
Abstract

Introduction
A
Neurological Complications of Varicella Zoster Virus Reactivation
VZV is a neurotropic alphaherpesvirus. Primary infection usually produces varicella (chickenpox), after which virus becomes latent in ganglionic neurons along the entire neuraxis. As cell-mediated immunity to VZV declines with advancing age or immunosuppression, virus reactivates to produce zoster (shingles). Zoster may be further complicated by myelitis, meningoencephalitis, or vasculopathy. VZV vasculopathy is due to productive virus infection in cerebral arteries and is a well-documented treatable cause of stroke. The diverse manifestations, laboratory features, pathogenesis, and treatment of VZV vasculopathy have been updated recently.(1)
Cases of VZV infection of the Temporal Artery
Most VZV vasculopathy involves intracranial arteries. However in the past 2 years, we showed that VZV also infects the extracranial temporal artery, producing symptoms, signs, and laboratory abnormalities seen in GCA. Case #1 was an elderly man who developed ophthalmic-distribution zoster followed one month later by multifocal VZV vasculopathy that manifested as ischemic optic neuropathy (ION), as well as clinical features of GCA.(2) Importantly, the presence of both anti-VZV IgG and anti-VZV IgM antibodies in CSF indicated chronic active infection. Furthermore, although visual loss began weeks before the presence of anti-VZV antibody in CSF was revealed, our patient's vision improved from finger-counting to 20/50 after 2 weeks of intravenous antiviral treatment. Finally, detection of VZV antigen verified the diagnosis of VZV infection in the temporal artery (Fig. 1). This was important because VZV vasculopathy has been successfully treated even after 6 months of disease.(3)
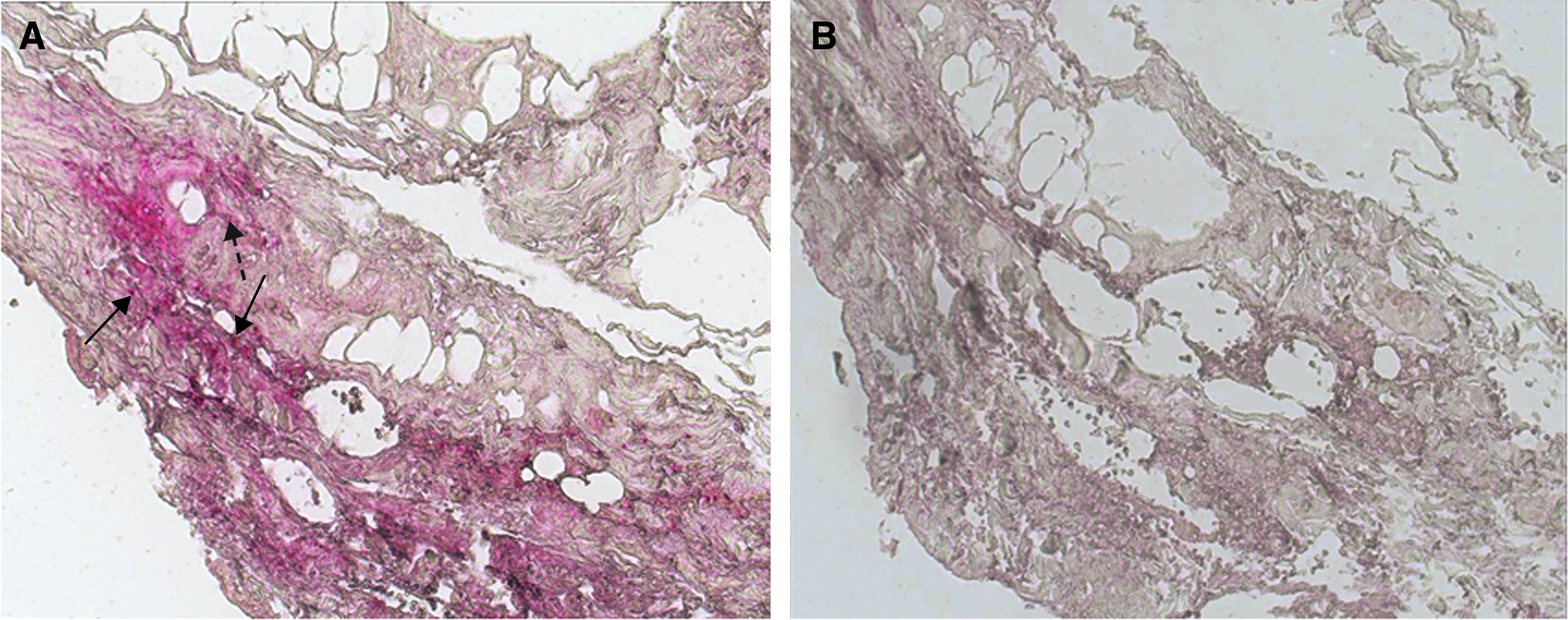
Immunohistochemical analysis of the ipsilateral temporal artery of a patient with ischemic optic neuropathy one month after herpes zoster. Sections of the temporal artery were deparaffinized and incubated with 10% normal sheep serum (NSS) in phosphate-buffered saline (PBS) for 1 h at room temperature. To prevent non-specific binding, primary antibodies were adsorbed with normal human liver powder for 30 min and again for 20 h at 4°C. Sections were then incubated with polyclonal antibodies raised against VZV ORF 63 protein (1:1000 dilution) or normal rabbit serum (1:1000 dilution), rinsed with PBS and incubated with a 1:300 dilution of biotinylated goat anti-rabbit IgG in PBS containing 5% NSS, washed three times in PBS, incubated