
Abstract
Monoclonal antibodies (mAbs) had received emergency use authorization for mild-to-moderate coronavirus disease 2019 (COVID-19) or for prophylaxis against COVID-19, including casirivimab plus imdevimab (C+I), bamlanivimab plus etesevimab (B+E), tixagevimab plus cilgavimab (T+CG), and sotrovimab (S) and bebtelovimab (BEB). This systematic review was done to assess the efficacy and safety of the same. PubMed, Embase, Scopus, medRxiv, bioRxiv, and FDA fact sheets were searched for the studies published between January 2021 and May 2022, and appropriate search terms related to the mentioned mAbs were used for data collection. Review included original research including randomized clinical trials and observational studies published or preprints. Studies included in the review had compared with placebo or standard of care or no treatment or mAbs with each other and also of various doses. Data extraction was done and reviewed the same for both efficacy and safety. Total of 20 studies were included in this review. The rate of hospitalization within 30 days showed ∼2% in comparison to ∼7% with placebo. Significant reduction in viral load was more observed with combination mAbs. Combination therapy showed faster virological cure against the Gamma variant. With C + I as postexposure prophylaxis (PEP), 29.0% of asymptomatic participants developed symptomatic COVID-19. Pre-exposure prophylaxis with T+CG reduced the incidence of infection by 77%. Infusion-related reaction was the most common adverse event (AE). The neutralizing mAbs reduced hospitalization in mild-to-moderate patients with infusion-related reactions as common AE. The response was better in the seronegative patients. Most of these studies were conducted in unvaccinated individuals and against Alpha, Gamma, and Delta variants.
Introduction and Background
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has been an ongoing pandemic, having its impact on global health care system causing significant mortality with its emerging variants. Once a person gets infected with this virus, based on the immune system's capacity to fight against the same, some patients will experience dysregulated host immune response, overexpression of inflammatory markers leading to wide range of clinical manifestations ranging from mild upper respiratory tract symptoms to severe acute respiratory distress syndrome (ARDS), which may further lead to respiratory compromise and death.1,2
Antiviral drugs such as remdesivir, approved drug by the U.S. FDA, though initially believed to be effective in treating mild-to-moderate COVID-19, was later found to be of not much use.3,4
Mild COVID-19 patients are usually managed at home (nonhospitalized) with symptomatic treatment. Patients with risk factors such as older age (≥65 years), obesity, pregnancy, chronic kidney disease, diabetes, immune compromised/on immunosuppressive treatment, cardiovascular disease or hypertension, chronic lung diseases, and neurodevelopmental disorders are more prone to develop severe disease. Remdesivir is the first antiviral drug approved by the U.S. FDA for hospitalized COVID-19 patients that is available as injectable preparation.
Later molnupiravir and nirmatrelvir plus ritonavir oral antiviral agents received emergency use authorization (EUA) by the U.S. FDA for mild-to-moderate COVID-19 patients who are at high risk for severe disease.5,6 These drugs have to be used within 5 days of symptom onset.
The U.S. FDA has also given EUA for monoclonal antibodies (mAbs) such as casirivimab plus imdevimab (C+I) combination, bamlanivimab plus etesevimab (B+E) combination, sotrovimab (S), and bebtelovimab (BEB) for the treatment of mild-to-moderate COVID-19 in adult and pediatric patients >12 years of age who are at high risk for progression to severe COVID-19, including hospitalization or death. The C + I combination and B + E combination also received EUA for post-exposure prophylaxis (PEP).7–10
Tixagevimab–cilgavimab (AZD7442; T+CG) has received EUA for pre-exposure prophylaxis (PrEP) in adults and pediatric patients ≥12 years who are not currently infected with SARS-CoV-2 and immunocompromised individuals who may not mount an adequate response to COVID-19 vaccination, and for individuals for whom COVID-19 vaccination is not recommended due to a history of a severe adverse reaction. 11
For the prevention of COVID-19 infection, vaccination may help. The difference between vaccines and mAbs is the efficacy. Vaccines will give protection for longer period whereas mAbs protection will be of shorter duration. Nevertheless, the mAbs will be useful as immediate option for prevention of COVID-19 infection in high-risk individuals.
All these neutralizing mAbs have a similar mechanism of action where they prevent binding of virus to the angiotensin converting enzyme 2 (ACE2), thereby preventing the entry into human cells and thus neutralizing the virus (Fig. 1).9–14 Most of the mAbs receiving EUA are the combination of two mAbs. This combination of mAbs has been given approval to reduce escape mutation and to show more effectiveness. The pharmacokinetic parameters, the activity of mAbs against various SARS-CoV-2 variants, dose, and other details are given in Table 1.
