
Abstract
Background:
Current understanding of changes in fluid distribution in response to the application of compression in primary lymphedema (PLE) is limited. This study measured fluid distribution before and after one application of standardized intermittent pneumatic compression (IPC) in the lower limbs of people with PLE, compared with those without lymphedema. High-frequency ultrasound (HFU) was used to measure dermal fluid, bioimpedance to measure segmental fluid, and percent water content (PWC) to measure fluid at specific anatomical points.
Methods and Results:
Fifteen people with PLE aged 11–40 years were matched for age, gender, and ethnicity to a person without lymphedema (NLE). PWC and HFU measures (low echogenic pixels) were taken bilaterally on the posterior leg and dorsum of the foot. Segmental bioimpedance (Extracellular Fluid/Intracellular Fluid, ECF/ICF) was measured in the foot, leg, and lower limb. Differences between groups, using the affected leg of unilateral and the more affected leg of bilateral PLE, were analyzed using the mixed ANOVA. There was significantly less ECF/ICF in the leg of NLE (p = 0.005) and PLE (p = 0.022) following IPC, and in the whole treated lower limb of NLE (p = 0.013), but no change in the treated limb of PLE. In contrast, the untreated limb showed significantly higher ECF/ICF in PLE (p = 0.040), a change not seen in NLE.
Conclusions:
The lack of response to compression in the foot, commonly affected in PLE, and the increase in fluid in the untreated PLE limb, indicates the need for further investigation of the effect of compression on fluid distribution in PLE.
Introduction
Genetic anomalies occur in primary lymphedema (PLE), impairing lymph drainage and resulting in fluid accumulation in the dermis and subcutaneous tissues.1,2 The long-standing fluid accumulation in lymphedema contributes to a stiffer dermis, 3 with associated inflammatory changes 4 and collagen deposition 5 in both the dermis and deeper tissues. These changes lead to challenges in treatment,6,7 especially with respect to application of compression, which is the mainstay of lymphedema management. Currently, the understanding of what changes in the dermis in response to application of compression in PLE remains extremely limited.
Fluid distribution in lymphedema and changes in fluid distribution in response to interventions have been assessed by fluid measures at a point, using percent water content (PWC) 8 measuring to the upper subcutis 9 and fluid measures in an overall limb segment (bioimpedance spectroscopy [BIS]). 10 High-frequency ultrasound (HFU) has been demonstrated to provide a method to measure dermal fluid in lymphedema. 11
The aim of this study was to compare fluid distribution before and after one application of standardized intermittent pneumatic compression (IPC) in the lower limbs of people with PLE, and those with no lymphedema. Both within-group and between-group changes were assessed using PWC, BIS, HFU, and circumferential measures.
Methods
Methodology for recruitment and measurement have been published elsewhere 11 but for the convenience of the reader, a summary is provided here. People with PLE aged 11–40 years were identified by staff from lymphedema services as either early or late onset PLE according to the St Georges algorithm 12 and invited to participate. People without lymphedema (NLE) were recruited by snowballing among friends and colleagues; their nonlymphedema status was confirmed using bioimpedance. All participants or their parent/guardian provided written informed consent for this study, with ethics approval from the Royal Children’s Hospital Melbourne (HREC/16/RCHM/136), Mercy Health (R16/67), and Mt Wilga Private Rehabilitation Hospital. Inclusion criteria for NLE were age within 12 months of their matched participant and of the same ethnicity and gender. Exclusion criteria for all participants included any inflammatory or infective skin conditions, pregnancy, uncontrolled cardiac or embolic conditions, connective tissue disorders, and active metastatic disease. Participants with a cardiac pacemaker were excluded from bioimpedance but included for other outcome measures.
Participants were asked to visit the bathroom on arrival, to establish baseline hydration status for bioimpedance measures, 13 before their height and weight were taken using a stadiometer and digital scales. Body Mass Index (BMI) was calculated by weight in kilograms divided by height in meters squared. During 20 minutes lying supine, both legs were marked for bioimpedance electrode placement at the boundaries of the foot and leg, measurement sites for PWC and HFU measures, and lower limb circumference (Table 1).
