
Abstract
Background:
Research has indicated a link between obesity and a greater likelihood of venous disorders. However, the specific relationship between obesity in children and conditions such as phlebitis and thrombophlebitis remains undetermined. To explore this, we undertook a two-sample Mendelian randomization (MR) study to investigate the possible causal impact of childhood body mass index (BMI) on the development of phlebitis and thrombophlebitis.
Methods:
This study utilized genome-wide association studies data from European populations. Childhood BMI was assessed in a sample of 39,620 individuals, while data on phlebitis and thrombophlebitis were obtained from 1613 cases and 335,586 controls. We selected 16 single nucleotide polymorphisms significantly associated with childhood BMI as instrumental variables (IVs). The inverse variance weighting (IVW) method was applied as the primary approach, with weighted median, MR-Egger regression, and weighted mode methods used as complementary analyses.
Results:
The IVW analysis indicates a significant causal link between childhood BMI and the occurrence of phlebitis and thrombophlebitis (Beta = 0.002739, Standard error (SE) = 0.000740, p = 0.0002147). Results from the weighted median method (Beta = 0.002446, SE = 0.001046, p = 0.01933) aligned with the IVW findings. However, the MR-Egger and weighted mode analyses did not show a significant association (p = 0.1051 and p = 0.2525, respectively). Leave-one-out sensitivity tests and heterogeneity assessments were performed, revealing no evidence of horizontal pleiotropy.
Conclusion:
The findings from the MR analysis suggest a potential causal relationship between childhood BMI and an elevated risk of phlebitis and thrombophlebitis. This study provides new insights into the impact of childhood obesity on venous health, emphasizing the need for early intervention and prevention strategies.
Introduction
Body mass index (BMI) is a widely used anthropometric measure that assesses an individual’s body weight relative to height, providing a simple indicator of whether a person is underweight, normal weight, overweight, or obese. BMI is calculated by dividing a person’s weight in kilograms by the square of their height in meters (kg/m2). It serves as a reliable screening tool for categorizing weight status and assessing potential health risks associated with undernutrition and overweight conditions.1–3 Childhood obesity, which is characterized by a high BMI for age and sex, has become a global public health concern. Over the past few decades, the prevalence of childhood obesity has increased dramatically across both developed and developing countries, largely due to shifts in dietary habits, physical inactivity, and an increase in sedentary behaviors. According to recent epidemiological studies, the global prevalence of overweight and obesity in children aged 5–19 years has risen from 4% in 1975 to over 18% in 2016. This alarming trend indicates that millions of children are now facing an elevated risk of various obesity-related health complications. 4 The growing rate of childhood obesity is associated with significant short- and long-term health consequences. Children with obesity are at increased risk of developing metabolic disorders such as type 2 diabetes, hypertension, and dyslipidemia, as well as respiratory issues like obstructive sleep apnea and asthma. Additionally, childhood obesity has been linked to early onset of cardiovascular diseases, musculoskeletal problems, and psychological disorders, including anxiety and depression. If not managed effectively, these conditions often persist into adulthood, contributing to an increased likelihood of chronic diseases and a reduction in overall quality of life.5–7
Phlebitis is characterized by pain and inflammation in a vein without the presence of a thrombus. Thrombophlebitis involves vein inflammation accompanied by thrombosis, a relatively common peripheral vascular disease, primarily affecting the superficial veins of the extremities. Deep vein thrombosis can affect deep veins anywhere in the body, but it most commonly involves the lower limbs. Thrombophlebitis is a serious condition that can lead to complications such as cerebral embolism, pulmonary embolism, lower limb amputation, and even sudden collapse.
