
Abstract
Lymphedema is a chronic condition characterized by dysfunction of the lymphatic system. There is currently no available cure. The standard of care is complete decongestive physiotherapy performed by a lymphedema therapist. However, lymphedema may flare between appointments, making home care important. There are several medical devices available to treat lymphedema at home, but they can be expensive, noisy, and bulky, restricting patient mobility. Thus, there is a demand for other devices that can be utilized at home, between appointments. The overall goal of this research study is to assess the safety of a newly developed vibratory device that may be utilized to supplement lymphedema treatment. Fourteen healthy subjects were recruited and treated with the device, all while measuring pre-treatment and post-treatment upper extremity circumference/induration, vital signs, pain, side effects, and intra-treatment acceleration produced by the device. There were no significant changes in reported pain or vital signs, and side effects were largely mild and transient. We believe that this device is safe for use in healthy subjects, and further studies should assess the efficacy of this device in treating patients with lymphedema.
Introduction
Lymphedema is a chronic condition characterized by the buildup of protein-rich fluid in interstitial spaces, manifesting as bothersome swelling. There are several causes of lymphedema, but it typically arises due to damage or dysfunction of the lymphatic system, which can be subdivided into primary and secondary causes. Primary lymphedema is due to underlying genetic mutations, often leading to malformation and malfunction of the lymphatic system. Secondary lymphedema, the most common type of lymphedema, is caused by various types of external damage or injury to the lymphatic system and is most widely seen in the oncologic population. This frequently occurs due to invasive surgery to remove tumors or diseased lymph nodes or radiation causing irreversible fibrosis. In fact, it is estimated that approximately 1 in 5 women who survive breast cancer will go on to develop lymphedema. While the underlying etiology of lymphedema may vary, all lymphedema is staged in the same fashion, falling anywhere from Stage 0 to Stage 3. Stage 0 represents an “at-risk” state, where an individual has risk factors associated with the development of lymphedema, and Stage 3 represents a stage of lymphostatic elephantiasis. 1
Lymphedema in and of itself can be uncomfortable, if not downright painful. However, it also predisposes patients to developing secondary vascular, inflammatory, and infectious conditions as it progresses and becomes increasingly severe. In addition, it may undermine patients’ body image and self-esteem and affect their daily lives and personal relationships. 1 Currently, once lymphedema develops, there is no definitive cure, only symptom management. The standard of care involves weekly or biweekly visits to a lymphedema therapist, an individual who has undergone specialized training to treat lymphedema. They most often practice complete decongestive physiotherapy, which combines modalities of compression, vibration, and massage. The massage, termed manual lymphatic drainage, consists of loosening stagnant lymphatic fluid and physically moving it to the next cluster of functioning lymph nodes. 2 While this practice is generally very safe, patients may experience side effects of a skin tingling sensation or mild dizziness. 3 Generally, these are regarded as therapeutic effects resulting from activation of the lymphatic system. Other, much less common effects may include headache, shortness of breath, or nausea.4,5
However, lymphedema tends to recur between appointments, making home care extremely important. Patients typically wear prescription-grade compression garments and are often taught techniques by their lymphedema therapist to perform at home. Unfortunately, compression garments can be uncomfortable and difficult to put on, factors that tend to decrease rates of patient compliance. 6 Some patients may also elect to use medical devices developed solely for the home treatment of lymphedema. The most frequently utilized devices use pneumatic pumps to sequentially fill air bladders along the length of the affected body part. Unfortunately, these devices can be bulky, noisy, expensive, and require long periods of immobility while treatment takes place. There is no “ideal” solution to the home treatment of lymphedema, which causes inter-appointment lymphedema exacerbation and overall poor quality of life for the many patients who are affected by this condition. 7 Because of this, there is a definitive need for new lymphedema technology that can improve patients’ symptoms while being easier and more user-friendly than previous products.