Measurement Sites
This table is reproduced with permission pending *******.
Least ankle and knee joint lines were boundaries for bioimpedance spectroscopy.
Measurement sites for PWC and HFU.
HFU, high-frequency ultrasound; PWC, percent water content.
All measures were taken on both limbs, the untreated limb providing a control for the effect of supine lying. Measures of PWC were taken using the MoistureMeterD Compact (Delfin Technology, Finland), on the foot in supine and the posterior calf in prone lying, with the leg supported on a pillow. In the same positions and at the same sites, the DermaScan C HFU (20 MHz; Cortex Technology) was used to measure low echogenic pixels (LEP). Reliability and methodology of image capture and LEP measures are fully described elsewhere, 14 but briefly a handheld transducer was held perpendicularly to the skin, with water-based gel between, and the same gain used for all image capture. From the image, LEP between 0 and 30 on a scale of 0–255, representative of fluid, 15 were measured in a standardized rectangular region of interest just below the epidermis (Fig. 1).
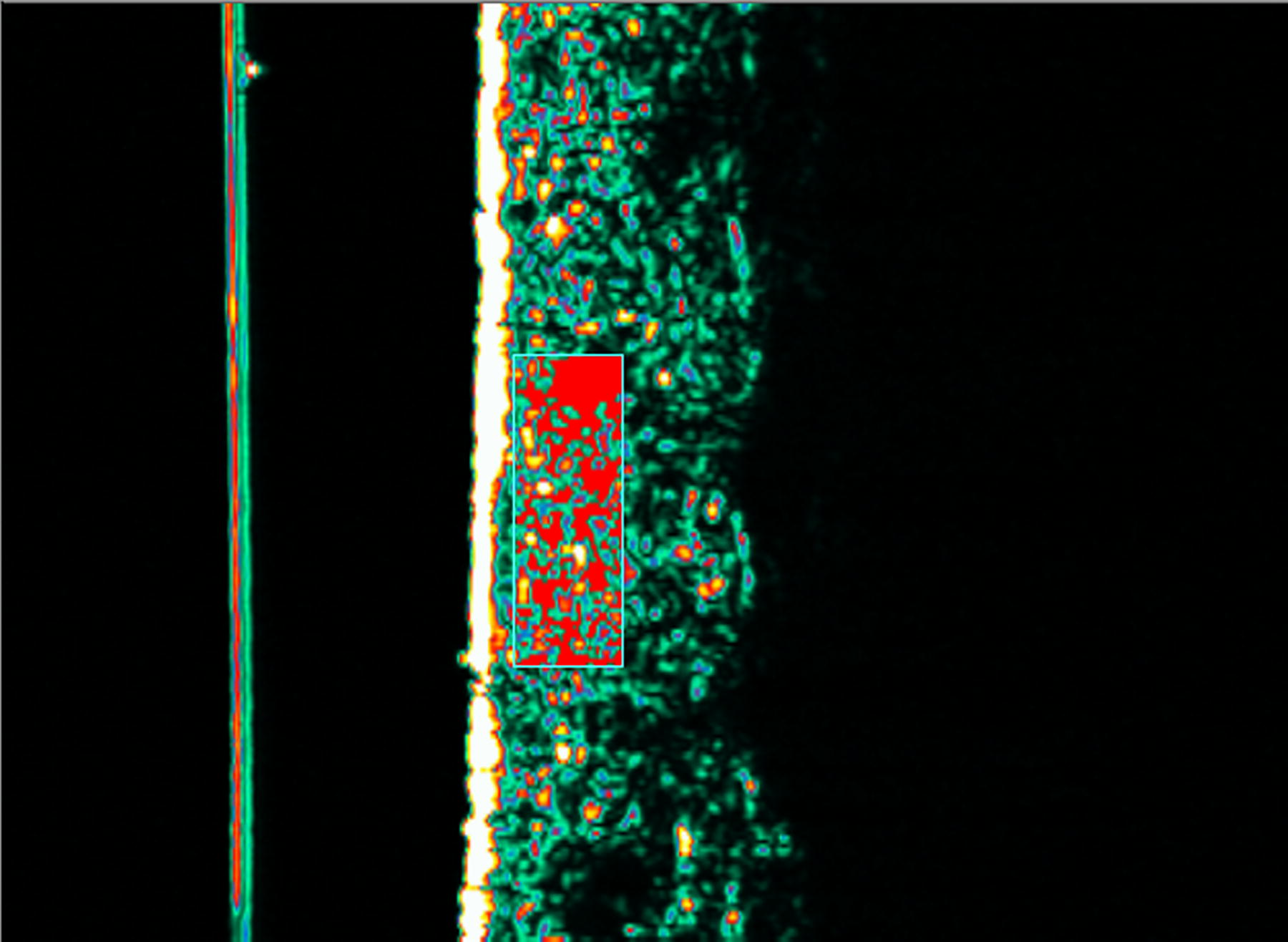
DermaScan C image. The rectangular region of interest (ROI) with range of pixel intensity from 0 to 30, representative of fluid, highlighted in red.