with alkaline phosphatase-conjugated streptavidin (1:100 dilution), and washed three times with PBS again. The color reaction was developed for 5–30 min with fresh fuchsin substrate system. Levimasole was added to the color reaction to block endogenous phosphatase. Uninfected and VZV-infected BSC-1 cells were used as controls (not shown). Note VZV antigen (red) in the nucleus and cytoplasm (solid arrows) and cytoplasm alone (dotted arrow) of cells in the arterial adventitia (
Further analysis of Case #1 revealed a number of remarkable features. First was the development of VZV vasculopathy in an extracranial artery. There are only two other reports of VZV vasculopathy affecting arteries that are not intracranial: one of a patient with spinal cord infarction due to VZV vasculopathy (4) and another case of varicella in an adult who developed stroke and peripheral arterial thrombosis.(5) Second, the serendipitous biopsy of the temporal artery before any clinical symptoms or signs developed corresponding to the temporal artery revealed that viral antigen was most abundant in the arterial adventitia, with lesser amounts in the media. In contrast, viral antigen was seen exclusively in the thickened intimal layer in fatal cases of VZV vasculopathy that progressed for 10 to 12 months before death.(6) It appears that early in the course of productive arterial infection, as seen in our patient, virus establishes infection initially in the adventitia, presumably after transaxonal spread via ganglionic afferent fibers. Thereafter, transmural migration occurs, with productive infection continuing in the arterial media and intima.
Case #2 was an elderly woman who developed an ION with no other features of GCA and in whom VZV was demonstrated in the ipsilateral temporal artery; importantly, she had no history of recent zoster.(7) Virological verification was provided by detection of VZV antigen in the adventitia of the clinically asymptomatic and pathologically GCA-negative temporal artery ipsilateral to vision loss (Fig. 2) and of anti-VZV IgG antibody in CSF with reduced serum/CSF ratios indicative of intrathecal synthesis of anti-VZV IgG antibody. This case: (1) expanded the spectrum of disease produced by VZV without rash to ION, (2) revealed that ipsilateral GCA-negative temporal artery VZV infection was useful in diagnosis, and (3) confirmed early VZV infection of adventitia in VZV vasculopathy, providing additional evidence that extracranial arteries become infected transaxonally after VZV reactivates from ganglia.
