assess the impact of lymphedema on the patient's QoL. The questions cover 4 domains: Function, Appearance, Symptoms, and Emotion. Domain totals are calculated by adding the individual scores and dividing the total by the number of questions answered. There is also an overall QoL rating (0–10). To show improvement, the scores for the 4 domains would decrease and the score for overall QoL would increase.
Outcomes
Objectively assessed, minute-by-minute PA data in multiple dimensions throughout the intervention period. Body weight (and height), limb volume, and LYMQOL questionnaire were administered at baseline and 24 weeks.
Statistical analysis
Comparison was made between outcome measures at baseline and subsequent periods during the program. Incremental area under the curve was used to determine the average total PA dose achieved above baseline in each dimension during the 24 weeks. In addition, comparison was made between those patients completing the program and those who did not complete, but for whom data were available.
Ethics
The Institutional Ethics Committee at SGUH NHS considered this a service development and subsequent evaluation.
Results
Recruitment commenced in February 2020 and ran until September 2021. Most of this time coincided with the unprecedented COVID-19 pandemic. Fifty-five patients started LymphActiv. Thirty-seven completed (67%) and 18 (23%) did not complete LymphActiv. The 18 who did not complete LymphActiv continued to be seen in clinic and their data have been used as a quasi-control group where necessary for the purpose of improving performance of the lymphedema service.
Demographics
Forty-four patients (80%) were female with an average age of 54 years and a BMI of 45.4 kg/m2, respectively (Table 1). Thirteen patients had primary lymphedema, 26 patients had secondary lymphedema, and 16 had lymphedema associated with lipedema. All patients had lower limb lymphedema, except one with arm lymphedema following breast cancer.
Physical Characteristics at Baseline Assessment
Data are expressed as n (%) for biological sex, or as mean (SD) for other data.
BMI, body mass index; IMD, indices of multiple deprivation; SD, standard deviation.
Outcome 1: PA
Of completers (n = 37), 32 patients had sufficient PA data (>42 complete days) for analysis at 12 weeks, and 26 patients had sufficient PA data (>84 complete days) for analysis at 24 weeks. Of the 26 patients with sufficient PA data across the 24 weeks, 81% improved their PA and 65% improved in multiple dimensions. On average, participants improved in 2.4 out of 4 dimensions. No data on PA were available for noncompleters. Matched pairs t-tests were used to compare average daily PA across baseline week with new average daily PA across 12 and 24 weeks, respectively.
Moderate activity
Moderate-intensity PA relates to all PA in which patients are burning 3 × to 6 × the number of calories burnt at rest. The average amount of time spent in minutes of moderate-intensity PA was 39 minutes per day at baseline (n = 32), increasing to 51 minutes per day across 12 weeks (n = 32; p < 0.05), and maintained at 51 minutes per day across 24 weeks (n = 26; p < 0.05) (Table 2).
Group Mean Daily Physical Activity At Baseline Week, and Across 12 and 24 Weeks for Participants with Sufficient Data for Analysis
Data are expressed as mean (SD) for continuous data, or % increase for change from baseline.
Denotes statistical significance (p < 0.05) between group mean at baseline and group mean at 12 weeks.
Denotes statistical significance (p < 0.05) between group mean at baseline and group mean at 24 weeks.
Denotes statistical significance (p < 0.05) between group mean at 12 weeks and group mean at 24 weeks.
Nonsedentary time
The average amount of time patients spent above their sedentary threshold was 2 hours 49 minutes per day at baseline (n = 32), increasing to 3 hours 16 minutes per day across 12 weeks (n = 32; p < 0.05), and 3 hours 18 minutes per day across 24 weeks (n = 26; p < 0.05) (Table 2).
Calorie burn
The average number of calories burned per day at baseline was 3883 kcal (n = 32), increasing to 3996 kcal burned per day across 12 weeks (n = 32; p < 0.05) and 4009 kcal burned per day across 24 weeks (n = 26; p < 0.05) (Table 2).
Moderate bouts of activity
Average time spent in moderate-intensity activity performed in sustained bouts of 10 consecutive minutes or longer was 6 minutes per day at baseline (n = 32), increasing to 13 minutes per day across 12 weeks (n = 32; p < 0.05), and 26 minutes per day across 24 weeks (n = 26; p < 0.05). There was also a statistically significant difference in group average daily moderate bouts from weeks 12 to 24 (Table 2).