Extracellular Fluid/Intracellular Fluid (ECF/ICF) from segmental bioimpedance was measured using the SFB7 (Impedimed Ltd, Pinkenba, QLD, Australia) bilaterally, in supine with legs apart for the foot, the leg, and the whole lower limb. Electrode placement for foot and leg segments, based on anatomical landmarks,16,17 is provided in Figure 2; standard electrode placement was used for the full lower limb.13,18 Jewelry was removed and the skin wiped with alcohol prior to electrode placement.
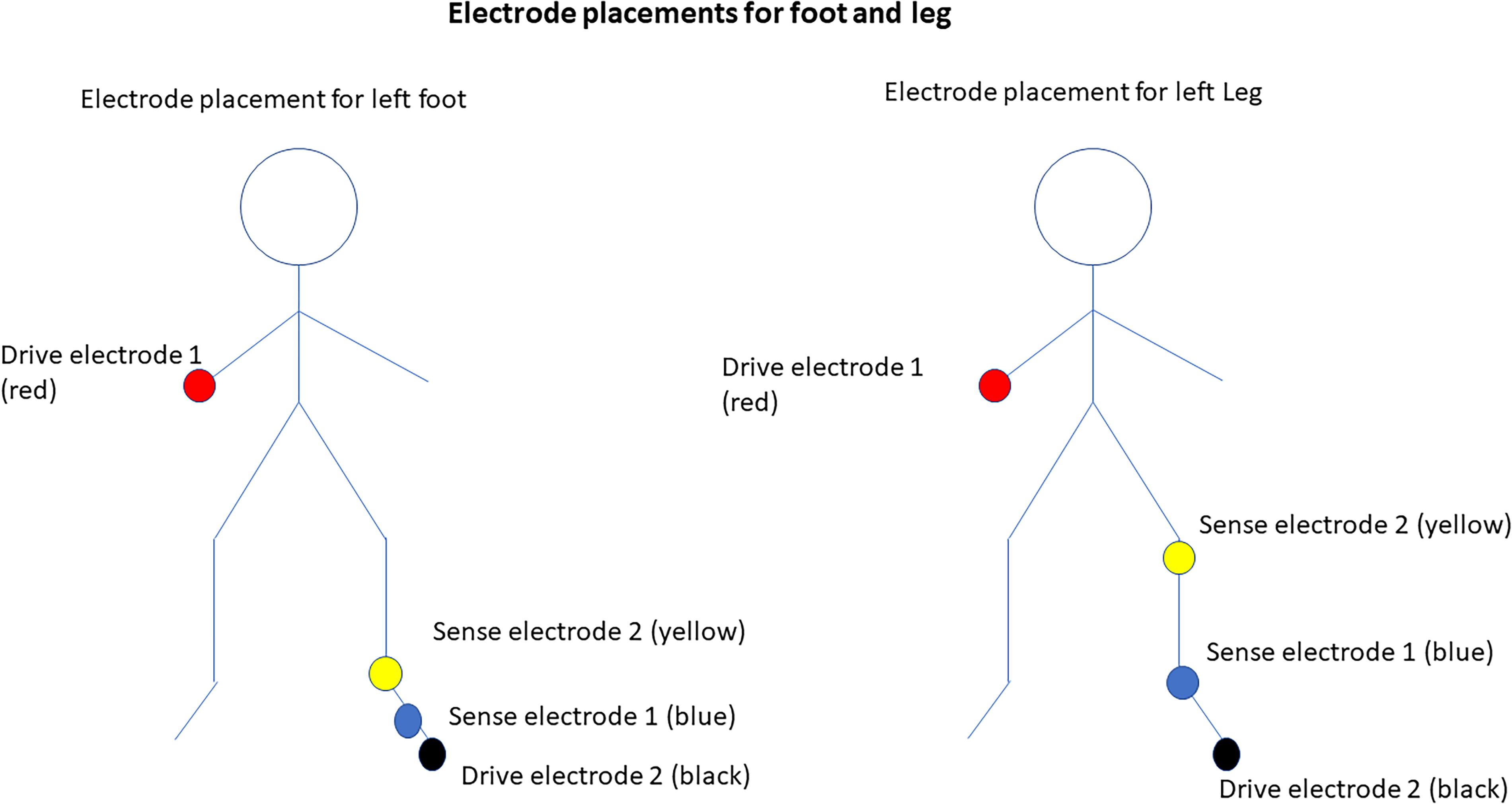
Bioimpedance electrode placement for foot and leg segments. Drive electrodes (black and red) were placed on the second toe and wrist joint, respectively. Sensor electrodes (blue and yellow) were placed (1) at the metatarsal head and ankle joint line, respectively, for foot segment measurement, and (2) at the ankle joint line and lateral knee joint line for leg segment measurements. ** reproduced with permission pending.
Following baseline measures, IPC was applied via an inflatable four-chamber leg sleeve, using the LX9 (Medi-Rent Pty Ltd, Matraville, NSW, Australia) for 50 minutes with 60 mmHg, dosage based on a systematic review of IPC dosage. 19 Compression was applied to the affected leg in unilateral PLE participants (uniPLE) and the more affected leg (determined by foot circumference at the measurement site) in bilateral PLE participants (biPLE). Measures of PWC, LEP, and ECF/ICF were repeated following compression.
Analysis