Obesity in patients can lead to increased venous pressure and a tendency for blood to pool in the lower extremities. This condition often results in the formation of blood clots within the venous system, potentially causing thrombophlebitis. Several studies have identified obesity as a contributing factor to venous thrombotic diseases.8,9 Consequently, a strong suggestion has been made regarding the association between BMI, as an indicator of obesity, and the occurrence of phlebitis and thrombophlebitis. There is, however, a need for further investigation to establish a causal relationship. Traditional retrospective studies, which typically rely on observational or randomized controlled trial designs, face challenges such as reverse causality and confounding factors. These challenges can be effectively mitigated through Mendelian randomization (MR) analysis. MR is a method that uses genetic variants associated with an exposure to investigate potential causal relationships between the exposure and an outcome. Because genetic variants are randomly allocated at conception, MR reduces the biases often seen in observational studies, such as confounding and reverse causation. This makes MR a powerful tool for assessing causality in clinical and epidemiological research.10–12 In this study, two-sample MR (TSMR) was utilized to explore the possible causal connection between childhood BMI and the development of phlebitis and thrombophlebitis.
Materials and Methods
Study design
In our research, a TSMR was employed to assess the causal link between childhood BMI and phlebitis and thrombophlebitis, using single nucleotide polymorphisms (SNPs) as instrumental variables (IVs). 13 To ensure the precision of our results, it was essential to verify three key hypotheses throughout the study. 14 First, the chosen IVs must have a direct association with childhood BMI. Second, these IVs should be free from any confounding factors that might affect both the exposure and the outcome. Third, the influence of the IVs on phlebitis and thrombophlebitis should occur exclusively through childhood BMI (Fig. 1). For the exposure data, we utilized publicly available summary statistics from genome-wide association studies (GWAS) meta-analyses (with a sample size of 39,620; GWAS ID: GCST90002409). The summary statistics for phlebitis and thrombophlebitis were obtained from the Neale Lab, comprising data from 1613 cases and 335,586 controls (GWAS ID: ukb-a-537).
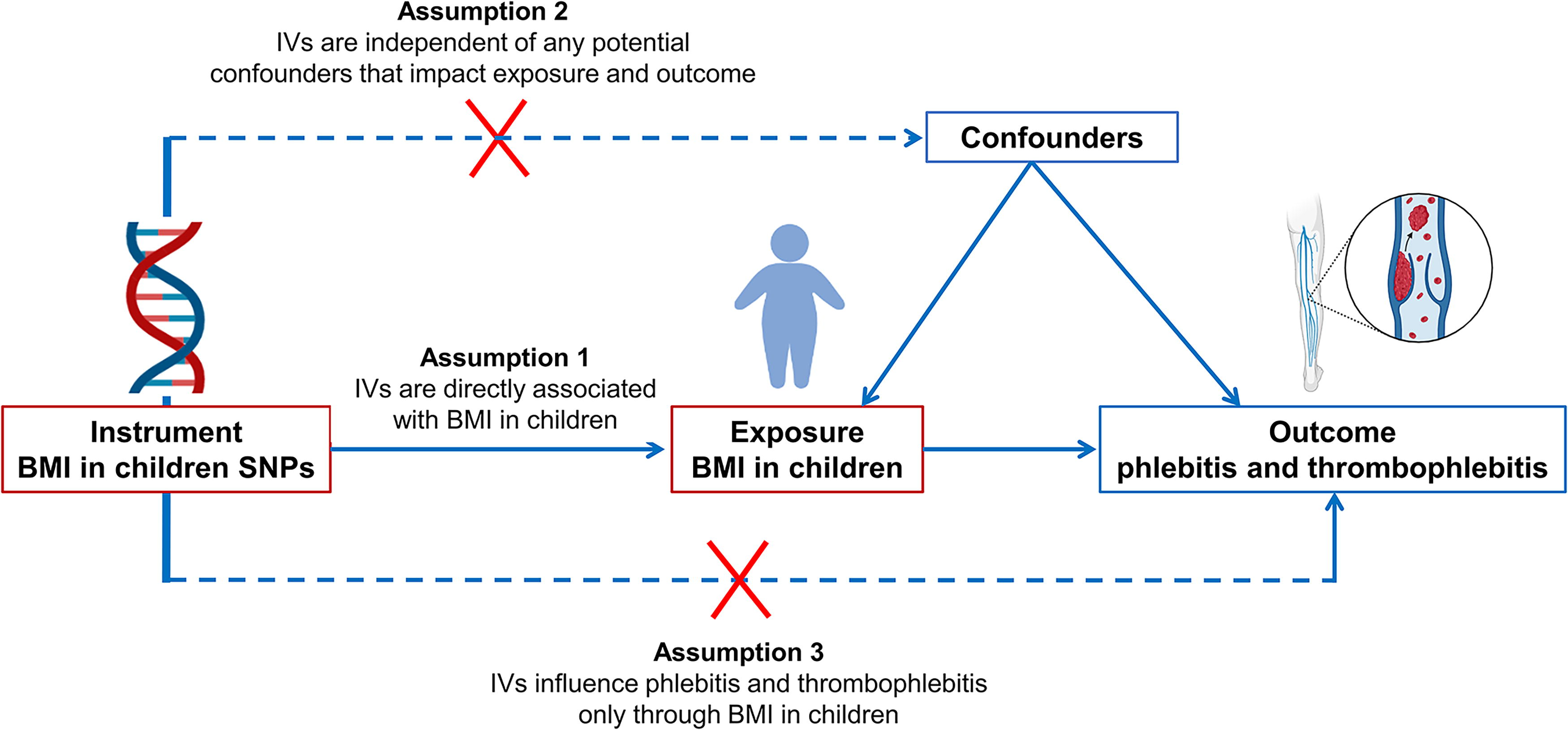
Graphic illustration of a TSMR analysis examining the link between childhood BMI and phlebitis and thrombophlebitis. TSMR, two-sample Mendelian randomization.