We have developed a wearable, therapeutic device (LymphaVibeTM) that utilizes vibration to treat upper extremity lymphedema (Fig. 1). The device is composed of eccentric rotating mass (ERM) vibration motors (NFP-E1015, NFP Motor) that are embedded into a retaining garment (90% polyester and 10% spandex) and activated in custom patterns designed to mimic manual lymphatic drainage massage. The exact placement of the motors is aligned with target lymph nodes, and the vibration intensity and frequency can be tailored to the patient’s stage of lymphedema and clinical response to treatment. Donning and doffing the device is simple; the patient slips their arm into a sleeve and tightens the fit using Velcro® straps. In previous benchtop testing, we were able to demonstrate that these ERMs are comparable to clinically used handheld massagers. 8 The overall goal of this research study is to assess the safety of this novel device in healthy participants.

Photos of the LymphaVibe secured on the arm.
Materials and Methods
This safety study was approved by the Virginia Tech Institutional Review Board (IRB Protocol 23-437). We recruited 14 healthy subjects (7 male and 7 female) from the local community. After informed consent was obtained, the research team collected and recorded a series of pretreatment measurements. Each research participant’s arm was marked at the palmar crease and in 10 cm increments up to 40 cm. Arm circumference was measured at each point (in centimeters) and induration was measured at the 20-cm point using an indurometer. Participants were asked to rate their pain on a standard 10-point scale, and their vital signs, including blood pressure, respiratory rate, oxygen saturation, heart rate, and temperature were measured using the appropriate medical equipment.
After pretreatment measurements were taken, participants were randomized to have the device placed on either their right or left arm, with equal numbers of participants receiving each treatment. The device was then secured with Velcro straps and turned on to cycle through a set sequence of vibrations. The device cycles through a series of five total phases for a 36-minute total treatment. The first phase is the distal preparation phase. This phase lasts for 7 minutes and consists of all distal motors, 1–4, being on for the entire phase (Fig. 2). This is followed by the proximal preparation phase, which lasts for 7 minutes and consists of all proximal motors, 5–8 being on. Then, the device moves to the decongestion phase, where moving proximal to distal, motor 8 to 1, the motors are turned on for 30 seconds and then turned off before moving to the next motor pair. This is followed by the clearing phase (total time: 4 minutes). Moving distal to proximal, motors 1–8, the motors are turned on for 30 seconds then turned off before moving to the next motor pair. Finally, the sequence ends with the reabsorption phase (total time: 14 minutes). Moving distal to proximal, motors are turned on at different intensities mimicking a wave pattern. The pattern moves up the arm for 16 cycles. At any point during this sequence of vibrations, research participants were told they could elect to end the treatment. In addition, an accelerometer (MetaMotionC, MBientLab) was placed within the sleeve at the proximal forearm between motors designated 3 and 4 prior to the start of treatment. Using the MetaWear app, accelerations were collected in the X, Y, and Z axes with a sampling rate of 200 Hz for approximately 1 minute during the decongestion phase of treatment. Data were collected while motors 3 and 4 were activated to capture the maximum acceleration values produced.

Schematic representation of motor positioning inside the device. Used with permission from Thomas, et al., 2023.
After the device completed treatment, the research team repeated and recorded the same measurements taken during the pretreatment phase. In addition, participants were asked to report any side effects that they may or may not have experienced, which could include a skin tingling/crawling sensation, pain/swelling at the treatment site, dizziness, nausea, headache, and shortness of breath. Data were compiled and analyzed using a paired, two-tailed t-test. The acceleration data were processed in MATLAB, where a magnitude of acceleration was determined during the time that motor was running, and a Fast Fourier Transform was used to calculate the frequency of the motors.
Results
All 14 subjects received treatment with the novel device. No participants elected to terminate the treatment session early due to perceived side effects or pain. The device’s battery ran out during the treatment session for one of the participants, at which point it was difficult to say where in the treatment cycle it had terminated. Nevertheless, their posttreatment measurements were obtained as stated in the protocol.