All analyses were carried out using SSPS v25 (IBM Corp, 2017). The mean of three measures were used for PWC and ECF/ICF and differences between pre- and postmeasures within and between NLE and PLE were investigated using the mixed ANOVA. Comparisons of LEP were made between NLE, uniPLE, and biPLE using the univariate ANOVA. The conservative Bonferroni correction was used and statistical significance denoted by p < 0.05. Clinical significance was addressed using the minimum detectable difference (MDD) calculated using the formula 1.96 × standard error of measurement (SEM) × √2, 20 where the SEM = SD√(1 − ICC). 20
Results
Analysis of baseline measures confirmed the presence or absence of lymphedema and hence the grouping of participants was correct. 11 Demographic data have previously been reported and are summarized here. 11 Fifteen PLE (2 male, aged 11 and 16 years; 13 females, aged 13–40), all Caucasian, were recruited. Eight (50%) had bilateral lymphedema (biPLE), and seven unilateral (uniPLE; four right, three left). The mean duration of lymphedema was 12 years, ranging 13 months–27 years. Four (27%) had onset at birth; most (11; 73%) were late onset, all diagnosed by lymphoscintigraphy, indocyanine green (ICG) lymphography, MRI, or ultrasound, except for one diagnosed at 9 years old and one aged 25 who declined lymphoscintigraphy but was diagnosed by a lymphedema physician. The majority were International Society of Lymphology (ISL) Stage IIA lymphedema, except one who, having a mild trace of papillomatosis on the toes, was ISL Stage IIB. The median BMI of PLE (24.3, Interquartile range IQR 6.5) was higher than that of NLE (22.5, IQR 4.7) but the difference was insignificant (p = 0.287), resulting in similarity between NLE and PLE in BMI, age, gender, and ethnicity.