GWAS datasets offer robust instruments for MR analyses. We sourced Childhood BMI-associated SNPs from the GWAS database under the identifier “ebi-a-GCST90002409” which includes data on 39,620 children of European descent. For genetic association data on phlebitis and thrombophlebitis, we used the GWAS identifier “ukb-a-537” within the same database. This dataset encompassed 1613 individuals diagnosed with phlebitis and thrombophlebitis and 335,586 healthy controls, all from European populations. To meet the criteria that the genetic variants in the TSMR analysis must be strongly associated with childhood BMI, SNPs significantly linked to the exposure factor were selected using a genome-wide threshold of p < 5e-08. Additionally, we assessed the strength of each SNP using the F-statistic. An F-statistic lower than 10 indicated a high risk of bias in the causal effect estimate. Therefore, to minimize the potential for weak IV bias, SNPs with inadequate strength were excluded from our analysis.15,16
Statistical analysis
Linkage disequilibrium assessment
To mitigate bias arising from linkage disequilibrium (LD) among SNPs in our analysis, we calculated the LD coefficient (r2) and the extent of the LD region. We established criteria such that when the r2 value was <0.001 and the width of the LD region extended to 10,000 kb, the SNPs in question could be considered independent of each other. This approach ensured that our analysis was not confounded by SNPs that were closely linked genetically. 17
TSMR analysis
In this study, the primary methodology for estimating the causal relationship was the inverse variance weighting (IVW) method. 18 IVW is a robust approach for discerning causal relationships, leveraging the IV properties of genetic variants. This method is particularly preferred in TSMR analyses. In TSMR, IVW assumes that the genetic variants impact the outcomes exclusively through the exposures being investigated. While this study accounted for the influence of known confounding SNPs, the possibility of unidentified confounding factors introducing genetic polymorphisms, which could skew the effect size estimation, remains. To validate the robustness and consistency of our findings, we implemented four supplementary methods: MR-Egger regression, the weighted median method (WME), and weighted mode.19–22 Concordance in the results obtained from these four MR models would strengthen the credibility of a causal relationship between childhood BMI and phlebitis and thrombophlebitis.