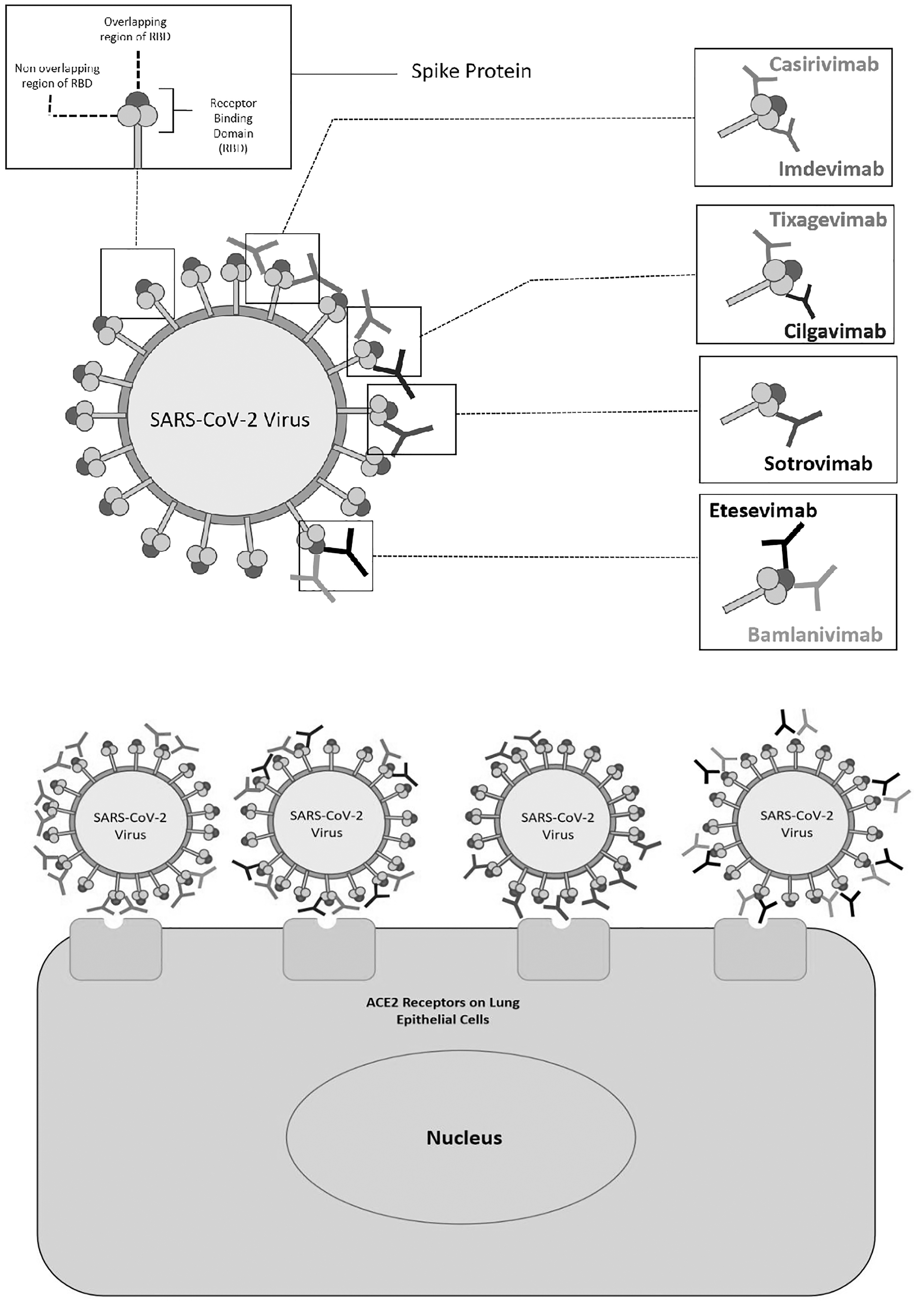
Mechanism of action of anti-SARS-CoV-2 mAbs. All these neutralizing mAbs have a similar mechanism of action, where they act as neutralizing antibodies by binding to the RBD of the viral spike protein and inhibit the attachment of the virus to human ACE2, but with different binding affinities. They bind to either overlapping or nonoverlapping epitopes on RBD, prevent virus binding to the ACE2, thereby preventing the entry into human cells and thus neutralizing the virus. Sotrovimab, tixagevimab–cilgavimab bind in a region of the RBD that does not overlap with the ACE2 binding site and others will bind to overlapping site. The bind site for bebletovimab was not reported in the literature.9–14 ACE2, angiotensin converting enzyme 2; mAb, monoclonal antibody; RBD, receptor binding domain; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Pharmacokinetics and Pharmacodynamics of Anti-SARS-CoV-2 Monoclonal Antibodies for COVID-19
Age, gender, race, body weight, disease severity.