As there was no difference between sides in the lower limbs of NLE, the limb corresponding to that of their matched pair was used for all comparisons. In LEP, there was a significant difference between uniPLE and biPLE at baseline, so subgroups of uniPLE and biPLE were compared with NLE. There was no difference between uniPLE and biPLE in PWC or ECF/ICF, so for these measures the whole group of PLE was compared with NLE.
Response to compression in NLE
There were significant decreases in ECF/ICF of the leg and whole limb, and in circumferences of the foot in the treated limb of NLE following compression (Table 2). Despite no significant change in ECF/ICF in the untreated limb after lying supine, there was, however, a significant decrease in leg circumference in the untreated limb as well, suggesting that positioning may have contributed to this change. Furthermore, the change in the treated foot did not exceed the SEM (0.1 cm for both foot and leg), so was unlikely to be clinically meaningful (Table 2). There were no significant changes in LEP or PWC.
Pre-IPC, Post-IPC, and Differences in All Measures in NLE
p value significant at < 0.05. 2. Two decimal places were given in the circumference of the foot, to make evident the differences. (Rounding obscured the difference in measures, tiny yet statistically significant on the treated side, and not significant on the untreated side).
IPC, intermittent pneumatic compression; LEP, low echogenic pixels; NLE, people without lymphedema.
Response to compression in PLE
Echogenicity: Response of biPLE and uniPLE to compression
Neither biPLE nor uniPLE showed any significant difference in LEP in either foot (p = 0.335; p = 0.422, respectively) or the posterior leg (p = 0.618; p = 0.553) in response to compression. Similarly, there was no change in LEP in the untreated leg or foot following the period of supine lying.
Circumference, PWC, and ECF/ICF: All PLE response to compression
There was a significant decrease in PWC, ECF/ICF, and circumference measures in the leg of PLE after application of IPC (Table 3).
Pre-IPC, Post-IPC, and Differences in ECF/ICF, PWC, and Circumference Following IPC in PLE
p value significant at < 0.05.
PLE, primary lymphedema.
The decrease in leg circumference in the treated limb of PLE (0.4 cm, p < 0.001) following IPC was clinically meaningful, being greater than the MDD (0.3; SEM 0.1 cm). However, the untreated leg of PLE also decreased in circumference by a mean of 0.6 cm, so the change on the treated limb cannot be attributed to IPC alone. As in NLE, supine positioning may have been a contributing factor.
There was a further overall effect on the untreated limb of PLE, as ECF/ICF significantly increased on this side following IPC. The clinical significance of the magnitude of this change in ECF/ICF is unclear, given the paucity of information regarding bioimpedance ratios in lower limb segments. It is unlikely such a small change has clinical significance but must be noted as an increase on this side that was not expected. The change in fluid distribution, however, was sufficient that there was no longer significantly higher ECF/ICF in the treated limb than the untreated limb, following compression (Table 4).
Between Sides Differences in ECF/ICF, PWC, IU, and Circumference in PLE: Pre- and Post-IPC
p value significant at < 0.05.
There was a significant decrease in PWC at the posterior leg of 2.3 (Table 3), which was not deemed clinically meaningful (MDD at the leg in PLE being 2.7).
The clinically significant reduction in PWC in the posterior leg, together with the significant reduction in the ECF/ICF in the same leg segment, suggests that there was a clinically meaningful change in point and overall segment fluid in response to IPC in the leg of PLE.
Differences between PLE and NLE in response to compression
There was no significant difference in any measure of PWC, ECF/ICF, or circumference at any site when the PLE and NLE groups were compared following compression, or in LEP when NLE was compared with uniPLE and biPLE (Table 5).
Treated Limb Response to Compression in ECF/ICF, PWC, and Circumferences PLE Compared with NLE
Indicates an increase in LEP postcompression.
Significant p value (< 0.05).
biPLE, bilateral PLE; uniPLE, unilateral PLE.
Discussion
This study provides evidence that measurable gross changes in fluid distribution (segmental bioimpedance and circumferential measures) in people with PLE are not related to changes in dermal fluid distribution. Broadly, the behavior of fluid distribution in the treated lower limbs of people with PLE and NLE appeared no different: both groups had gross changes (ECF/ICF) in fluid distribution in the treated leg and whole limb following compression, and no change in any measure in the treated foot. What is concerning is (1) the unexpected increase in ECF/ICF in the untreated limb of PLE and (2) the lack of response in any measure in the foot in PLE. This is a segment of high fluid accumulation in PLE,1,11,21 which appears not to respond to this mode or dose of compression.