In all subjects, there were no significant changes to upper extremity circumference at any of the marked locations, including the palmar crease, 10 cm, 20 cm, 30 cm, or 40 cm (p = 0.33, 0.82, 0.46, 0.78, and 0.46, respectively, Fig. 3a). There was also no significant change in upper extremity induration pre- and posttreatment (p = 0.50, Fig. 3b). All participants reported a pretreatment pain level of 0/10 (as measured on a 10-point Likert scale). Twelve out of 14 participants reported a post-treatment pain level of 0/10, and two participants reported a posttreatment pain level of 1/10 and 2–3/10, respectively. However, there was no significant change to participant perceived pain levels (p = 0.19, Fig. 4a). There was no vital sign instability associated with the use of the device, with no significant changes seen in systolic blood pressure, diastolic blood pressure, heart rate, oxygen saturation, respiratory rate, or temperature (p = 0.10, 0.80, 0.79, 0.19, 0.61, and 0.15, respectively, Figs. 4b–4f).
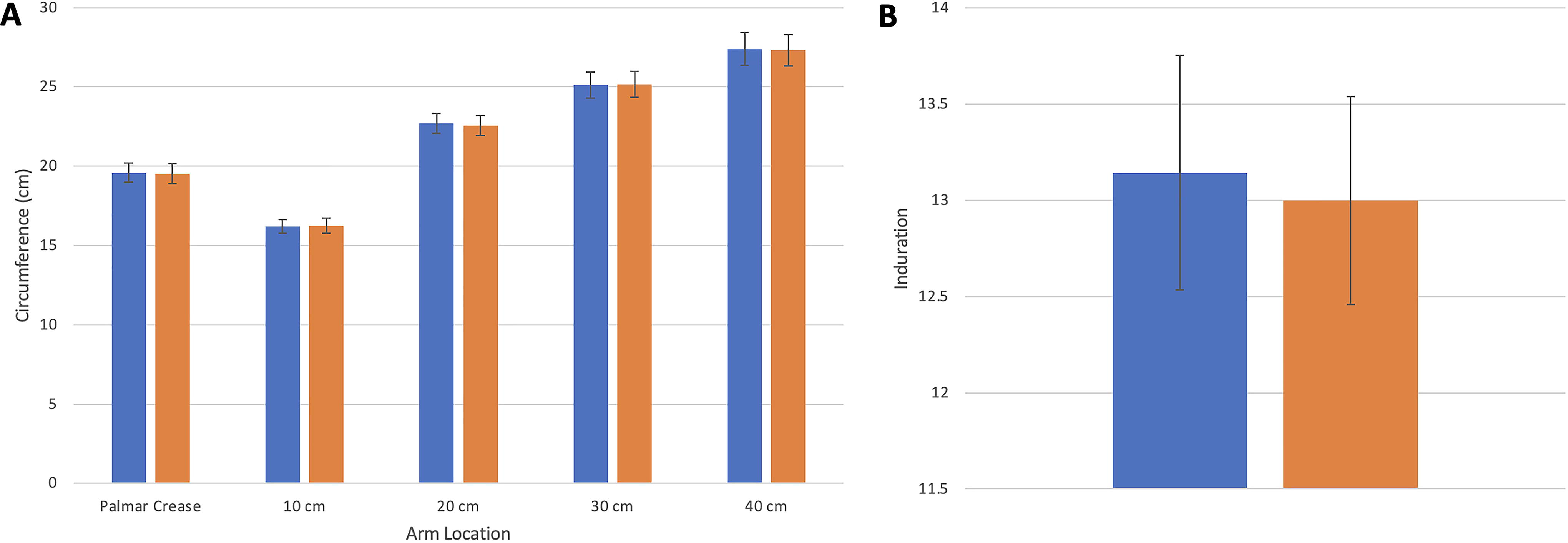
Pre- and Posttreatment Arm Measurements—
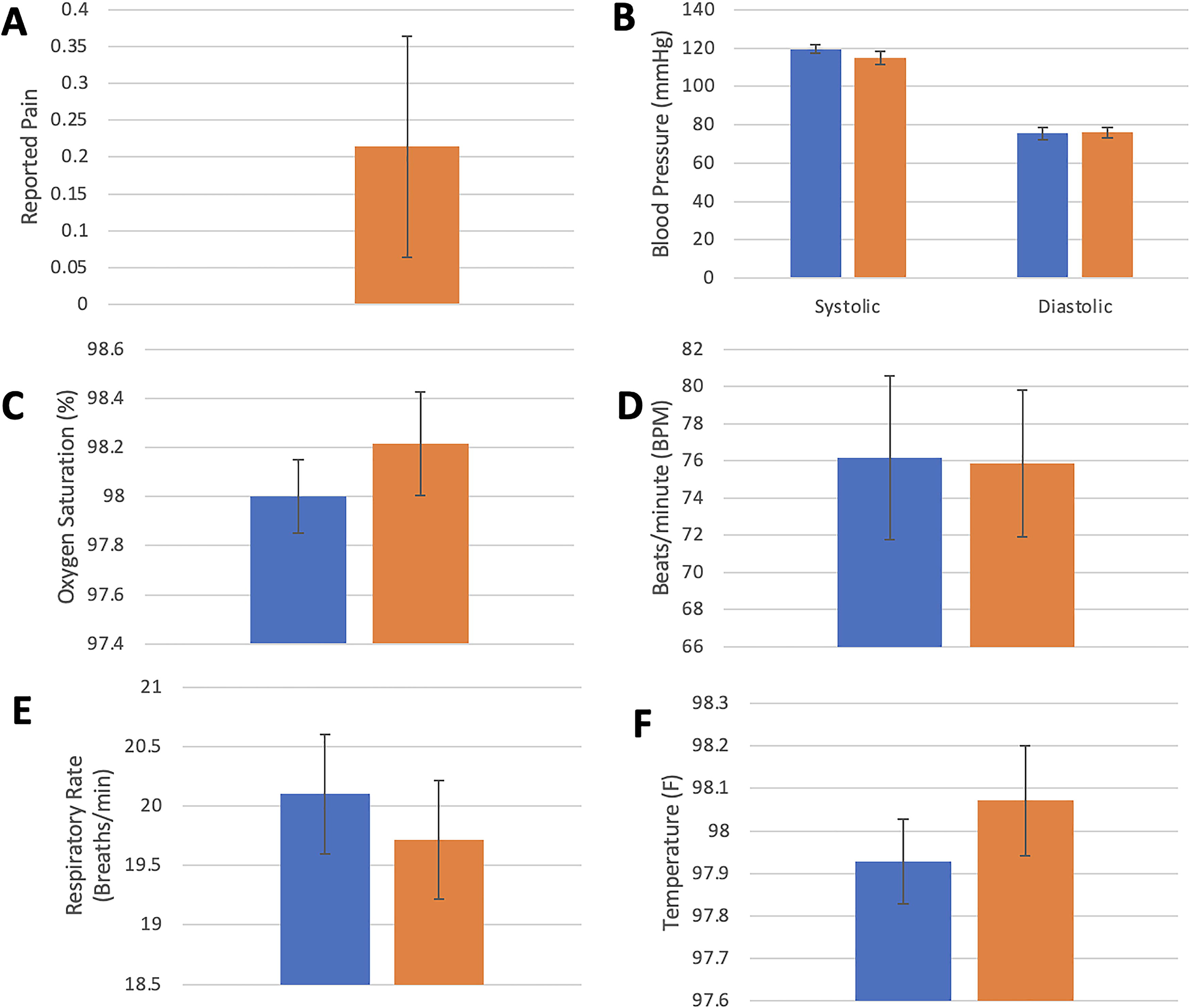
Pre- and Post-Treatment Pain and Vitals—
Out of 14 subjects, 5 did not report any side effects, and 9 did. Please see Table 1 for a full list of the side effects reported. The participants who did report side effects largely reported anticipated potential side effects. There were no adverse events.