Heterogeneity test
In our study, we evaluated the heterogeneity among SNPs using Cochran’s Q-statistics, which are derived from the IVW estimate, along with the I2 statistic. The I2 statistic is a measure of the proportion of total variation in study estimates that is due to heterogeneity rather than chance. A lower I2 value, particularly when closer to zero, suggests that the observed heterogeneity is more likely attributable to sampling error. When the I2 value is <0.25, it indicates that the heterogeneity is minimal. This approach allows for a more nuanced understanding of the variability in the results attributed to differences between the SNPs that extend beyond what could be expected by chance alone.23,24
Pleiotropy test
In MR analysis, a crucial assumption is that the IVs influence the outcome exclusively through exposure. Therefore, it is vital to assess the potential genetic pleiotropy, which refers to a situation where a single genetic variant affects multiple traits, in the relationship between the exposure and outcome. MR-Egger regression analysis is employed to evaluate the bias introduced by genetic pleiotropy. The intercept of the MR-Egger regression serves as an indicator of the extent of pleiotropy. A smaller value of the intercept suggests a lower degree of genetic pleiotropy. In our study, we assessed the presence of genetic pleiotropy by examining the p value from the genetic pleiotropy test. A p value >0.05 is indicative of weak or no significant evidence of genetic pleiotropy affecting the causal analysis, implying that any such effects are likely negligible. Thus, the p value was used as a criterion to evaluate the impact of genetic pleiotropy in our causal analysis.
Sensitivity analysis
In our study, we conducted a leave-one-out sensitivity analysis alongside the IVW method to evaluate the impact of each individual SNP. This method checks if removing any single SNP significantly alters the combined effect value of the remaining SNPs. Consistency in results with and without each SNP indicates that no single SNP is unduly influencing the MR analysis.
Results
SNP selection and validation
In our study, SNPs linked to childhood BMI were identified from the Integrative Epidemiology Unit (IEU) Open GWAS database for childhood BMI. The screening criteria for these SNPs were a p value of <5e-08 and LD value of <0.001. Following these criteria, we successfully identified a total of 16 SNPs associated with childhood BMI. Importantly, the F-statistics for all these 16 SNPs were >10, indicating their robustness as IVs in our analysis.
MR assessment of the effect of childhood BMI on phlebitis and thrombophlebitis
The IVW method in our study provided evidence supporting a causal association between BMI and phlebitis and thrombophlebitis (beta = 0.002739, SE = 0.0007401, p = 0.0002147; Table 1, Fig. 2). The MR-Egger intercept, indicative of average pleiotropic effect, was −0.00018 (p = 0.405), suggesting that directional pleiotropy likely did not bias the results. However, the MR-Egger analysis itself showed no causal association (beta = 0.005276, SE = 0.003045, p = 0.1051; Table 1, Fig. 2). Similarly, the weighted mode analysis also indicated no causal relationship (beta = 0.002204, SE = 0.001852, p = 0.2525; Table 1

The scatterplot illustrates the distribution of individual effect size estimates, demonstrating the association between childhood BMI and phlebitis and thrombophlebitis. It includes scatterplots for four distinct TSMR methods, each depicting causality. BMI, body mass index.
Analysis Utilizing TSMR to Investigate the Link Between Childhood BMI and the Risk of Phlebitis and Thrombophlebitis
BMI, body mass index; CI, confidence interval; Nsnp, Number of single Nucleotide Polymorphism; TSMR, two-sample Mendelian randomization.
Assessment of MR assumptions
In our study, the robustness of the findings was evaluated using a leave-one-out sensitivity analysis. This analysis revealed that no individual SNPs exerted a significant impact on the overall effect of childhood BMI on phlebitis and thrombophlebitis, as illustrated in Figure 3. Furthermore, heterogeneity analysis across all four TSMR methods revealed no statistically significant heterogeneity (p > 0.05), enhancing the reliability of our MR estimates (Table 2).