While baseline increased dermal fluid was identified in the foot of both uniPLE and biPLE compared with NLE, 11 application of compression did not alter the amount of dermal fluid in either PLE or NLE either in the leg or the foot. However, gross changes (circumference and ECF/ICF) and point changes (PWC) at greater depth in the leg did occur. This challenges our understanding of the impact of compression and its mechanism for the management of LE and raises questions over how best to address increased fluid in the dermis in PLE.
The uncertain nature of drainage in PLE is illustrated by the increase in ECF/ICF in the untreated limb of PLE. Does compression of this type simply redistribute fluid across limbs rather than reintroducing it to the central drainage pathways, which is the theoretical underpinning for application of compression to one limb? This has implications for clinical practice.
Lack of change in the foot
Of further interest clinically, is the lack of change in fluid distribution (in all measures) of foot PLE after compression. Foot edema is a common problem and a difficult area to manage in PLE and this study indicates that compression applied in this manner makes no change to fluid distribution. This may be related to (1) the clinical changes in the condition itself, such as compromise in dermal lymph uptake, or drainage pathways from the foot; or (2) the method and type of compression application (pressure or cycle timing or sleeve construction) or a combination of the two.
As the foot is challenging to measure, 22 it is often not included in outcome measures 23 or combined with the whole limb in a volume measure. 24 Even compression garments are only tested for their effectiveness proximally from the ankle, 25 excluding the foot. Dermal fluid measures using HFU provides a method for future investigations of fluid distribution in the foot, along with segmental measures using bioimpedance.
Lack of response to compression in dermal fluid
Poor lymph uptake by initial lymphatics and incompetent lymphangions have been reported in some forms of PLE. 1 This immediately presents as a possible reason for the lack of dermal response to compression in PLE participants in this study; however, we were unable to determine the specific type of PLE in participants. Of great interest is the absence of fluid change in the dermis of NLE participants, which provides evidence that this lack of response is normal.
Dermal pressure variations, which are important to fluid uptake in the initial lymphatics,26,27 may have been absent in both groups during IPC in the supine position and contributed to the lack of response. Gaps in the initial lymphatics allow fluid uptake when open (when interstitial pressure is greater than pressure within the initial lymphatic)28–30 but are not evident when resting.30,31 Although IPC was intermittent, the sustained pressure of a long compression cycle in contrast to a short “off” cycle used in this study, may potentially not allow sufficient time for the dermal pressure variation required for lymph uptake, in support of previous studies. 32 Further studies examining response to different doses of compression are required.
The absence of movement, known to assist in reducing lymphedema, 33 may have contributed to the lack of change in dermal fluid. Skeletal muscle contraction and increased lymphangion contraction in the upright position34,35 both assist in increased lymph flow. As well, the lift-and-pull effect of movement on the skin creates fluctuating pressure 29 in the dermal interstitium, facilitating lymph uptake into the initial lymphatic vessels.26,27 It is important therefore not to extrapolate the findings from this application of compression to other applications of compression.
Response to compression in the leg
PLE had significantly more ECF/ICF and PWC in the leg segment than NLE at baseline, strong clinical indicators of edema, regardless of the lack of difference in circumference or LEP. Following compression, the lack of response in the dermis, along with significant reductions in both point (PWC) and segmental (ECF/ICF) measures in the leg segment of PLE, and ECF/ICF alone in NLE, appears to indicate the deeper overall effect of IPC on subcutaneous tissues, as previously suggested, 23 perhaps involving venous return.36–38
The lack of bioimpedance data in lower limb segments in the normal population limits the conclusions that may be drawn in this study. The percentage ECF/ICF reductions in legs of NLE (7%) and PLE (3%) appear small in contrast to the 44.9% variation in full limb bioimpedance (female Ri/R0 interleg ratios) found in the normal population over 18 months. 18 However, given the short time frame of this study (1–2 hours compared to 18 months), such small changes as 3% and 7% could be clinically meaningful.