No data available.
No data available in moderate-to-severe hepatic impairment.
ACE2, angiotensin converting enzyme 2; COVID-19, coronavirus disease 2019; EUA, emergency use authorization; IV, intravenous; mAb, monoclonal antibody; NA, not available; PK, pharmacokinetics; RBD, receptor binding domain; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
There is one systematic review conducted by Kreuzberger et al. to assess the effectiveness and safety of SARS-CoV-2-neutralizing mAbs for treating patients with COVID-19 by including the clinical trials on the mAbs published between January 2020 and June 2021. The data from the four studies in nonhospitalized participants who have received either bamlanivimab or bamlanivimab/etesevimab or sotrovimab or regdanvimab showed low certainty of evidence and very low-to-moderate evidence for hospitalized patients who had received either bamlanivimab or casirivimab/imdevimab. 15
Later many other anti-SARS-CoV-2 mAbs were approved; many studies published with these mAbs against changed COVID-19 variants. After July 2021, the Omicron variant has become the dominant SARS-CoV-2 variant in most parts of the world. In in vitro neutralization assays, Omicron variant and its subvariants have shown reduced susceptibility to many anti-SARS-CoV-2 mAbs especially bamlanivimab plus etesevimab and casirivimab plus imdevimab. Sotrovimab is active against the Omicron BA.1 and BA.1.1 subvariants, but reduced susceptibility with other subvariants.
Bebtelovimab that received approval recently had shown retaining of the neutralizing activity against circulating Omicron subvariants.16–18 Tixagevimab–cilgavimab also known as AZD7442, a long-acting antibody combination, given as two consecutive intramuscular injections, one each of tixagevimab and cilgavimab also received EUA for prophylaxis of COVID-19.
Considering the approval of many anti-SARS-CoV-2 antibodies and change in variants, there is a need to do systematic review on efficacy and safety of these mAbs used for either treatment or for PrEP of COVID-19.
Objectives
Primary objective
To assess the efficacy and safety of SARS-CoV-2-neutralizing mAbs in the treatment mild-to-moderate COVID-19 patients
Secondary objective
To assess the efficacy and safety of SARS-CoV-2-neutralizing mAbs in prevention of COVID-19 infection
Materials and Methods
Study designs
Clinical studies conducted that evaluated the effect of mAbs either in combination or as monotherapy were considered for the review. Both prospective and retrospective studies using these mAbs for treatment of mild COVID-19 nonhospitalized patients or as PrEP have been included in the analysis. The search words used are bamlanivimab (B) alone or bamlanivimab plus etesevimab (B+E), casirivimab plus imdevimab (C+I), sotrovimab, bebtelovimab, and tixagevimab–cilgavimab (T+CG).
Original research articles and articles with full text published and preprints only were considered. Review articles, editorials, conference proceedings, author responses, commentaries, preclinical studies, and book chapters were excluded. Studies with duplicates or exact matching or data that cannot be reliably extracted were also excluded.
We included studies that compared with placebo or standard of care or no treatment or other mAbs with each other and also studies that compare several doses of one type of mAb with another treatment, placebo, or no treatment.
Search strategy
Search engines such as PubMed, Embase, Scopus, medRxiv (preprint), bioRxiv (preprint), and FDA fact sheets were searched for studies published between January 2021 and May 2022. Search strategy using MeSH terms is mentioned in Table 2.
Search Strategy Using MeSH Terms
Data extraction and management
Two authors (G.R., K.R.M.) independently extracted data using a standard data extraction sheet. The extracted data included general characteristics of the articles, study population, intervention details, samples size, male and female ratios, median age, and study type and outcome parameters as per the study objectives. Discrepancies were resolved by discussion or by third author.
Statistical analysis
As this is a qualitative synthesis of evidence, no statistical test was applied for comparison.
Study registration
The study was not registered in PROSPERO.
Risk of bias
Risk of bias assessment was not done.