List of Side Effects Experienced by Research Participants
Analyzing the results of the healthy subject test, the motors produced an acceleration of 0.4964g at a distance of approximately 75 mm. Bench testing conducted prior to this study showed that the vibration tool commonly used in clinical practice produced an acceleration of 0.4973g at a distance of 75 mm. Therefore, our motors are producing results nearly identical to that of the vibration tool. 8
Discussion
Secondary lymphedema, the most common form of lymphedema, affects approximately 1 in 1000 Americans. 1 There is no definitive cure, thus making management of this condition even more important. While complete decongestive therapy has been shown to be effective in several trials, it must be done consistently to maintain results. 9 This poses several issues of accessibility. Many times, insurance companies limit the number of approved lymphedema therapy visits causing patients to stretch out the timing between appointments, which may worsen symptoms. In addition, patients living in rural or isolated areas may not have access to a trained lymphedema therapist in their area. Both issues underscore the importance of home care in decreasing lymphedema burden. While therapist taught skills and compression garments are a mainstay of home care, it may be greatly improved using wearable devices for at home use, such as the one being tested in this study.
Normally, health care providers who care for lymphedema patients, including lymphedema therapists, measure limb circumference and induration as part of the treatment process to both stage lymphedema and assess treatment success. 10 Since the eventual goal of this device is to aid in this treatment, we took similar measurements as part of the study. Our research participants had healthy lymphatic systems (as indicated by their answers to inclusion/exclusion criteria questions). Therefore, they had no pooling of lymphatic fluid that could be moved by our device, leading to no significant changes in upper extremity circumference or induration, which was to be expected.
Assessment of pain was also an important part of our research study. While the use of some medical devices can be uncomfortable or slightly painful, it is important that therapeutic potential is not overshadowed by a painful patient experience. In addition, compared to healthy individuals, lymphedema patients are more likely to have associated pain. Approximately 35% of patients with lymphedema report being treated for pain, and this pain is often caused by stretching of soft tissues, which can occur during lymphedema treatment and potentially treatment with this device. 11 There was no significant difference in pre- and posttreatment pain measurements, but two participants did report a slightly elevated pain score after treatment with the device. This perceived pain was not great enough to prompt research subject withdrawal. Each research participant received the same vibration duration and intensity using a 5 V energy source. As determined by previous experiments, this is comparable to the highest intensity that could be produced by commercially available handheld massagers (D-Actor/V-Actor [K173692] and Norco NC70209 Mini Massager) used in lymphedema treatment. 8 Research participants also wore the same size sleeve for the sake of consistency, despite having different arm circumference measurements. Because of differences in anatomy and positioning of the ERM motors along the arm in combination with the high vibration intensity, this could have produced a sensation of pain. However, in practice, both vibration frequency and intensity as well as the size of the device sleeve would be tailored to fit a particular patient’s needs in treating their lymphedema, therefore minimizing the potential for a painful experience.
Overall, there was no vital sign instability associated with the use of this device. There were some nonsignificant vital sign changes; however, many factors influencing vital signs were not controlled for in this study, including caffeine consumption, BMI, and time of measurement. 12 While our device had some side effects, they were regarded as mild by the participants, as no one deemed them excessive enough to terminate the treatment session. All participants that had side effects reported quick resolution after cessation of treatment. The most common side effect reported was a skin tingling or crawling sensation, with five out of the nine participants who reported a side effect, indicating this. However, considering that skin tingling and dizziness are both side effects of complete decongestive physiotherapy, it may be regarded as more of a therapeutic effect. Gentle vibration activates the lymphatic system, increasing lymphatic flow through existing vessels, which is often perceived by the individual as a skin tingling or crawling sensation. 3 Thus, this side effect is simply a demonstration that the lymphatic system is functioning properly and doing its job, and this can be seen as a therapeutic effect instead of a side effect. 2 In addition, conditions that would automatically cause withdrawal of patients from the study without their consent, including bruising or bleeding, pain not alleviated by loosening the device, and skin rash or irritation, did not occur. Finally, as mentioned previously, the device was running at a high intensity, which may indicate that this is the most severe side effect profile that we would expect to see.
Considering the results of this research study, we believe that this device is safe to use in healthy adults. With this consideration in mind, we hope to move on with testing this device in patients with lymphedema to assess its ability to decrease upper extremity lymphedema in a clinic population before it can be made widely available for at-home treatment of lymphedema.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Author Disclosure Statement
The authors have no conflicts of interest.
Funding Information
This device was developed with funding from Carilion Clinic Innovations.