Outcome 2: limb volume
Limb volume was measured by the Lymphedema Team at SGUH at baseline and at follow-up appointments. COVID-19-induced closures of clinic, postponement of face-to-face appointments, and patients' reluctance to attend clinic during certain phases of the pandemic meant that the period between baseline and follow-up limb volume assessment varied greatly in this group. Treatment during this period was compression garments only.
Nevertheless, follow-up lower limb measurements were completed for 39 patients (completers, n = 30; and noncompleters, n = 9). Two patients were excluded from the completer group due to confounding treatments (bariatric surgery and liposuction). Likewise, in the group who started, but did not complete, two patients were excluded due to confounding treatments (decongestive lymphatic therapy and liposuction).
The results of a one-way analysis of covariance (ANCOVA) suggest a statistically significant difference between completers and noncompleters for right leg limb volume at follow-up (F[1,32] = 14.43, p < 0.05), when adjusting for variation between groups at baseline. For left leg limb volume, there was also a statistically significant difference between completers and noncompleters at follow-up when adjusting for variation between groups at baseline (F[1,32] = 19.35, p < 0.05; Fig. 1). Descriptive statistics show that noncompleters saw small increases in both right and left leg volume, whereas completers saw a small decrease over the 24 weeks (Table 3). These directional changes, combined with the results from both one-way ANCOVAs, show that completing LymphActiv had a statistically significant positive effect on bilateral limb volumes when compared to those who started LymphActiv, but did not complete.
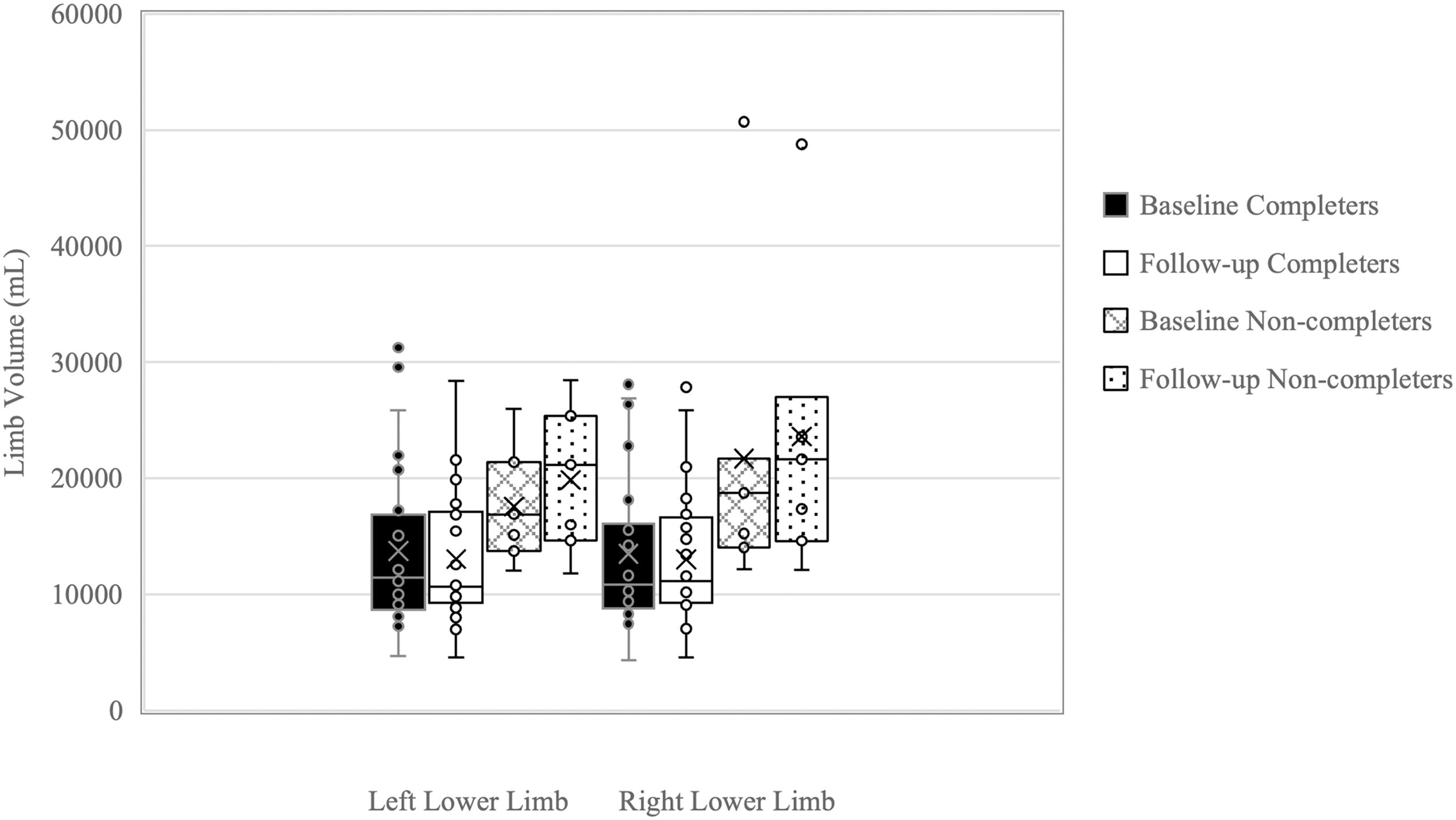