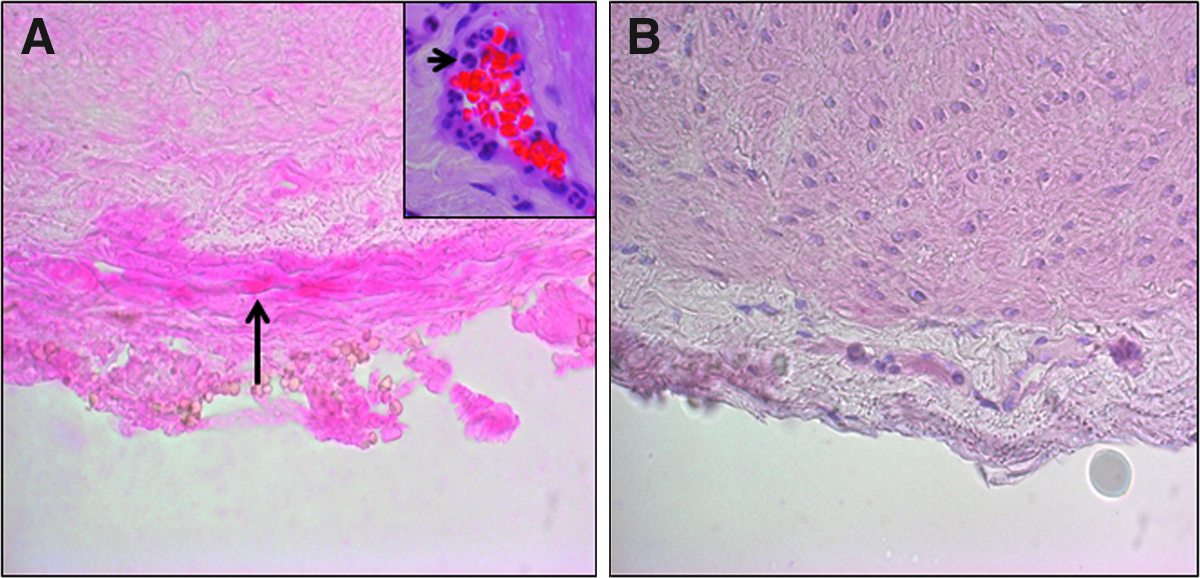
Immunohistochemical analysis of the ipsilateral temporal artery of a patient with ischemic optic neuropathy and no history of zoster rash. Sections of the temporal artery were prepared and immunostained as described in Figure 1. Note the presence of VZV antigen in the adventitia of the temporal artery stained with anti-VZV antibody (
Case #3 was a 54-year-old diabetic, also with no history of recent zoster, who developed an ION followed by acute retinal necrosis and temporal artery infection, again in the absence of zoster rash.(8) The vitreous fluid contained amplifiable VZV DNA but not HSV-1, CMV, or toxoplasma DNA. The clinical presentation was remarkable for jaw claudication and intermittent scalp pain, prompting a temporal artery biopsy that was pathologically negative for GCA, but notable for VZV antigen (Fig. 3). The case added to the clinical spectrum of multifocal VZV vasculopathy. The development of acute VZV retinal necrosis after ION supports the notion that vasculitis is an important additional mechanism in the development of VZV retinal injury.
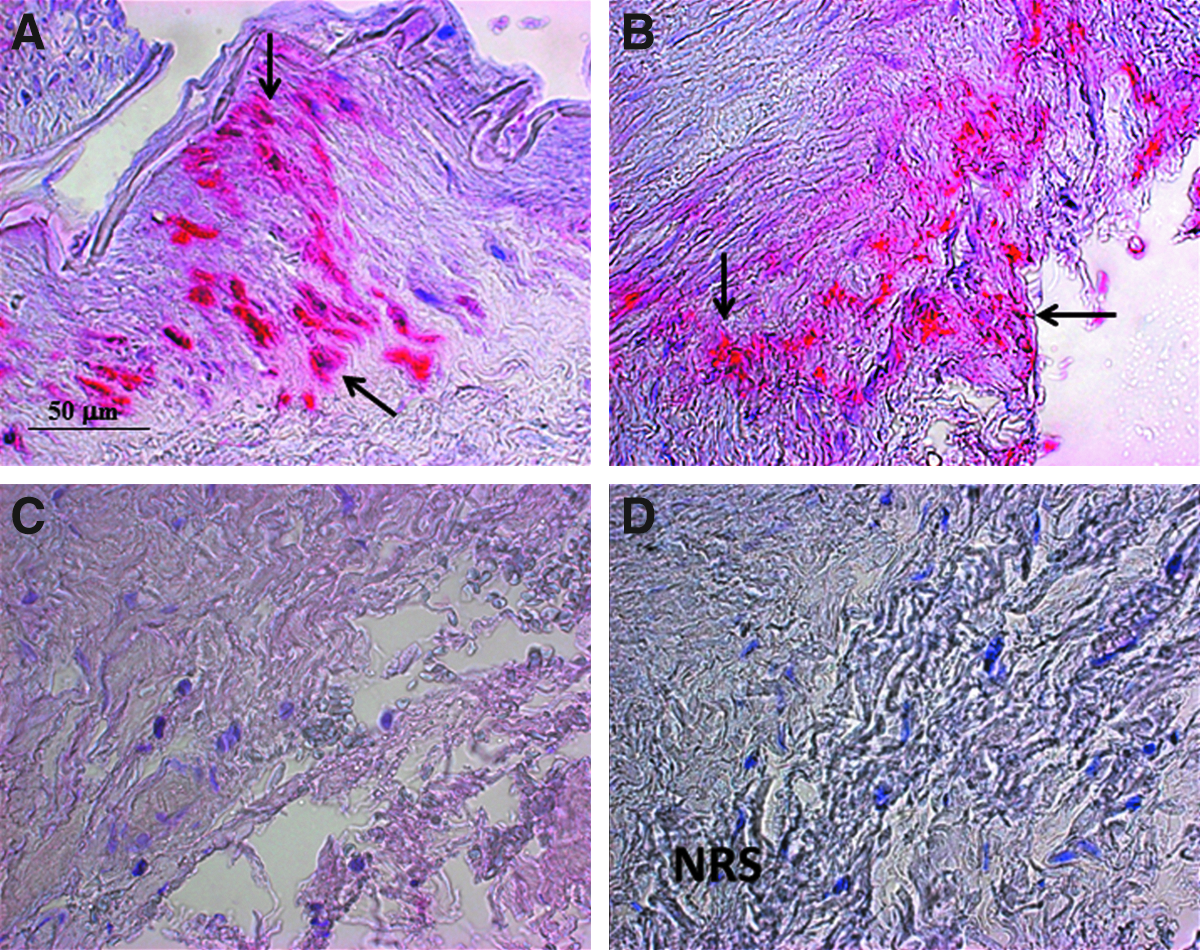
Immunohistochemical analysis of the ipsilateral temporal artery of a patient with ischemic optic neuropathy, acute retinal necrosis, and no history of zoster rash. Sections of the temporal artery were prepared and immunostained as described in Figure 1. Note VZV antigen in a positive control cadaveric cerebral artery 14 days after VZV infection in vitro (
Search for VZV in GCA-negative Temporal Arteries