Outcomes reviewed
Primary outcome
Rate of hospitalization or emergency department (ED) visit or death within 30 days.
Secondary outcomes
Change in viral load
Median time for symptom resolution
Proportion of patients requiring intensive care unit (ICU) admission
Duration of hospitalization
Mortality on day 28
Proportion of patients experiencing adverse events (AEs) and serious adverse events (SAEs).
Results
In total of 10,651 articles were screened. After duplication, 7613 articles were considered for further analysis. Figure 2 shows summarizing of the search strategy. The literature search identified 30 full-text articles, of which 20 studies were eligible for inclusion in this review after a full-text read.

Study flow chart. The flow chart shows the details of our search and selection of articles during the review process.
A total of 28,447 patients were included, of which 13,974 patients received mAbs and 14,473 received standard care or placebo and two studies compared the efficacy and safety of mAbs against the other mAb combination. Prophylactically 3460 patients received mAbs. The details of the number of studies for each mAb are shown in Figure 3. Most of the studies included in this review were conducted in mild nonhospitalized COVID-19 patients and one study was conducted in hospitalized patients and two studies prophylactically. Most of the studies compared mAbs with placebo, and in three studies they were compared with other anti-SARS CoV-2 mAbs. The results were discussed as primary and secondary outcomes.
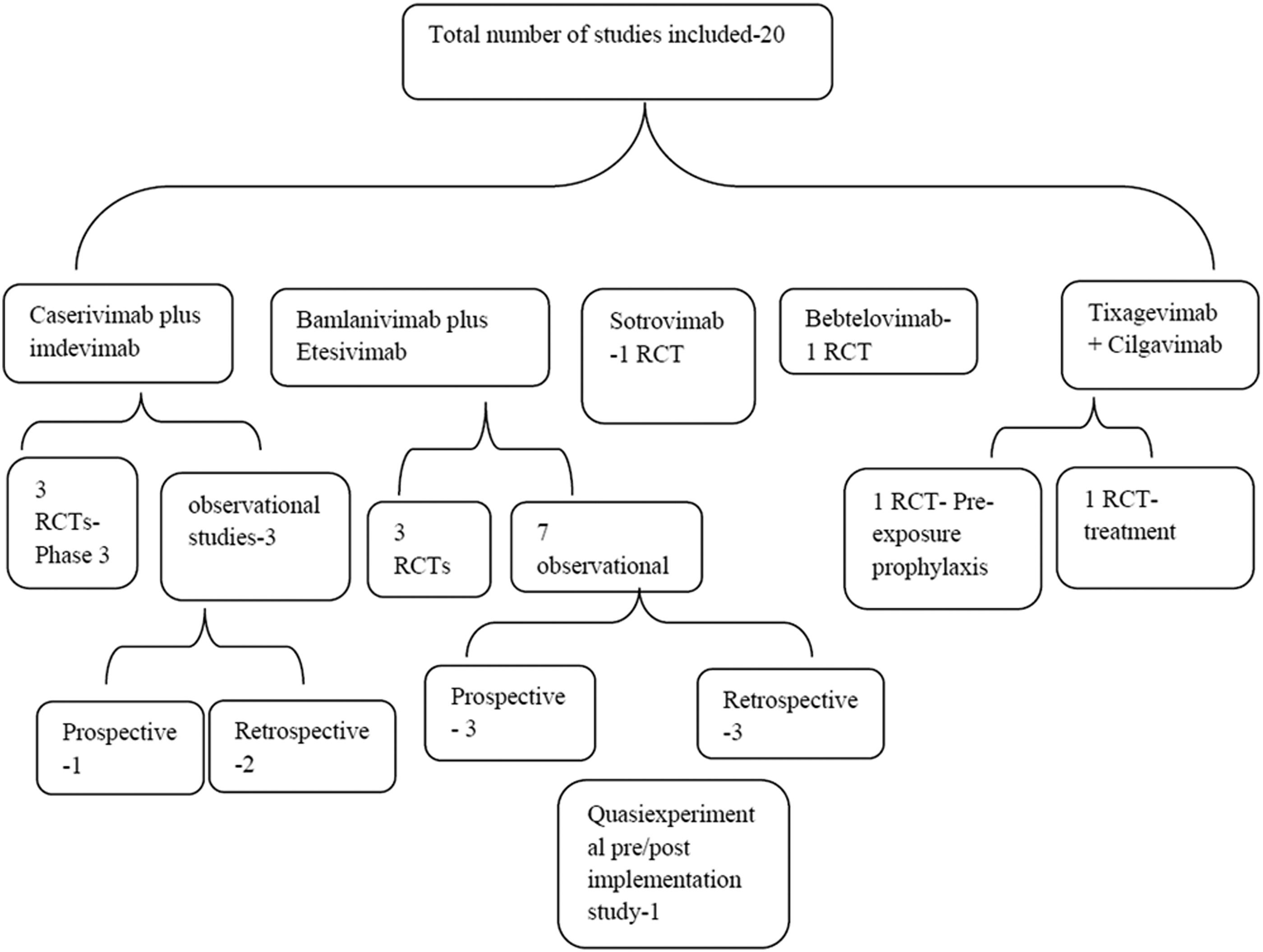
Details of collected articles. The diagram shows the number of articles included in this review based on the type of mAb and study.
