
Abstract
Background:
Lymphedema is an intractable disease requiring lifelong treatment. Daily self-care by the patient is essential; however, establishing care is often difficult. Our hospital offers a short-term educational hospitalization program that involves intensive, multidisciplinary intervention to develop self-care. This study aimed to evaluate the effectiveness of this program.
Methods and Results:
Among the patients diagnosed with primary or secondary lymphedema who underwent educational hospitalization, 31 cases (33 limbs) were included in this study. The upper extremity lymphedema (UEL) index and lower extremity lymphedema (LEL) index were used for objective evaluation, and the Lymphedema Quality of Life Questionnaire was used for subjective evaluation. The therapeutic effects of educational hospitalization were examined before admission, at discharge, and at 6 months postdischarge. The UEL/LEL index significantly decreased for both the upper and lower limbs after educational hospitalization. In addition, the UEL/LEL index change rate from prehospitalization to 6 months postdischarge was compared between the continued and discontinued exercise groups; the former index showed significantly more improvement than the latter. Comparing the quality of life (QOL) assessments pre- and posthospitalization, statistically significant improvements were observed in all categories, including function, appearance, symptoms, and psychological state.
Conclusions:
Short-term educational hospitalization led to a sustained reduction in the circumference of lymphedema-affected limbs and an improvement in the QOL. The multidisciplinary approach resulted in improved self-efficacy and established daily self-care.
Introduction
Primary or secondary lymphedema following malignant tumor treatment is an intractable disease characterized by fluid and protein accumulation in the interstitial spaces of the upper and lower limbs, causing physical distress, such as heaviness, mental stress, and cellulitis. No curative treatment has existed for lymphedema, and once it develops, complete recovery is impossible, and patients must live with the condition for the rest of their lives. Treatment for lymphedema is mainly conservative, aimed at maintaining the current condition, and complex decongestive therapy (CDT) combines compression therapy using elastic garments, exercise therapy under compression, manual lymphatic drainage, and skincare. 1 Daily self-care by the patient is essential to accomplish these CDTs. However, adherence is insufficient because learning the techniques is a burden and not easily established. 2 Studies on self-care adherence have reported attempts to improve adherence, such as self-recording. Still, the effects should be increased, with adherence level being low at around 40%–50%.3–5 It is difficult to increase patients’ motivation. To improve self-care adherence, patient education and comprehensive support should be provided through multidisciplinary collaboration and encourage patients’ self-efficacy. 6 Although several reports focused on factors affecting self-care adherence, only a few have tried to promote adherence. Our hospital provides a short-term lymphedema educational hospitalization program that involves intensive, multidisciplinary intervention for patients who have difficulty establishing self-care during outpatient visits, aiming to improve self-care and self-efficacy. In this study, objective and subjective evaluations were conducted before and after educational hospitalization to evaluate the effectiveness of this hospitalization.
Materials and Methods
Patients
The patients originally received compression therapy using their compression garments and simple lymphedema guidance, and educational hospitalization was performed for those who wanted to review their self-care or further enhance it. Among patients who underwent educational hospitalization treatment diagnosed with primary or secondary lymphedema between July 2021 and March 2024, those who were ≥20 years old and could be followed up for at least 6 months postdischarge were eligible in this study. The exclusion criteria are as follows: (1) patients with active cancer; (2) patients with edema other than lymphedema, such as lipedema, chronic venous insufficiency, heart or renal failure, and vein thrombosis; (3) patients with symptoms/signs of infection in the affected limb; (4) patients who are unable to perform accurate questionnaire evaluations due to mental illness; (5) patients with severe physical disabilities that interfere with daily life; and (6) patients who underwent lymphatic surgical treatment, such as lymphovenous anastomosis.
This study was approved by the Institutional Ethics Committee of the Kobe University Graduate School of Medicine (B230016-I), and all participants provided written informed consent and agreed to the scientific use of their data.
Intervention
Educational hospitalization was conducted for 4 or 9 days, depending on the patient’s request, and consisted of exercise therapy, nutritional guidance, compression garments, and skin care guidance. Patients brought their compression garments to the hospital. Before admission, the affected limb was measured, and the compression garment was ensured to have the appropriate compression pressure for the patient. During hospitalization, the patient underwent exercise therapy twice a day for 60 minutes each while wearing a compression garment according to the guidance of a physical therapist. The patients performed shoulder rotation and elevation exercises for the upper limbs and flexion/extension exercises for the elbows and wrist joints. For the lower limbs, the patients performed flexion/extension exercises for the hip and knee joints, as well as squat and calf raises. Aerobic exercises were performed using a treadmill or ergometer as appropriate. A nutritionist provided nutritional guidance and reviewed the patient’s diet to reduce fat, improve lymph flow, and eliminate swelling. Nurses are adequately guided in wearing compression garments, providing skin care, and living life postdischarge. In addition, we offered learning guidance by watching original videos to acquire basic knowledge about lymphedema. In all cases, thorough individual guidance was provided to the patients to ensure their understanding so they could continue the treatment at home after hospitalization.