These remarkable cases were followed by studies to address the incidence of VZV infection in patients with biopsy-negative GCA temporal arteries. Immunohistochemical examination of archived biopsy-negative temporal arteries for the presence of VZV antigen from patients with clinically suspect GCA revealed VZV in five (21%) of 24 such temporal arteries (Fig. 4).(9) All five subjects whose temporal arteries contained VZV antigen had presented with clinical and laboratory abnormalities of GCA and early visual disturbances, indicating that multifocal VZV vasculopathy can present with the full spectrum of features seen in GCA.
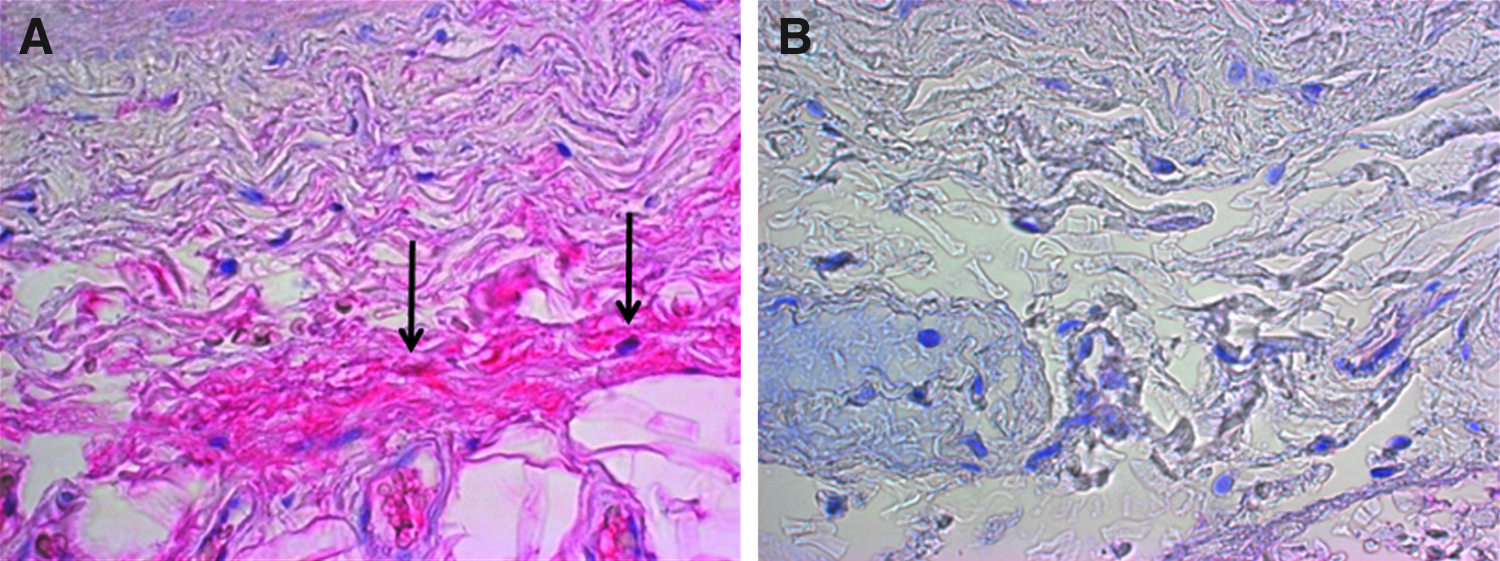
VZV antigen in a biopsy-negative temporal artery from a subject with clinically suspected giant cell arteritis. Sections of the temporal artery were prepared and immunostained as described in Figure 1. Note VZV antigen exclusively in the adventitia after immunohistochemical staining with anti-VZV IgG antibody (
The continuing search for VZV antigen in GCA-negative temporal arteries also revealed abundant VZV antigen as well as VZV DNA in multiple regions (skip areas) of a GCA-negative temporal artery and in skeletal muscle adjacent to the infected temporal artery (Fig. 5); additional pathological analysis of sections adjacent to those containing viral antigen showed inflammation involving the arterial media and abundant multinucleated giant cells characteristic of GCA (Fig. 5),(10) consistent with a possible causal role for VZV in GCA.
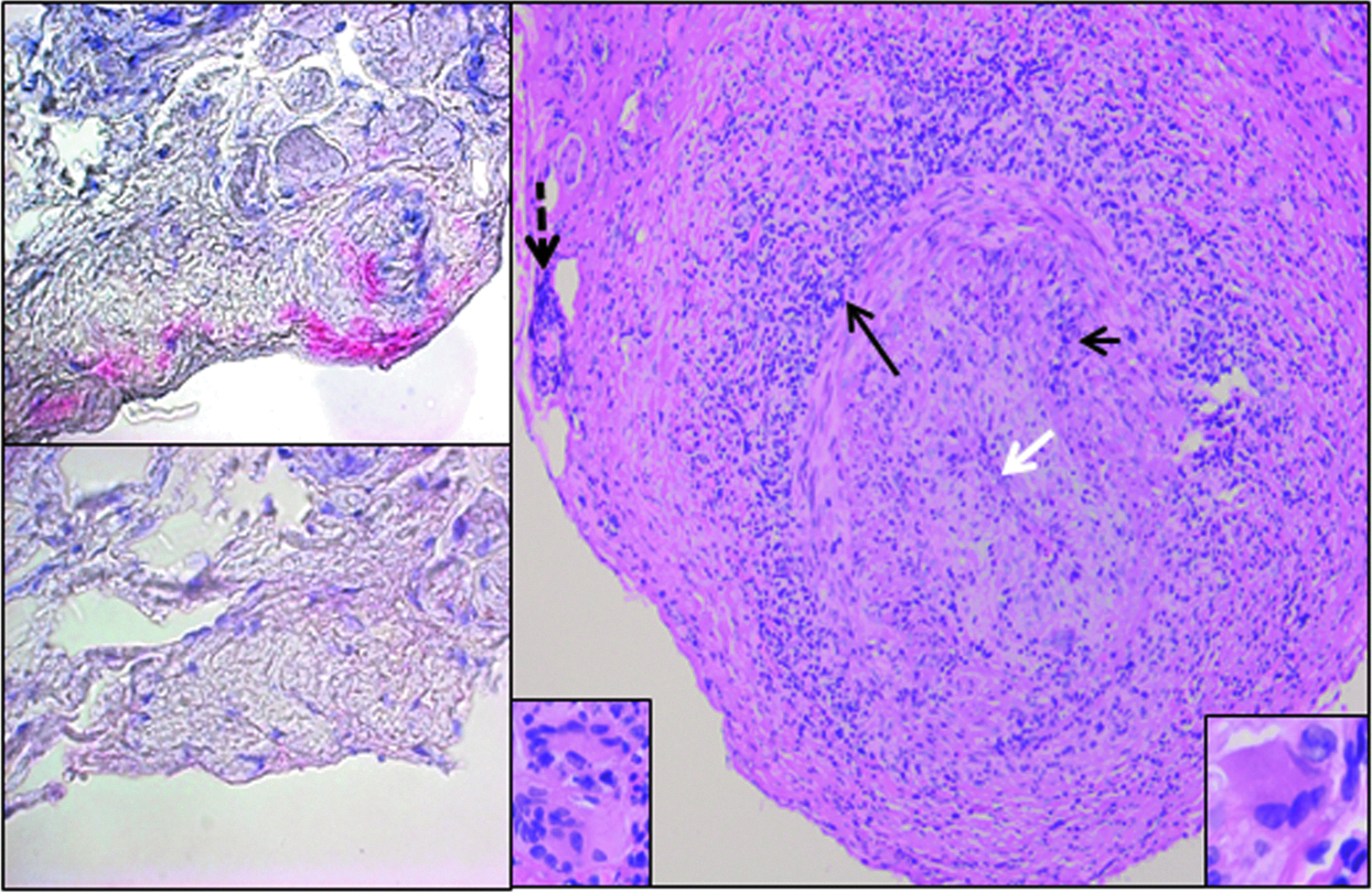
