
Abstract
Previously, we established a convenient enzyme-linked immunosorbent assay (ELISA) system targeting glucosyltransferase (GTF)-B derived from Streptococcus mutans for diagnosing caries risk. However, it has been reported that S. sobrinus possesses high cariogenicity and is more frequently detected in highly caries-susceptible patients than S. mutans is. S. sobrinus can secrete GTF-I, an important cariogenic factor for dental plaque formation, as well as S. mutans GTF-B. Therefore, in this study, we developed another feasible ELISA system targeting S. sobrinus GTF-I that would ensure caries risk determination by combined GTF-I and GTF-B levels. A readily measurable sandwich-ELISA system was devised, which consisted of monoclonal and polyclonal antibodies against GTF-I. The developed sandwich-ELISA system quantified the purified GTF-I with sensitivity and specificity, and a positive correlation was observed between the amount of GTF-I extracted from clinical plaque samples and S. sobrinus levels. Furthermore, high levels of GTF-I and GTF-B were detected using the sandwich-ELISA system in caries-susceptible subjects. These results indicate that the sandwich-ELISA system against GTF-I developed in this study is useful, and that the dual detection of the caries risk factors GTF-I and GTF-B is helpful for predicting caries risk.
Introduction
D
Dental caries remain an epidemic infectious disease, particularly among children, and some individuals may be susceptible throughout their lifetime.(4,5) Therefore, the prediction of caries risk is beneficial for the prevention of dental caries. It is well known that S. mutans is predominantly detected in the oral cavity of most people, and has a high cariogenic potential. Therefore, we previously established a readily measured sandwich enzyme-linked immunosorbent assay (ELISA) system that targeted GTF-B, which is the pathogenic factor of S. mutans.(6,7)
However, in some epidemiological studies, S. sobrinus is isolated more frequently from highly caries-susceptible patients than S. mutans is and it has greater cariogenic potential than S. mutans has.(8–10) S. sobrinus is usually detected in subjects also harboring S. mutans, whereas S. mutans is often found alone, even in caries-free subjects.(11,12) These findings suggest that the determination of a S. sobrinus pathogenic factor could be important for predicting the risk of caries, in addition to the estimation of S. mutans GTF-B. S. sobrinus can secrete GTF-I for the synthesis of WIG, as well as GTF-U, T, and S for WSG synthesis.(13,14) WIG synthesis is essential for the accumulation of bacteria on the tooth surface and induction of dental caries.(15,16) Therefore, quantification of GTF-I would contribute to evaluation of caries risk.
In this study, we attempted to develop a swift, convenient system for estimating caries risk using a sandwich-ELISA system against the GTF-I from S. sobrinus. We evaluated a sandwich-ELISA system for determining caries risk using a combination of GTF-I and GTF-B levels.
Materials and Methods
Bacterial strains and culture conditions
Streptococcus sobrinus 6715 and Streptococcus anginosus SS-03E(17) were used in this study and grown in Todd-Hewitt broth (THB; BD Difco, Franklin Lakes, NJ). Mitis Salivarius (MS; BD Difco) agar supplemented with 0.2 U/mL bacitracin and 15% sucrose (MSB) was used to grow the mutans streptococci. MSB agar containing 0.2 mg/mL aztreonam (MSBA) was used to grow S. sobrinus.(18)
Purification of recombinant glucosyltransferases
Extracellular recombinant GTF-I (rGTF-I) was purified from the culture supernatant of S. anginosus SS-03E as described previously.(17) In brief, cells were grown anaerobically for 18 h at 37°C in THB containing erythromycin (10 μg/mL), followed by centrifugation (10,000 g, 15 min). The supernatant was mixed with an equal volume of chilled ethanol and incubated at 4°C for 2 h. The precipitate was collected by centrifugation (20,000 g, 20 min) and dissolved in distilled water. Insoluble material was removed by centrifugation and the supernatant was used as the crude enzyme preparation. This preparation was supplemented with loading buffer (50 mM Tris-HCl [pH 6.8], containing 1% sodium dodecyl sulfate [SDS]), filtered (0.22 μm filter), and applied to a preparative polyacrylamide gel column, as described previously.(19) Eluted fractions were subjected to mini-slab SDS-polyacrylamide gel electrophoresis, and gels were either stained with Coomassie brilliant blue R-250 or subjected to Western blot analysis to confirm the presence of GTFs. The active fractions were pooled and mixed with chilled ethanol to remove the detergent. The precipitate was collected by centrifugation, dissolved in distilled water, and dialyzed against phosphate-buffered saline (PBS).