Measurements
As an objective assessment of the treatment effect, we compared the upper extremity lymphedema (UEL) index or lower extremity lymphedema (LEL) index before admission to the hospital, at the time of discharge, and 6 months postdischarge.7,8 The UEL/LEL index is calculated by taking the sum of the squares of the affected limb circumference in five areas of the upper/lower extremity and dividing it by body mass index. Also, we calculated the UEL/LEL index change rate at discharge and 6 months postdischarge compared with the UEL/LEL index before admission. In addition, we compared the UEL/LEL index change rate before hospitalization and 6 months postdischarge between the group who continued the exercise taught during hospitalization at home and the group who did not.
As a subjective assessment, we compared the results of the Lymphedema Quality of Life Questionnaire (LYMQOL) questionnaire before admission and 6 months postdischarge. LYMQOL was proposed by Keeley et al. as a quality of life (QOL) evaluation method for lymphedema consisting of four domains, function, body image/appearance, symptoms, and mood, and has been translated and widely used in various countries. 9 The self-report questionnaires consist of 23 statements for the upper limbs and 22 for the lower limbs, and each item is answered on a four-grade Likert-like scale: “Not at all; A little; Quite a bit; A lot.” “Not at all” indicates a high QOL, and “a lot” indicates a low QOL. 10
Statistical analysis
Descriptive statistics was determined as means ± standard deviation for continuous variables, median (interquartile range 25%–75%) for discrete variables, and number (n) and percentage (%) for qualitative variables. Student’s t-test or Wilcoxon signed-rank test was used to analyze quantitative variables such as UEL/LEL index depending on the Gaussian distribution. Fisher’s exact test was used to analyze the qualitative variables of LYMQOL. p Values of <0.05 were used to denote statistical significance. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria, version 4.20). More precisely, it is a modified version of R Commander (version 4.20) designed to add statistical functions frequently used in biostatistics. 11
Results
A total of 33 limbs of 31 patients were included in the analysis. The demographic profiles and clinical characteristics of patients are shown in Table 1. The median age of the patients was 68 (60–74) years, and all were female. There were 15 upper and 18 lower limbs; two were primary, and 31 were secondary lymphedema. The median duration of lymphedema was 62 (44–91) months. Regarding the severity of lymphedema classified according to the stages of the International Society of Lymphedema, there were no cases of stage I, 11 limbs of stage IIA, 21 limbs of stage IIB, and one limb of stage III.
Patient Demographic Profiles and Clinical Characteristics
Continuous data are presented as means ± standard deviations or medians (interquartile ranges); categorical data are presented as absolute and relative frequencies, N (%).
ISL, International Society of Lymphedema.