VZV antigen in a biopsy-negative temporal artery from a subject with clinically suspected giant cell arteritis. Sections of the temporal artery were prepared and immunostained as described in Figure 1. Note VZV antigen in the adventitia after immunohistochemical staining with anti-VZV IgG antibody (top left), not seen after staining with anti-HSV-1 antibody (bottom left). Hematoxylin & eosin staining of sections of the temporal artery adjacent to where VZV was found (right panel) revealed extensive inflammation in the adventitia (long black arrow), as well as inflammation in the media (short black arrow) and the vaso vasorum (dashed black arrow). White arrow spans the thickened intima and points to an occluded lumen. Numerous multinucleated giant cells were seen throughout the artery (insets). 600x magnification. (Reproduced with permission from Nagel MA, et al: J Neurol Sci 2013;335:229-230.)
Co-morbidities That Increase VZV Reactivation
Currently both normal extracranial temporal arteries and GCA-positive temporal arteries are under intense search for VZV. As the results of these important studies become available, it is important to remember that the percent of humans whose normal intracranial arteries contain VZV antigen correlates positively with the number of 5 μm sections examined. If VZV is a major cause of GCA; statistical significance must be achieved pathologically and virologically after examination of large numbers of sections from GCA-positive and from normal temporal arteries obtained at autopsy from people over 50 years old, the age group that develops GCA.