Lower limb volume for completers (n = 29) and non-completers (n = 7) at baseline and at follow-up. Left lower limb volumes represented by boxes 1–4 from left of figure. Right lower limb volumes represented by boxes 5–8 from left of figure. Black fill represents baseline for each limb, and white fill represents follow-up for each limb, for individuals who completed their respective programs. Cross-hatch fill represents baseline for each limb, and dotted fill represents follow-up for each limb, for individuals who did not complete their respective programs. “x” denotes group mean; “o” denotes individual data points. Horizontal line in each box denotes group median.
Volume Calculations for Each Lower Limb At Baseline and At 12-Week Follow-Up
Of the 28 patients with follow-up limb volume measurements, who completed LymphActiv, 19 (67.8%) improved their lower limb volume. Of the 7 patients with follow-up limb volume measurements, who did not complete LymphActiv, 3 (42.8%) improved their lower limb volume. There was no change in standard care.
Outcome 3: weight
Average weight change for the completers included (n = 30) was a loss of −1.3 kg, equivalent to a reduction of −0.7% of body weight. In comparison, average weight change for the 8 patients who did not complete LymphActiv, but were included in the weight analysis was an increase of +4.8 kg, equivalent to +3.2% of body weight (Fig. 2).
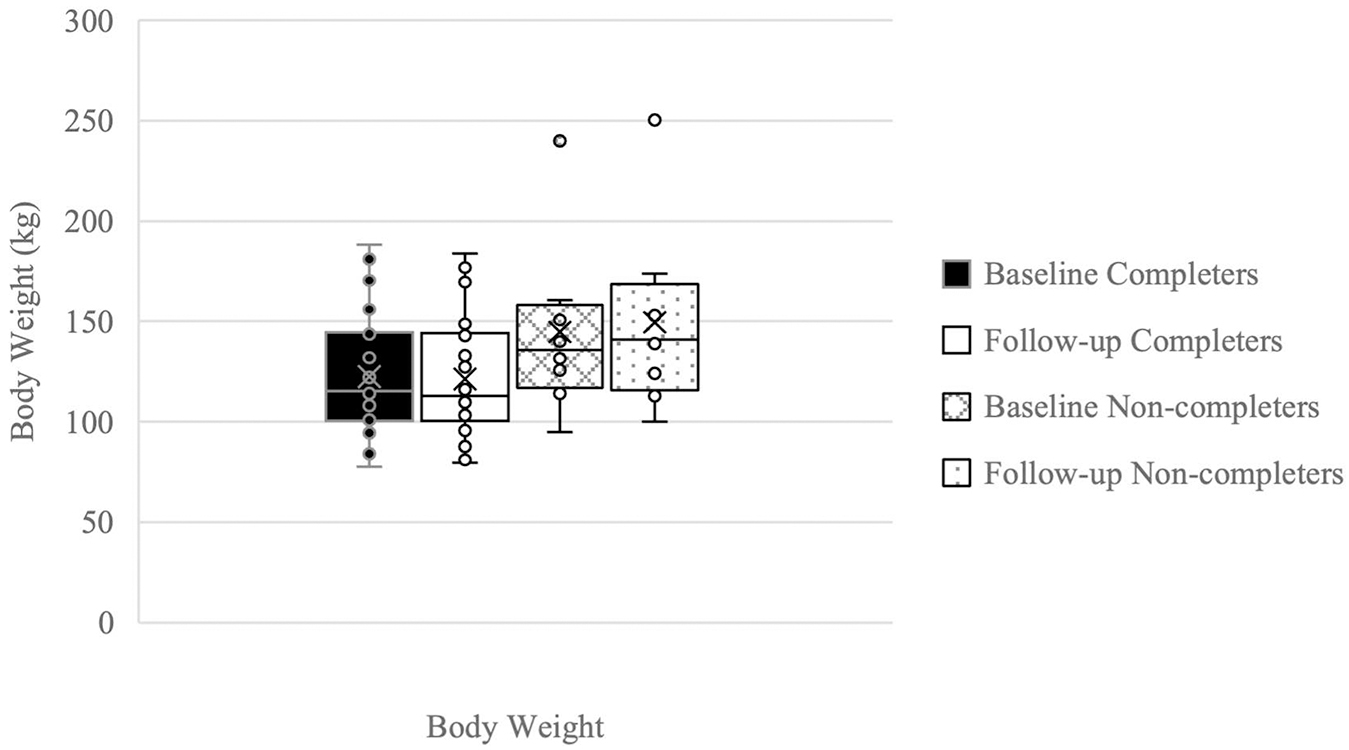
Body mass for completers (n = 30) and non-completers (n = 8), at baseline and follow-up (24 weeks). Black fill represents baseline body mass for completers, white fill represents follow-up body mass for completers. Cross-hatch fill represents baseline body mass for non-completers, dotted fill represents follow-up body mass for non-completers. “x” denotes group mean; “o” denotes individual data points; horizontal line in each box denotes group median.