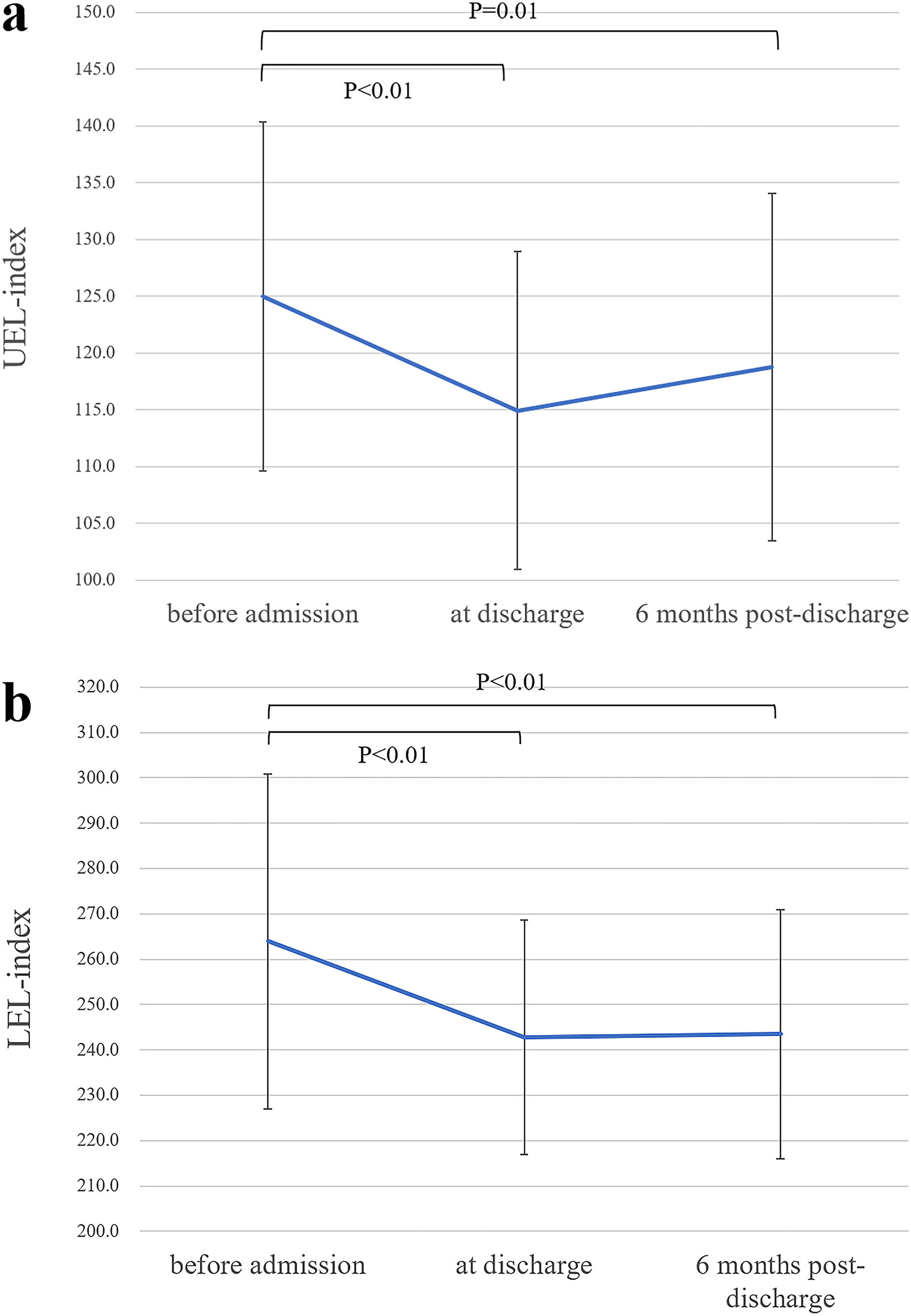
Figure 1 shows the changes in UEL/LEL index for the upper and lower limbs before admission, at discharge, and at 6 months postdischarge. The median upper limb UEL index was 127.0 (113.5–129.7) before admission, 112.0 (103.7–122.0) at discharge, and 116.3 (111.3–125.1) at 6 months postdischarge, and the median lower limb LEL index was 260.1 (241.6–284.1) before admission, 238.8 (224.4–261.4) at discharge, and 236.9 (226.9–253.4) at 6 months postdischarge. There was a significant decrease in the circumference of both the upper and lower limbs after the educational hospitalization, and the decreasing effect continued even 6 months postdischarge. Compared with the UEL/LEL index before admission, the change rate was significantly decreased at discharge and at 6 months postdischarge (Fig. 2).