Sensitivity analysis using the leave-one-out approach for the impact of childhood BMI on phlebitis and thrombophlebitis is shown. Each black dot represents the causal effect determined by the IVW method after excluding each specific SNP on the left. The red line illustrates the overall causal effect estimated through IVW, including all SNPs. IVW, inverse variance weighting; SNPs, single nucleotide polymorphisms.
Heterogeneity Statistics of TSMR
Additionally, the results of the pleiotropy test, as indicated by the MR-Egger regression intercept of −0.00018 (p = 0.405), suggested that horizontal pleiotropy did not significantly affect the causal analysis outcomes, as detailed in Table 3. Asymmetry in the funnel plot would typically indicate directional horizontal pleiotropy, potentially biasing MR results. However, in our study, both the funnel plot and the MR-Egger regression test showed no evidence of asymmetry, as depicted in Figure 4. These findings collectively underscore the strength and reliability of the causal associations identified in our MR analysis.
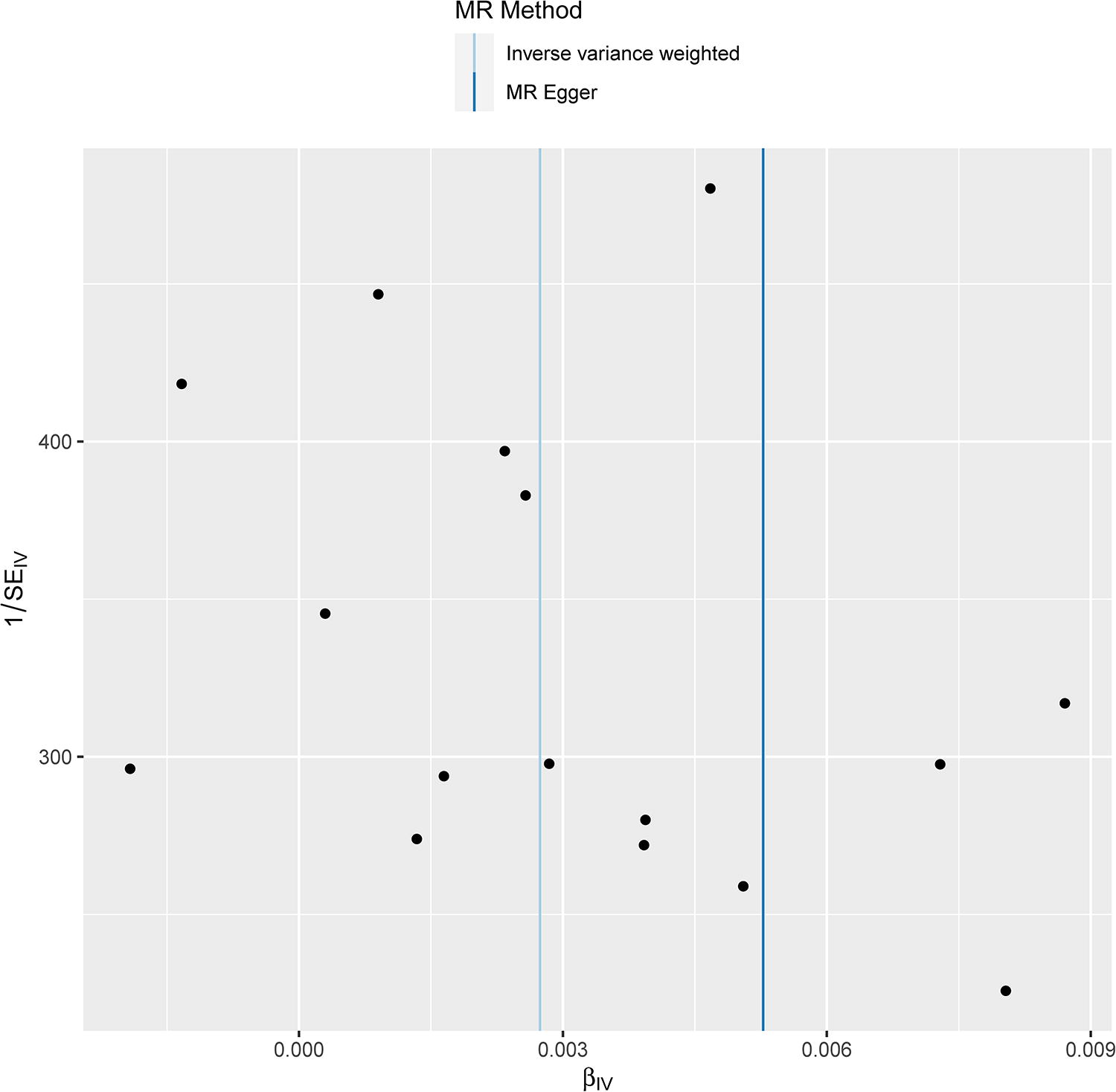
Funnel plot designed to evaluate heterogeneity. The blue line symbolizes the IVW estimate, while the dark blue line denotes the MR-Egger estimate.