Primary outcomes
Rate of hospitalization or death within 30 days
Most of the mAbs were evaluated in nonhospitalized mild COVID-19 patients who are at high risk for progressing to severe disease. Hence rate of hospitalizations or death or ED visit within 30 days was the outcome parameter measured in most of these studies. There were 10 studies conducted with either bamlanivimab alone or combination of B+E. Out of these, three were randomized controlled trials (RCTs), three studies were retrospective, three were prospective observational studies, and one was a quasi-experimental study.
The absolute risk ratio (ARR) of COVID-19-related hospitalization or death from any cause by day 29 with combination of B + E (dose 2800 + 2800 mg) was −4.9% (95% confidence interval [CI], −8.9% to −0.8%; p = 0.049) 19 and −4.8%; (95% CI, −7.4 to −2.3; p < 0.001). 20 Monotherapy of bamlanivimab at 2800 mg showed ARR of −3.9% (95% CI, −8.4% to 0.6%; p = 0.21) in a prospective study. 19
Significant reduction in the rate of hospitalization or death or ED visit was reported in other prospective studies and was found to be 2.5% versus 3.9%, 23 6.9% versus15.5%, 26 12.1% versus 20.3% with B compared with control, respectively. 27 In retrospective studies, 1.9% versus 12% (p < 0.01), 22 7.3% versus 20.0%, 24 and 6.3% versus 39.3% 25 with bamlanivimab treatment compared with control group, respectively.
In a quasi-experimental study where B was compared with C+I, results showed that 14-day hospitalization or all-cause mortality was 12.1% (B) compared with 8.7% in (C+I)-treated group with odds ratio (OR), 0.52 (95% CI, 0.17 to 1.63, p = 0.26). 28
In an RCT study, C + I showed that the relative risk reduction (RRR) was 71.3% (p < 0.001) and 70.4% (p = 0.002) with 2400 and 1200 mg, respectively. 30 The C + I was compared with B + E in a prospective observational study where the hospitalization/death within 30 days was 4.3% versus 5.7% and 17.4% versus 55% (p = 0.013) against Alpha (B.1.1.7) and Gamma (P.1) variants, respectively. 32 In retrospective studies it was 1.6% and 2.6% with C + I compared with control (4.8% and 16.6%).33,34
Efficacy of this combination mAbs in vaccinated and unvaccinated persons infected with Delta variant was studied by Bierle et al. and results showed that there was a significant decrease in the rate of hospitalization 2.6% (C+I) compared with the control group 16.6%. 34
Only one RCT was conducted with sotrovimab at 500 mg intravenous (IV) infusion in 1057 mild-to-moderate COVID-19 patients, who are at risk for progressing to severe disease. The interim analysis of this COVID-19 Monoclonal Antibody Efficacy Trial–Intent to Care Early (COMET-ICE) trial had shown significant reduction in hospitalization, ED visit OR death, with single infusion of sotrovimab, and it was 2% (sotrovimab) versus 7% (placebo) with absolute difference of −4.91% (95% CI, −7.50% to −2.32%; p < 0.001). 35
The BLAZE-4 trial tested single IV infusion of BEB (175 mg) and combination of BEB + B (700 mg) + E (1400 mg) in low- and high-risk patients with mild-to-moderate COVID-19, within 3 days of first real time-polymerase chain reaction positive test. A total of 706 patients were recruited in the study. Authors reported that COVID-19 hospitalization was equal in BEB (1.6%) and placebo (1.6%) and 2.4% with BEB+B+E in the low-risk group. 36
Secondary outcomes
Change in viral load
Significant reduction in SARS-CoV-2 log viral load −0.57 (95% CI, −1.00 to −0.14; p = 0.01) and −1.20 (95% CI, −1.46 to −0.94; p < 0.001) at days 11 and 7 was reported with combination of B + E (2800 + 2800 mg), respectively.19,20
The C + I combination had shown significant decrease in number of weeks of high viral load (>4 log10 copies/mL) in nasopharyngeal swab samples per 1000 participants (489.8 [C+I] vs. 811.9 [placebo]). 29