Subjects and collecting samples
Oral samples were collected from 28 healthy volunteers (age 20 to 27 years) with different S. sobrinus levels. This study protocol was approved by the Ethical Review Board of Nihon University School of Dentistry at Matsudo (EC02-015). Oral samples of brushing plaque were collected from each subject at 2 h after eating. After gargling once, plaque was taken by vigorous brushing for 1 min with a sterile toothbrush, collected in a sterile bottle after mouth rinsing for 30 s with 5 mL PBS, and used as brushing plaque samples. Samples were stocked in 10% skim milk or 50% dimethyl sulfoxide and maintained at −80°C until use.
Extraction of GTFs from oral samples
The brushing plaque samples (600 μL) were centrifuged (6000 g, 5 min) and 50 μL of 0.5 N NaOH were added to precipitate the samples. Samples were mixed for 1 min to extract, and 50 μL of 1 M MOPS were added for neutralization. Finally, 25 μL PBS were added and centrifuged (6000 g, 5 min). Supernatants were maintained on ice, precipitated again, and mixed with the first extraction to be used as GTF extractions.(6,7)
Microbiological analyses
Samples preserved at −80°C were immediately dissolved at 37°C, dispersed by sonication (50 W, 20 s), serially diluted, and inoculated on the MSB and MSBA agar plates using a spiral system (Model-D, Gunze Sangyo, Tokyo). After anaerobic incubation for 48 h, the number of mutans streptococci colonies on the MSB plates and the number of S. sobrinus colonies on the S. sobrinus selective MSBA plates(18) were counted using a microscope. The colony-forming units (CFU) per mL for each subject were calculated. The difference in colony numbers between MSB and MSBA represents the number of S. mutans colonies.(20)
Sandwich-ELISA
To quantify GTF-I in each sample, sandwich-ELISA was performed. Dr. K. Kobori (Sekisui Medical) kindly provided the anti-GTF-I monoclonal antibody (MAb) 5A and the anti-GTF-I polyclonal antibody used in this study. The wells in microtiter plates were coated with MAb 5A (10 μg/mL) (6,7) and incubated overnight. The plates were washed with PBS containing 0.05% Tween-20 and blocked for 1 h at room temperature with PBS containing 0.05% Tween-20, 1.0% bovine serum albumin, 10% sucrose, and 0.1% ProClin 300, a preservative containing the active ingredients 5-chloro-2-methyl-4-isothiazolin-3-one and 2-methyl-4-isothiazolin-3-one (Sigma-Aldrich, St. Louis, MO). After blocking, the plates were kept in a chamber (dry module, AS-ONE) for 2 days and stored at 4°C until use. Extracted GTF-I samples (50 μL) were added to each well and incubated for 2 h. After washing, the rabbit IgG anti-GTF-I polyclonal antibody was added and incubated for 1 h. After washing, plates were incubated with the goat anti-rabbit IgG horseradish peroxidase conjugate (Life Technologies, Tokyo, Japan) for 1 h at room temperature, followed by washes with PBS containing 0.05% Tween-20. Following the addition of the chromogenic substrate (1.5% citric acid monohydrate, 5.3% trisodium citrate dehydrate, 0.0015% thiourea, 0.2% 1.2-phenylenediamine dihydrochloride, and 0.02% hydrogen peroxide in distilled water), plates were incubated for 15 min at room temperature. The optical density (OD) at 492 nm was measured using a microplate reader (model MTP-32, Corona Electric, Hitachinaka, Japan), and the amount of GTF-I was calculated. The amount of GTF-B was measured as described previously.(7)
Results
Standardization of GTF-I ELISA
Purified rGTF-I was used to calibrate the developed sandwich-ELISA system. The calibration curve was constructed from a set of six rGTF-I concentrations and the OD values were measured using this ELISA. A correlation was observed between the amount of rGTF-I and the OD value obtained from the ELISA from 0 to 50 ng/mL protein. To avoid overestimation of GTF-I due to reaching a plateau, an optical density less than 0.8 was employed in the ELISA (Fig. 1).