Changes in
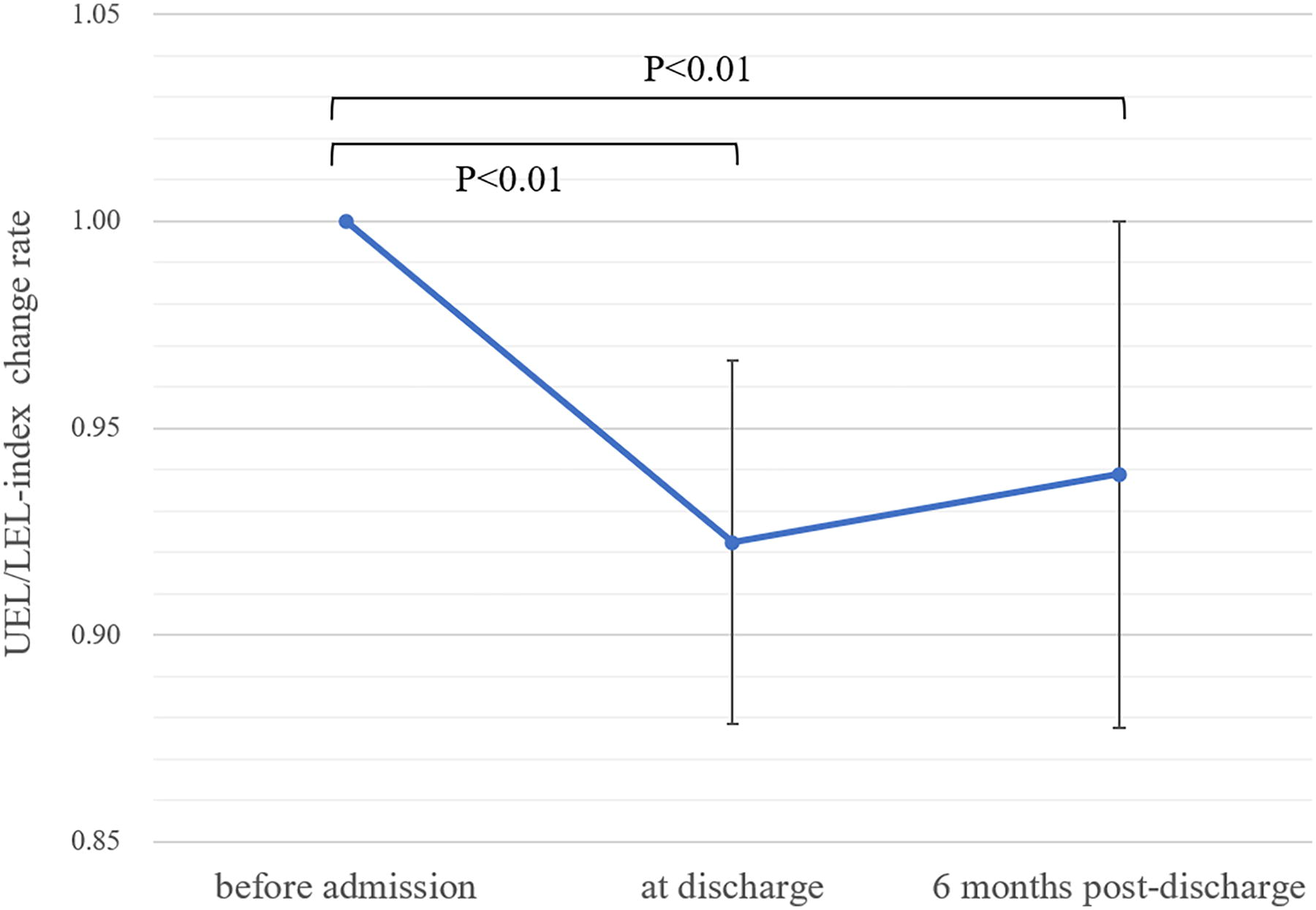
The UEL/LEL index change rate before admission, at discharge, and 6 months postdischarge. Compared with the index before admission, the index’s change rate significantly decreased at discharge and 6 months postdischarge.
At 6 months postdischarge, 20 patients (65%) continued to exercise as instructed during hospitalization at home, and 11 patients (35%) did not. Figure 3 shows the UEL/LEL index change rate from prehospitalization to 6 months postdischarge between the continued and discontinued exercise groups. In both groups, the UEL/LEL index decreased in most cases from prehospitalization to 6 months postdischarge. The average rate of change for the continued exercise group was −7.92 ± 5.74, while for the discontinued exercise group, it was −2.68 ± 5.40; the UEL/LEL index in the continuous exercise group showed a significant improvement compared with the discontinued exercise group.

The UEL/LEL index change rate from prehospitalization to 6 months postdischarge between the continued and discontinued exercise groups. The index in the continuous exercise group significantly improved compared with the discontinued exercise group.
Figure 4 compares LYMQOL, which summarizes the results of function, appearance, symptoms, and mood prehospitalization and 6 months postdischarge for all cases. Improvements in QOL were observed in all categories and were statistically significant. There were 132 LYMQOL responses for all patients of which 83 (63%) showed improvement before and after the educational hospitalization, 26 (20%) showed no change, and 23 (17%) showed worsening. Improvements in QOL were observed in many cases, with showing improvement of 1–2 scales within each item.