Pleiotropy Statistics of TSMR
Discussion
Our study utilized MR to investigate the causal relationship between childhood BMI and the risk of phlebitis and thrombophlebitis. One of the key strengths of MR is its ability to minimize biases from unmeasured confounders and reverse causation, making it particularly valuable in epidemiological studies. By establishing a potential causal link, our findings highlight the importance of early prevention and management of childhood obesity to reduce the risk of venous disorders later in life. We utilized four different estimation methods for MR analyses: IVW method, weighted mode, WME, and MR-Egger regression. The findings demonstrated reliability and robustness in the sensitivity analyses conducted. While obesity has long been recognized as a risk factor for phlebitis and thrombophlebitis, the nature of its causal relationship with these conditions has remained unclear. Our study suggests that the associations between BMI and phlebitis and thrombophlebitis could be causal. Despite inconsistencies in the MR estimates obtained using IVW, weighted mode, MR-Egger, and weighted median analysis, both the IVW and weighted median analyses support a causal association between childhood BMI and phlebitis and thrombophlebitis. Given the greater precision retained in estimates by the weighted median estimator compared to the MR-Egger analysis, 26 our MR study points toward a potential causal role of childhood BMI in the risk of phlebitis and thrombophlebitis. Therefore, our research substantiates the association observed in previous observational studies, adding a new dimension to the understanding of the relationship between childhood obesity and these specific health outcomes.
Several traditional observational studies have examined the link between self-reported or measured BMI and the incidence of thrombotic disorders.27–31 A high BMI is acknowledged as a significant risk factor for various thrombotic conditions, including cardiovascular disease, stroke, and venous thromboembolism. Strong epidemiological data indicate that the relative risk of deep venous thrombosis in obese patients, as compared to nonobese individuals, is 2.50, with a 95% CI ranging from 2.49 to 2.51.31,32 This highlights the substantial impact of obesity on the risk of developing thrombotic disorders. 33
Studies have shown that chronic inflammation and impaired fibrinolysis, driven by obesity, are key mechanisms contributing to the increased risk of thrombosis in individuals with obesity. The pro-inflammatory and hypofibrinolytic states associated with obesity are likely exacerbated by the dysregulated expression and secretion of adipokines and microRNAs. These factors, which are significantly altered in obesity, further elevate the risk of thrombotic events. This connection underscores the complex interplay between obesity, inflammation, and thrombosis, highlighting the multifaceted impact of obesity on cardiovascular health.