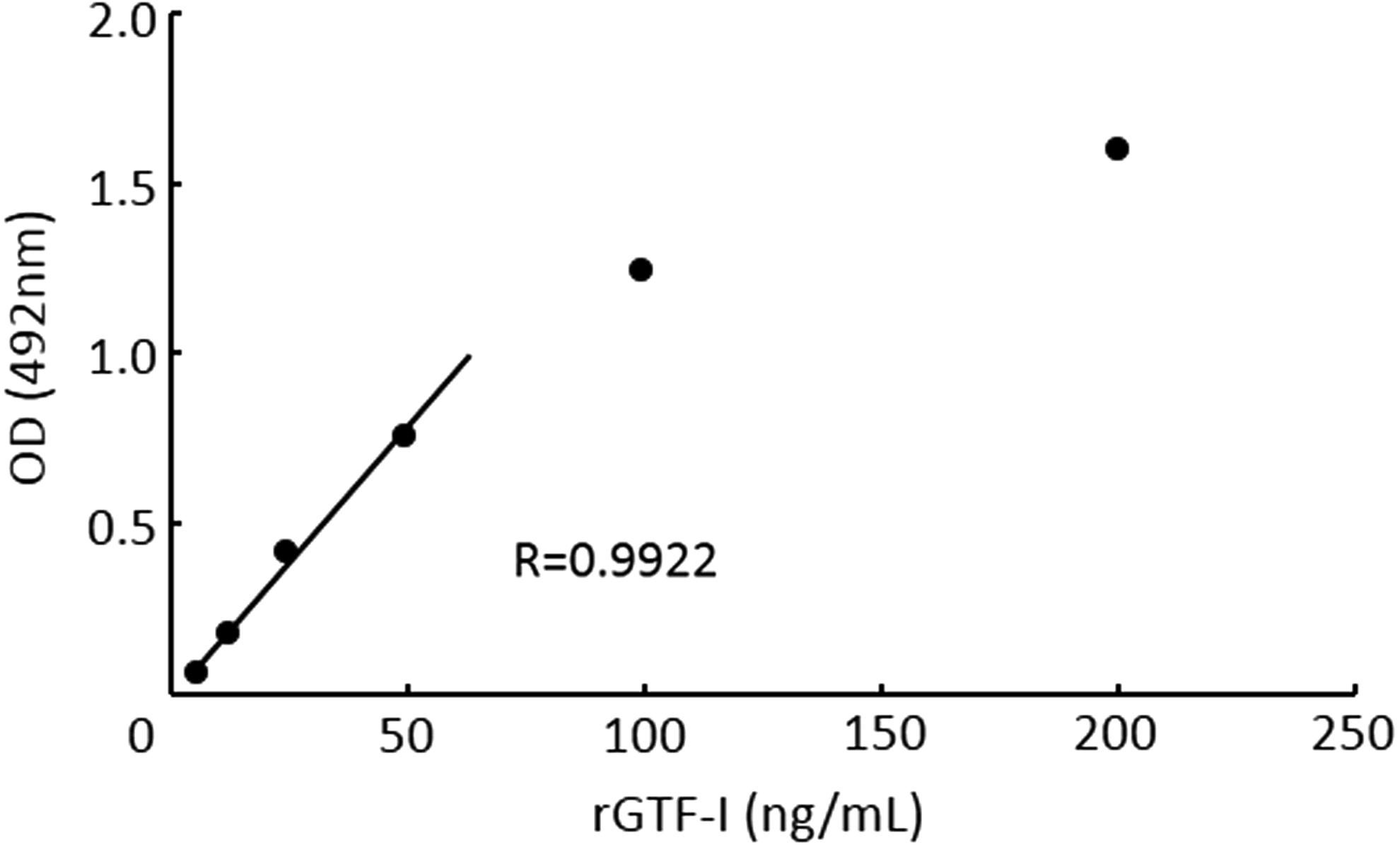
Calibration curve for purified rGTF-I. The mean of triplicate samples for each concentration is shown.
Evaluation of sandwich-ELISA system
The developed ELISA was used to assess the GTF-I level in frozen stocks of S. sobrinus 6715 cells. A positive correlation was observed between OD values and the number of S. sobrinus cells (Fig. 2). These results indicate that storage of bacteria at −80°C did not degrade GTF-I.