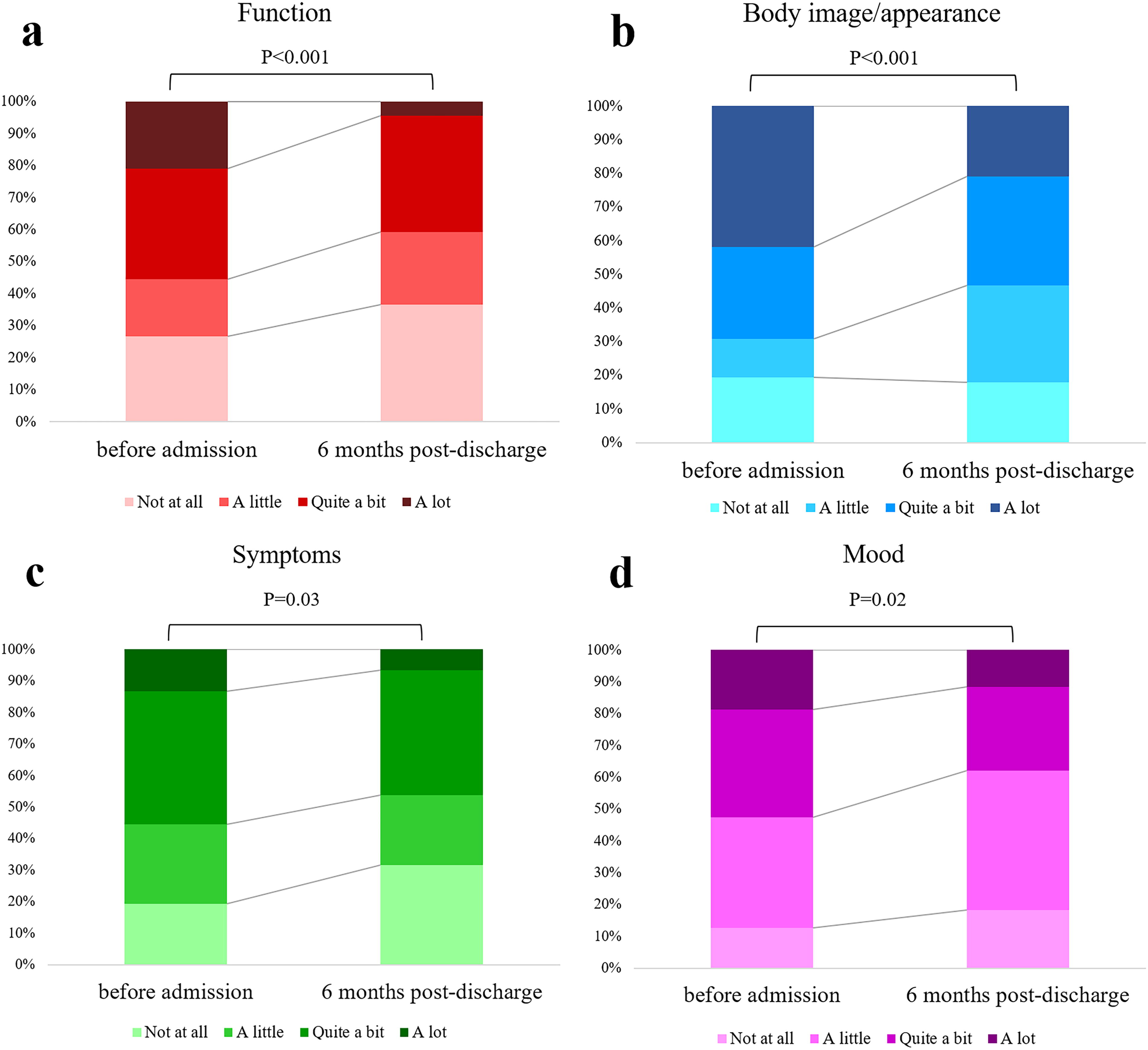
Comparison of LYMQOL that summarizes the results of
Discussion
Various treatments have been reported for treating lymphedema, and CDT is considered the most effective.12,13 CDT is useful because it improves patients’ function and QOL, and patients themselves actively carry out CDT, so daily self-care is essential. However, more than adherence to self-care is required due to the burden of learning complex procedures and the lack of time in daily life.2,14 Ridner et al. suggested that less than half of breast cancer survivors with lymphedema perform self-care as directed, and effective lymphedema self-care is necessary to achieve satisfactory health outcomes. 15 Greater self-care adherence was associated with lymphedema controllability, self-efficacy, perceived consequences, and more excellent knowledge; in particular, self-efficacy is said to have a highly positive effect on self-care.4,16,17 In our educational hospitalization, patients experienced an immediate reduction of limb circumference after exercise, giving them a sense of self-efficacy. In addition, a multidisciplinary approach was taken during hospitalization, and patients learned CDT from medical professionals, helping them solidify their knowledge. This was a reasonable approach to improving adherence to self-care.