The results of the one-way ANCOVA revealed a statistically significant difference between completers and noncompleters for follow-up body weight (F[1,35] = 5.97, p < 0.05), when adjusting for variation in baseline body weight between groups. Descriptive statistics show that noncompleters had a small increase in body weight, whereas completers had a small decrease over the 24 weeks (Table 4; Fig. 2). These directional changes, combined with the results from the one-way ANCOVA, indicate that completion of LymphActiv had a statistically significant positive effect on body weight when compared to those who started, but did not complete LymphActiv.
Means for Body Weight At Baseline and Follow-Up for LymphActiv Participants
Outcome 4: patient-reported outcome measures (LYMQOL)
A repeated-measures ANOVA determined that mean scores did not differ significantly across the 3 time points for any of the 4 domains or overall QoL in those with lymphedema of the leg. As such, the results for patients who have completed LymphActiv and LYMQOL Leg at baseline and 12 and 24 weeks (n = 25) are displayed in Table 5. Those who started, but did not complete LymphActiv did not complete LYMQOL assessment, which means there is no comparator group.
Means for LymQoL At Baseline, and 12 and 24 Weeks for Participants Who Completed LymphActiv
The impact of COVID
This study commenced shortly before the emergence of COVID-19 and continued during the pandemic with patients recruited and supported throughout. The pandemic deeply affected hospital services, which disrupted the acquisition of limb volumes and body weight, but did not prevent the delivery of the remote LymphActiv program. Further analysis was conducted on the cohort of LymphActiv completers who had been included in the follow-up limb volume analysis (n = 28), which revealed several interesting outcomes (Fig. 3).
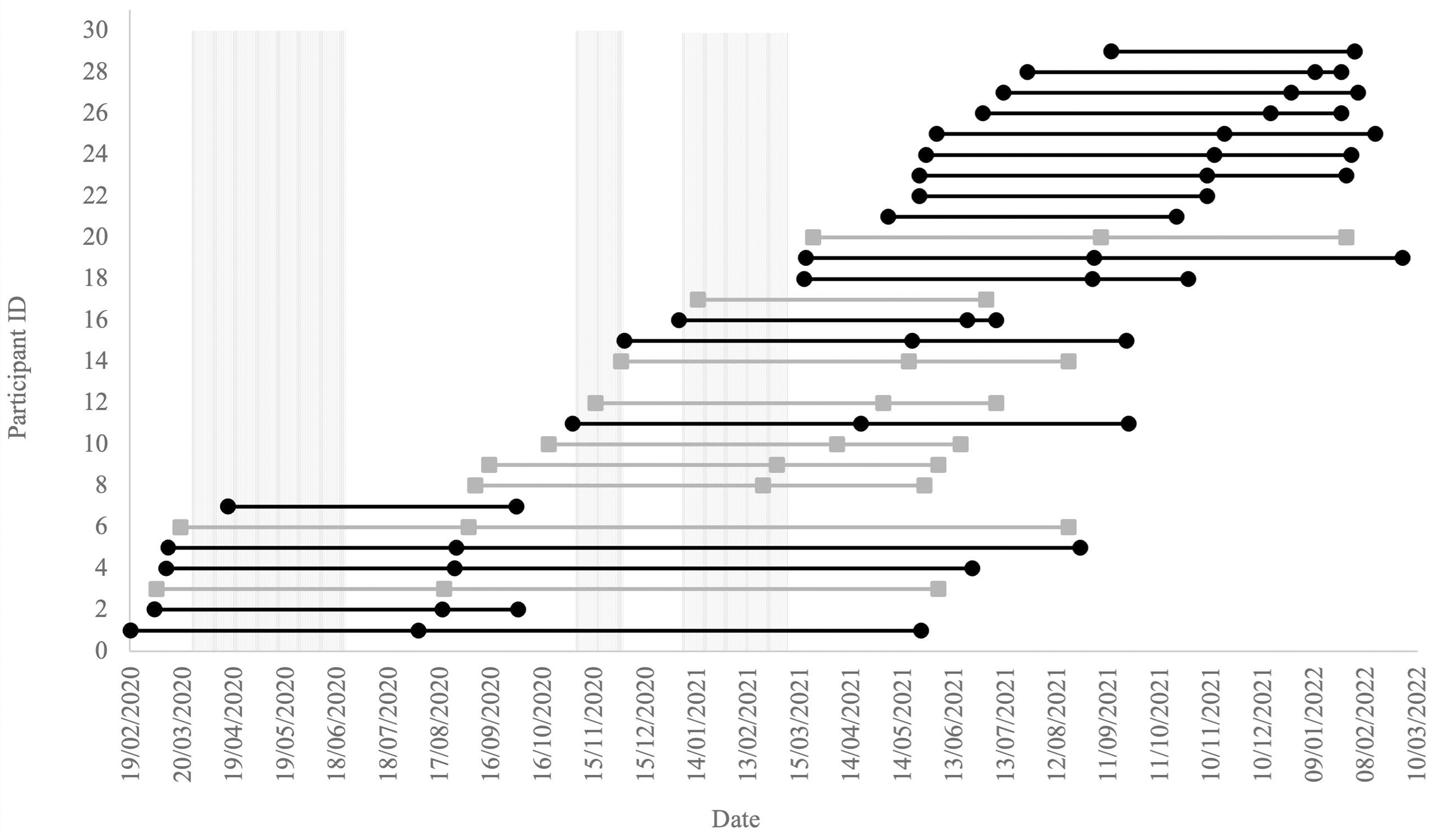