Our study presents several notable strengths. To our knowledge, this is the first MR study that employs robustly associated SNPs to investigate the causal relationship between BMI in children and phlebitis and thrombophlebitis. This novel approach provides support for a causal link between a genetically predicted unit increase in childhood BMI and the development of phlebitis and thrombophlebitis, a relationship not previously reported. MR offers a significant advantage in minimizing the biases typically inherent in observational studies.34,35 We identified 16 SNPs from two distinct GWAS datasets and employed four different models (IVW, weighted mode, MR-Egger, and weighted median) to discern the causal relationship. This methodology enhances the validity of our findings. The sensitivity tests conducted in our study further validate the stability and accuracy of our causal findings. These tests reinforce the reliability of our results. The implications of our study are substantial. The evidence suggests that the genetic predisposition to childhood obesity is directly linked to an increased risk of phlebitis and thrombophlebitis. Our findings suggest that childhood obesity could have long-term health impacts, specifically increasing the risk of venous conditions like phlebitis and thrombophlebitis. Clinicians should consider the management of BMI in pediatric populations as a strategy not only for metabolic health but also for venous health. Early identification and management of high BMI in children could potentially reduce the burden of these conditions in adulthood.
Our study, while comprehensive, does encounter certain limitations. Our analysis was conducted using GWAS data from individuals of European ancestry. This demographic limitation restricts the generalizability of our findings to non-European populations, who may exhibit different genetic architectures and environmental exposures. Consequently, the causal relationship observed between childhood BMI and phlebitis and thrombophlebitis risk might differ in other ethnic groups. Future studies should aim to replicate these findings in diverse populations to confirm the generalizability and external validity of the results. The GWAS data used in this study did not include detailed childhood BMI characteristics, such as height, weight, and waist circumference. The absence of these specific components and the inability to categorize BMI into different obesity classes (e.g., mild, moderate, severe) limited our ability to perform stratified analyses that could provide deeper insights into the relationship between BMI and venous health. Additionally, childhood BMI can vary significantly during growth and development; therefore, using a single measure of BMI might not fully capture the complexity of the association between childhood obesity and later-life venous conditions. Future research should utilize datasets that incorporate more detailed phenotypic information to allow for a more comprehensive analysis of the impact of childhood obesity on venous health.
To further explore the association between childhood BMI and the risk of phlebitis and thrombophlebitis, future studies should focus on several key areas. First, conducting MR analyses in non-European populations would help determine if the observed causal relationship is consistent across different ethnic groups and genetic backgrounds. Second, incorporating longitudinal datasets with detailed phenotypic information, such as weight, height, and waist circumference, could provide a more comprehensive understanding of how various aspects of childhood obesity influence venous health over time. Additionally, exploring the underlying biological mechanisms, including inflammatory and coagulation pathways, could shed light on potential mediators and intervention targets. Last, evaluating the impact of early obesity management strategies through clinical trials could offer insights into effective prevention and treatment approaches for reducing the risk of venous disorders associated with elevated childhood BMI.
Conclusion
In conclusion, our MR analysis lends support to the hypothesis that BMI in children may have a causal association with an increased risk of phlebitis and thrombophlebitis. Our findings indicate that obesity could be a significant factor in the development of these conditions. These insights offer a valuable opportunity to explore and elucidate the underlying mechanisms through which obesity influences the risk of phlebitis and thrombophlebitis. To further our understanding, additional research is necessary to investigate the biological mechanisms that underpin this association. Such studies could not only deepen our knowledge of the pathophysiology of these conditions but also potentially lead to more targeted and effective prevention and treatment strategies for individuals at risk due to obesity, particularly from a young age.
Footnotes
Authors’ Contributions
Conception and design: T.Z. and L.L. Administrative support: F.J. and C.W. Collection and assembly of data: J.H. and Y.Y. Data analysis and interpretation: Y.B. Article writing: T.Z. Final approval of article: All authors.
Ethics Approval and Consent to Participate
As our study utilized publicly available summary data from existing GWAS, ethical approval was not required. The original GWAS had already obtained participant consent and provided de-identified data for research use.
Availability of Data and Materials
Data will be available on request to the corresponding author (Email:
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This work was supported by Dali Prefecture Science and Technology Plan Project (Grant No. 20232901A020010).