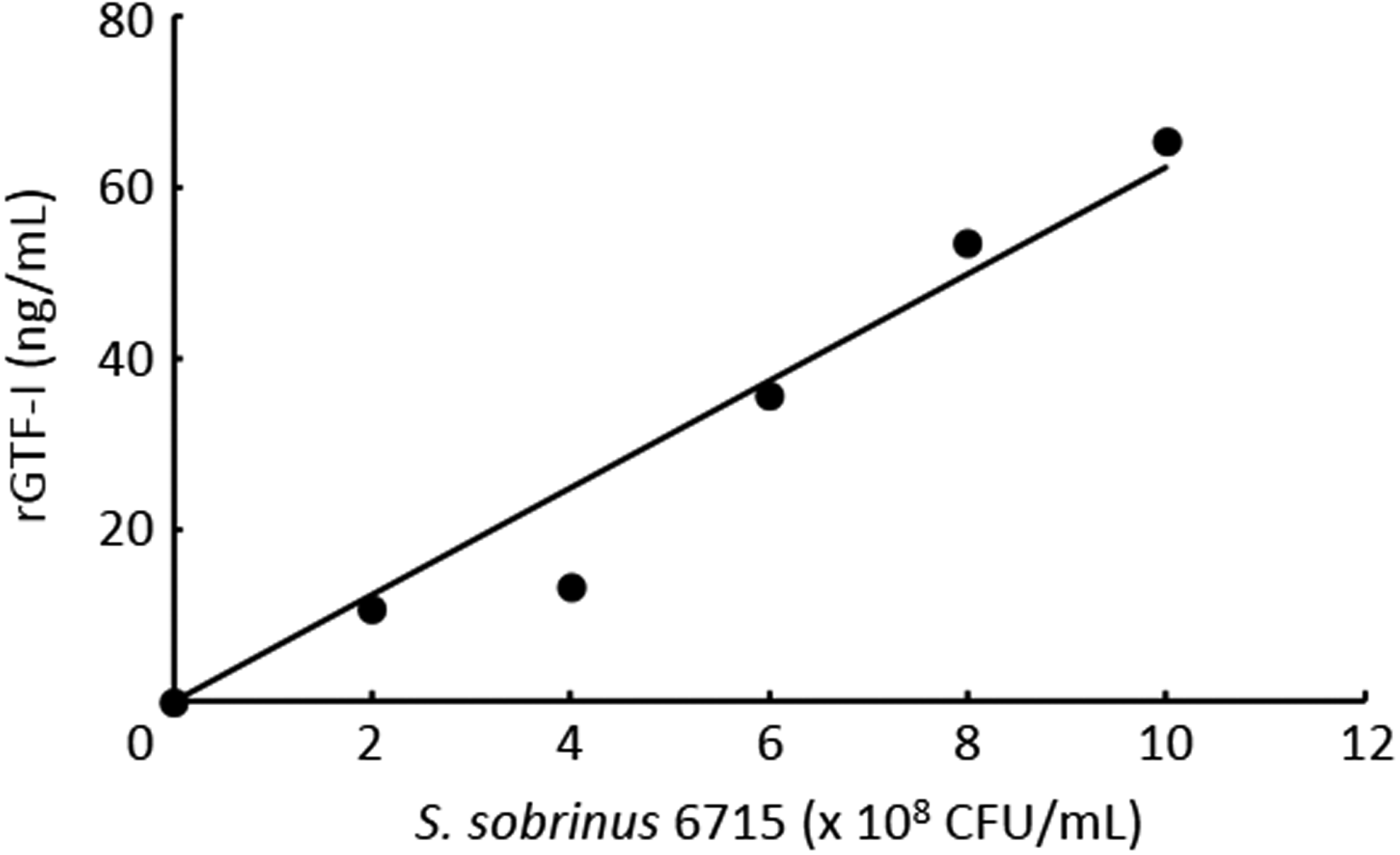
Estimation of GTF-I levels extracted from frozen S. sobrinus 6715. S. sobrinus was cultured in THB broth, washed with PBS, and stocked in PBS at −80°C. GTF-I was extracted from these bacteria using 0.5 N NaOH for 1 min and GTF-I was quantified by sandwich-ELISA.
Application of sandwich-ELISA system to clinical plaque samples
We next analyzed the relationship between S. sobrinus quantity and the amount of GTF-I in each clinical oral sample. From 28 healthy subjects, brushing plaque samples were collected, and S. sobrinus levels in each sample were calculated using MSBA plates. Simultaneously, the amount of GTF-I in each sample was assessed using the sandwich-ELISA method. The quantities of GTF-I and S. sobrinus levels in brushing plaque samples were positively correlated, with a correlation coefficient of 0.896 (Fig. 3). Our data indicate that the quantitative determination of GTF-I by sandwich ELISA in oral samples is useful for the evaluation of caries risk.

Correlation between the GTF-I level and S. sobrinus quantity in brushing plaque samples. Oral samples were collected and GTF-I was quantified using the sandwich-ELISA method.