Reading left to right, markers denote start date, end date and 24-week follow up assessment date for participants who completed the 24 weeks and had a follow-up limb volume assessment (n = 28). Vertically shaded areas represent U.K.-wide lockdown periods. Black (with circular markers) indicates participants who improved limb volume. Grey (with square markers) indicates participants who did not improve limb volume. Participants are categorised into three subgroups: subgroup 1 (n = 7; Participant ID 1–7), those participating in LymphActiv program during first U.K.-wide lockdown; subgroup 2 (n = 9; Participant ID 8–16), those participating in LymphActiv program during second and third U.K.-wide lockdowns, and winter months; subgroup 3 (n = 12; Participant ID 17–29), those participating in LymphActiv program who were not impacted by any U.K.-wide lockdown restrictions. (N.B., participants with only two markers in this figure had follow-up assessment on the same day as 24-week end date).
Three distinct subgroups of patients were observed based on the date at which they started their LymphActiv program:
Subgroup 1 (n = 7): Those who were impacted by the first U.K.-wide lockdown.
Subgroup 2 (n = 9): Those who were impacted by both the second and third U.K.-wide lockdown, and the winter months.
Subgroup 3 (n = 12): Those who began after all U.K.-wide lockdown measures had been lifted.
Of the 12 completers who undertook the intervention after the lockdowns had ended, only one failed to improve their limb volumes. This compared with 8 of 16 who failed to improve when recruited during one or more of the lockdowns.
Discussion
Lymphedema and lipedema are more common than generally appreciated and can be extremely debilitating. Not only is swelling disabling but the high associated risk of infection in the form of cellulitis can be life-threatening. Lymphedema and cellulitis present an enormous challenge to health and social services in terms of both management and cost. A scenario frequently arises where the development of lower limb edema further compromises mobility, leading to further deterioration of the condition.