There have been several reports of inpatient conservative treatment for lymphedema, but these have required relatively extended hospital stays. Previous reports have shown that a 3-week inpatient rehabilitation program improved vitality, mental health, emotional well-being, and interpersonal sensitivity and that an average of 17.0 days of conservative inpatient treatment positively affected the psychological status.18,19 These results indicate that lymphedema improved after a relatively long period of hospitalization and can be attributed to good adherence to the treatment. However, the medical burden associated with inpatient treatment for lymphedema has become a problem.20,21 The costs of conservative treatment are a concern, and lymphedema-related hospitalizations are a significant burden to the healthcare system, so long educational hospitalizations may be a waste of medical expenses.22,23 A short educational hospitalization, as in our treatment, can provide affordable and sufficient self-care skills; it can reduce the frequency of future cellulitis and decrease the frequency of outpatient and inpatient treatment, benefiting the health economy.
In recent years, advances in cancer treatment have improved prognosis, and the number of cancer survivors has increased, leading to a new era in which QOL after cancer treatment is increasingly important. Lymphedema is a significant disturbance to the QOL of cancer survivors, and if the care and control of edema are not effective, the patient’s QOL will be significantly impaired. When treating lymphedema, the patient’s condition should be appropriately evaluated, including their QOL. Patient-reported outcome measures are considered essential for evaluating the QOL of lymphedema, and LYMQOL, Lymphedema Quality of Life Inventory, and Lymphoedema Functioning, Disability and Health questionnaire have been reported.9,24,25 The LYMQOL was developed in the United Kingdom to evaluate the QOL of patients with lymphedema of both the upper and lower limbs. It is highly correlated with the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30, translated into other languages, and is used worldwide. 26 After educational hospitalization, even 6 months postdischarge, QOL often showed improvement in all four categories: function, body image/appearance, symptoms, and mood, with 63% of responses indicating at least one level of improvement in each item within each category. Hara et al. reported that conservative inpatient treatment for lymphedema helped elevate patients’ mood by the fifth day of hospitalization despite stressors such as environmental changes and the introduction of compression and exercise therapy. 19 This supports that short-term hospitalization positively affects the patients’ mental state rather than negatively. We believe that acquiring knowledge through educational hospitalization and the multidisciplinary approach led to a change in awareness of lymphedema care and a desire to engage in self-care, which positively affected the patient’s QOL.
When comparing the UEL/LEL index change rate before and 6 months after educational hospitalization, the continued exercise group showed significant improvement compared with the discontinued exercise group; 65% of the overall patients continued to exercise, which was disappointing. However, this study defined continued exercise as continuing what was instructed at our hospital. Because some patients did their strength training and went to the gym, the number of patients who continued to exercise is thought to be higher. Water percentages in the local tissue decrease immediately after compression bandage with exercise, so previous reports have shown that exercise effectively reduces limb and fluid volume.27,28 The evidence has been established regarding the effect of exercise, so patients should be diligent in engaging in exercise as part of self-care. For patients who cannot perform continuous exercise after educational hospitalization, ways to encourage them to continue exercising should be considered. This study relied on self-reported data on exercise adherence; thus, incorporating more objective measurement methods, such as activity tracking devices, in future studies may improve the accuracy of such assessments and lead to increased exercise adherence.
This study was conducted at a single institution with a sample size of 31 patients (33 limbs). Thus, multicenter studies or larger sample sizes would help increase the statistical power and generalizability of our findings. Moreover, extending the follow-up period to assess the sustainability of self-care practices and treatment effects would provide more comprehensive insights.
Conclusions
This study revealed that short-term educational hospitalization led to a sustained reduction in the circumference of lymphedema-affected limbs and improved QOL. Enhancing self-efficacy through a multidisciplinary approach during educational hospitalization led to the establishment of daily self-care, improving subjective and objective evaluations. Even short-term educational hospitalization can produce satisfactory results and will contribute to reducing medical costs and savings to the health care system. We want to conduct further follow-up research and examine the medium- to long-term effects.
Footnotes
Authors’ Contributions
Writing article and statistical analysis: D.A. Data collection and conceptualization: J.I. and M.O. Revision of the article: S.S.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.