Other co-morbidities may also increase VZV reactivation. For example, although initial studies of cerebral arteries from subjects without a history of transient ischemic attacks or stroke revealed no VZV DNA or VZV antigen,(11) both were found in the cerebral arteries of a subject with diabetes,(12) a known risk factor for VZV reactivation and zoster.(13) Most recently, additional analysis of 55 cerebral arteries from 18 subjects with co-morbidities that may increase the risk of VZV reactivation (i.e., a history of alcohol abuse, tricyclic antidepressant intoxication, cocaine abuse, HIV, or being over age 70) detected VZV antigen in 24/55 (44%) arteries from 14/18 (78%) subjects.(14) These findings support the notion that VZV infection of intracranial cerebral arteries may be a significant cause of stroke in the elderly, in HIV+individuals, and other at-risk subjects.
Addendum/Closure
Surely if Hilary Koprowski were alive today, he would sense the excitement that links VZV with GCA. In fact, given his creativity, he would be one of the first to offer critical suggestions to further determine how best to prove cause, not merely association. HK is sorely missed in many ways.
Footnotes
Acknowledgments
This work was supported in part by Public Health Service grants AG032958 and AG006127 from the National Institutes of Health. The author thanks Marina Hoffman for editorial assistance and Lori DePriest for word-processing and formatting.
Author Disclosure Statement
The author has no financial interests to disclose.