There is no proven drug or surgical therapy, and treatment relies on movement/exercise and compression. Sustainable treatment relies on self-management. Movement and PA are pivotal to that success. Structured exercise alone is often daunting, and sometimes inappropriate, so the addition of personalized everyday PA can be transformative. Finding ways to move more within the patient's existing daily routine enables utilization of the ∼112 waking hours per week, substantially increasing the therapy window and enabling an increased dose of PA. This is accessible and sustainable for everyone, regardless of age, surroundings, or mobility.
During the 24 weeks, 81% of patients who completed LymphActiv improved their PA. In comparison to other published interventions that utilized a wearable PA monitor, daily improvements to moderate-vigorous PA and nonsedentary time in this evaluation were twofold and threefold greater, respectively, among LymphActiv patients. 9 Given the widespread deterioration in PA levels reported at a population level throughout the pandemic,10,11 and the deterioration in self-care methods among lymphedema patients during this period, 12 these improvements are particularly impressive.
Using wearable monitors to capture and an online dashboard to present sophisticated multidimensional PA feedback combined with discrete mentor support may be a useful way of facilitating changes in behavior, and as a result treat disease where PA is desirable. Studies using the KiActiv technology in the management of other diseases such as cardiovascular disease have shown promise. 13 While mortality of sufferers from lymphedema is not known, it is likely to be higher than average, given the impairment to mobility that leg swelling creates, and the life-threatening infections that occur from the associated interference with local immunity. 14 Therefore, improvements in PA in this cohort of patients would be helpful.
There were limitations to this study. The initial plan was to test the feasibility of LymphActiv by seeing if the movement and exercise component of standard care could be better implemented, hence why it was initially considered a service development. Caution must be exercised when inferring the results from the comparator group as they were not randomized.
The program was an undoubted success, despite the noncompleters, who were undoubtedly disincentivized by the circumstances surrounding the pandemic. Overall, engagement with the intervention was good and withdrawal rate was low, relative to other published interventions employing similar digital technology. 15 Difficulties of attendance at hospital compromised the times at which data, for example, limb volumes and weight, could be collected and the lack of control data further limits interpretation. Nevertheless, this pilot study has established the value of this intervention in the care of lymphedema patients. The next step would be to undertake a randomized, controlled trial comparing the intervention with standard care. The results from this service evaluation can be factored in to future sample size calculations.
It is difficult to draw firm conclusions on the effect on weight. It is known that excess weight has a strong adverse effect on lymphedema, 5 so even small losses can be beneficial. Given the substantial weight gain in the noncompleters, an observation supported by a study showing that 63.1% of the 203 people with lymphedema surveyed had gained weight during the COVID-19 pandemic, 12 the small loss in the completers is most encouraging. Any intervention that reduces weight gain would be appealing, particularly one that does not have time/cost implications on services.
In conclusion, these results indicate that LymphActiv provided benefit to lymphedema sufferers who might otherwise have deteriorated. Such benefit should reduce the need for hospital-based care and the risk of worse swelling and infections such as cellulitis. At a service level, this intervention may lead to substantial cost-savings as a direct result of reduced hospitalizations, greater patient independence with more self-management, and less need for community health care input.
Footnotes
Acknowledgments
We acknowledge the essential contributions of the entire SGUH Lymphoedema and Lipoedema department team and the KiActiv team throughout the service improvement evaluation. We thank Dr. K. Riches and Prof. V. Keeley for providing guidance and invaluable editorial support. We also want to extend our gratitude to all participants who kindly gave their time and shared their experiences and feedback, which was crucial to the success of the service improvement evaluation.
Authors' Contributions
P.S.M.: Conceptualization (lead), methodology (equal), data analysis (lead), writing–original draft (lead), and review and editing (equal). M.P. and P.G.: Conceptualization (support), methodology (equal), data analysis (supporting), and review and editing (equal). K.R.: Review and editing (equal). V.K.: Conceptualization (supporting), data analysis (supporting), and review and editing (equal). K.F.T.: Conceptualization (supporting), data analysis (supporting), writing–original draft (supporting), and review and editing (equal). E.J.C.: Data analysis (supporting), writing–original draft (supporting), and review and editing (equal).
Author Disclosure Statement
K.F.T. is Lead Scientist and Lead Mentor for KiActiv, and E.J.C. is Informatics Lead for KiActiv. All other authors report no conflict of interests and have nothing to disclose.
Funding Information
This service improvement evaluation was funded by the St. George's Hospital Charity (Registered Charity No.: 1171195) and the Bernard and Joyce Coleman Charitable Trust (Charity No.: 1075731).