The significant ECF/ICF reduction in the leg but not the full limb in PLE suggests fluid redistribution within the limb rather than reintroducing it to the central drainage pathways, consistent with a lymphoscintigraphic and ICG lymphography study of IPC in postinflammatory edema. 23 In contrast, NLE showed significant reductions in ECF/ICF in both the treated leg and full limb but not the untreated side, indicating a difference in the behavior of fluid distribution between NLE and PLE in response to compression.
A small percentage of lower limbs of PLE reportedly drain to the inguinal nodes on the contralateral side. 39 This is consistent with the increase in ECF/ICF following compression in the untreated limb of PLE in this study and suggests that fluid movement occurred from the treated to the untreated limb following compression. This fluid redistribution appears to have resulted also in a corresponding loss of significant difference in ECF/ICF between sides in PLE following compression. Previous studies have reported reductions in the contralateral untreated limb following IPC attributed to increased rate of lymphatic propulsion 40 as well as the effect of supine positioning. 41 Combining primary with secondary lymphedema in the same study may mask variations in drainage pathways in PLE. In the latter study, of mixed primary and secondary LE, there was an outlier with a large increased limb volume in the contralateral leg, suggesting the possibility of a primary LE with contralateral drainage. The results reported here raise questions over the suitability of applying compression to only one limb in PLE, even if swelling is not manifested in the contralateral side, unless ipsilateral pathways have been imaged and are known.
Further clinical implications come from considering the beneficial effect of elevation, which may have contributed to the small but significant circumferential reduction of both the treated and untreated leg of PLE, as seen in venous edema. 42 However, the reduction of circumference in the untreated leg was seen alongside an increase in ECF/ICF throughout that limb. This highlights the misleading information that comes from a nonspecific measure such as circumference to describe fluid fluctuations in a limb with PLE, as well as the importance of monitoring both lower limbs.
Limitations
This study was limited by its small sample size and a lack of genetic profiling with limited understanding of specific lymphatic anomalies in those with PLE. The results were specific to the pneumatic compression device, sleeve, and dosage used and may not be generalized to other types of compression. However, given the paucity of measurement reporting in the foot, it is fair to conclude that further investigation of response to compression in the foot in PLE is necessary.
Conclusions
Greater understanding of the effect of compression on fluid in PLE is required to ensure appropriate dosage and application. Further investigation of the efficacy of IPC compression sleeves in the foot is warranted. The lack of response to compression in the foot, commonly affected in PLE, indicates the need for further investigation for effective management of edema in PLE. Future studies investigating PLE, subgrouped according to genetic anomaly where the functionality of initial lymphatics is known, may provide more clinically relevant information about response to compression. Further study of a comparison of the response to compression in PLE, with lymphedema of different etiologies, may also add to dosage specificity in treatment.
Footnotes
Acknowledgements
Huge debt of gratitude for the generous time given by the participants with and without primary lymphedema, and their families, to be a part of this study. The authors also thank Professor Tony Penington for support at Murdoch Children’s Research Institute; for the mentorship of Professor Nicky Kilpatrick; Professor Karen Reynolds for support in the use of the DermaScan C ultrasound; Rotary Health for a PhD scholarship to study primary lymphedema; Haddenham Healthcare for provision of a MoistureMeterD Compact; and James Cook University for provision of the DermaScan C ultrasound.
Authors’ Contributions
J.J.P.: Conceptualization (support), methodology (equal), investigation (lead), formal analysis (lead), writing—original draft (lead), and writing—review and editing (equal). S.J.G.: Conceptualization (lead), methodology (equal), supervision, writing—original draft (support), and writing—review and editing (equal).
Author Disclosure Statement
J.J.P. is a private physiotherapist for people with primary lymphedema and a clinical advisor for Haddenham Healthcare who provided the MoistureMeterD Compact for this study. Haddenham Healthcare had no input to any part of this study. S.J.G. has no interests to disclose.
Funding Information
This study was completed with the support of the PhD research allowance from Flinders University and a PhD Scholarship from Rotary Health Australia.