Application of combining GTF-I and GTF-B levels to caries risk diagnosis
Finally, we confirmed the relationship between GTF-I and GTF-B levels detected using sandwich-ELISA and the caries prevalence of an individual. Three caries prevalence groups were created depending on the decayed, missing, and filled teeth (DMFT) scores of the subjects: caries-susceptible (DMFT>12), intermediate-level caries, and caries-free (DMFT=0). Table 1 shows the CFU of S. mutans and S. sobrinus, and the detection levels of GTF-B and GTF-I in the brushing plaque samples from subjects A–I. In all three subjects from the caries-susceptible group (A–C), both GTF-B and GTF-I were detected at high levels, which were correlated with the S. mutans and S. sobrinus levels. By contrast, all three subjects from the caries-free group (G–I) showed no GTF-B or GTF-I and no mutans streptococci in the order of 105 CFU. These results indicate that determination of GTF-I and GTF-B in oral samples enables determination of caries risk.
Susceptible, DMFT >12; free, DMFT=0.
Discussion
The diagnosis of caries risk is meaningful in preventive dentistry because dental caries is one of the most common and preventable diseases, particularly in childhood. In addition, humans are likely to get dental caries throughout their lifetime.(4,5) There are several diagnostic approaches to estimating caries risk, including streptococcus cultivation methods, semiquantitative immunoassay methods for S. mutans in saliva,(21,22) and quantitative real-time PCR methods.(23,24) However, cariogenicity and genetic diversity may not be identical among bacterial isolates.(8,25–28) Furthermore, it is not clear whether the levels of mRNA expression and protein translation are correlated.(29) Therefore, we targeted the GTF protein existing actually in the oral samples. We previously established a feasible, convenient sandwich-ELISA system targeting GTF-B produced from S. mutans in oral samples.(6,7) GTF-B is considered an important virulence factor due to its high sticky WIG synthesis activity.(30) This developed system is highly sensitive and specific for quantifying the amount of GTF-B. A strong correlation was observed between the amount of GTF-B and the DMFT score, as well as between S. mutans quantity and the DMFT score in clinical oral samples.(6,7) However, it has been reported that S. sobrinus is isolated more frequently from highly caries-susceptible patients than is S. mutans, and the cariogenic potential of S. sobrinus is greater than that of S. mutans.(8–10) Furthermore, S. sobrinus is usually detected in subjects also harboring S. mutans, whereas S. mutans is often found alone, even in caries-free subjects.(11,12) Therefore, in the present study, to improve the diagnostic result, we targeted GTF-I produced from S. sobrinus and developed a convenient sandwich-ELISA system against GTF-I. In this regard, our results showed that the GTF-I level was higher in caries-susceptible subjects who also had high levels of GTF-B. These results suggest that the GTF-I level is an indicator of caries risk.
MAb 5A showed high sensitivity and specificity against GTF-I, but did not react with GTF-U, T, and S from S. sobrinus, as indicated by Western blotting (data not shown). When the specificity of the ELISA system was examined using filtered saliva, including appropriate amounts of S. sobrinus as samples, it was not affected by other components of saliva. In addition, when other oral streptococci, such as S. mitis, S. salivarius, S. oralis, S. gordonii, S. anginosus, and S. sanguinus were subjected to ELISA, only S. sobrinus was recognized (data not shown).
Furthermore, a positive correlation was observed between the amount of GTF-I and the S. sobrinus quantity in brushing plaque samples from individuals with exceptions (Fig. 3). These data suggest that the GTF-I-producing ability may differ among the S. sobrinus strains harbored by each subject. Similar properties were observed for GTF-B detection by the sandwich-ELISA system developed previously by our group.(6,7) Our preliminary tests showed that GTF-I was likely unstable in alkaline solution (data not shown), perhaps resulting in reduced detection of GTF-I compared to GTF-B. Although the GTF-I detection limit was lower than that of GTF-B, the value of GTF-I detected was discriminative. Furthermore, the detection results of GTF-I and GTF-B quantified using our sandwich-ELISA system were reflected in the caries prevalence (Table 1), indicating that determination of GTF-I supports the diagnostic result of GTF-B. Combined, these results indicate that although some exceptions occur, the swift sandwich-ELISA system targeting GTF-I developed in this study is satisfactorily sensitive and positively correlates with both the GTF-I level and S. sobrinus quantity. Furthermore, high levels of GTF-I and GTF-B were detected in caries-susceptible patients using this sandwich-ELISA system. These results suggest that dual estimation of the two caries risk factors, GTF-I and GTF-B, in an individual ensure caries risk diagnosis and would contribute to the prevention of dental caries.
Footnotes
Acknowledgments
We would like to thank Professors K. Fukushima and M. Hayakawa for guidance and advice. This work was supported by a Grant-in Aid for Scientific Research (24592845) from the Japan Society for the Promotion of Science and the Tsuchiya Culture Promotion Foundation.
Author Disclosure Statement
The authors have no financial interests to disclose.