The same combination in another RCT showed reduction in viral load by day 7, from baseline −0.71 log10 copies/mL (95% CI, −0.90 to −0.53) with 1200 mg and −0.86 log10 copies/mL (95% CI, −1.00 to −0.72) with 2400 mg. 30
In one study, B + E was compared with C + I for time to virological cure against Alpha and Gamma variants and it was 14 versus 15 and 17 versus 14 days, respectively. Results were significant against Gamma variant. 32
Median time for symptom resolution
The change in symptom resolution from baseline to day 11 with treatment of B + E was 9.0% (95% CI, −3.1% to 21.1%; p = 0.16). 19 It was reported that (C+I) caused reduction symptomatic duration per 1000 participants (895.7 weeks vs. 1637.4 weeks [placebo]; p = 0.03) 29 and time for COVID-19 symptoms to resolve was significant (14 [C+I] vs. 18 days [P] p < 0.001). 30
The BLAZE 4 trial showed time to symptom resolution was less in BEB (6%)-treated group compared with the group treated with combination BEB+B+E (7%) and placebo (8%) in the low-risk group. 36
Proportion of patients requiring ICU admission, duration of hospitalization, mortality on day 28, and other details are given in Table 3.
Efficacy Data of the Anti-SARS-CoV-2 Monoclonal Antibodies in COVID-19
AE, adverse event; ARR, absolute risk ratio; B, bamlanivimab; B+E, bamlanivimab plus etesevimab; BEB, bebtelovimab; C+I, casirivimab plus imdevimab; CI, confidence interval; ED, emergency department; ICU, intensive care unit; IQR, interquartile range; OR, odds ratio; ; RCT, randomized controlled trials; RR, rate ratio; RRR, relative risk reduction; RT-PCR, real time-polymerase chain reaction; SD, standard deviation; SAE, serious adverse event.
Others
T+CG was studied in the TACKLE COVID-19 treatment trial and results showed 50% reduction in the risk of developing severe COVID-19 or death (from any cause) compared with placebo in mild-to-moderate symptomatic COVID-19 patients. The findings of this study were released through the media by Astra Zeneca after primary analysis of 822 participants data. 38
Safety outcomes: Proportion of patients experiencing AEs and SAEs were shown
Prophylaxis
Phase 3 RCT was conducted with C + I as PEP in 214 asymptomatic COVID-19 adults and adolescents (Table 4). Study results reported that the proportion of participants developing symptomatic COVID-19 on day 28 was 29.0% (C+I) versus 42.3% (placebo) with ARR, −13.3% (95% CI, −26.3% to −0.3%). 29
Safety Outcomes of Anti-SARS-CoV-2 Monoclonal Antibodies
BP, blood pressure; ETE, etesevimab; GI, gastrointestinal; TEAE, treatment emergent adverse events; UTI, urinary tract infections.
PROVENT trial studied the single dose of AZD7442 (T+CG) for PrEP against COVID-19 in adults who were at an increased risk of exposure to SARS-CoV-2 COVID-19 and an inadequate response to COVID-19 vaccination. The results showed that AZD7442 reduced the incidence of infection by 77% (95% CI, 46% to 90%; p < 0.001) after median follow-up of 183 days and 82% after post hoc analysis.
Discussion
The present review was done to know the efficacy and safety of neutralizing anti-SARS CoV-2 mAbs against COVID-19. REGEN COV mAb (C+I) was the first drug received EUA and it was most commonly used during third wave in India. A total of 20 studies were included for review, and in these studies, mAbs were tested either alone or combination of mAbs. The combination was used mainly to decrease the loss of antiviral activity on different variants and escape mutants.
Bamlanivimab, and T+CG were derived from B lymphocytes of a convalescent naturally SARS-CoV-2-infected person. The EUA given to bamlanivimab was revoked by U.S, FDA on April 17, 2021, due to an increase in virus variants that are resistant to viral neutralization. 39 The efficacy of these mAbs against various variants of SARS CoV-2 was tested in in vitro through pseudo type neutralization assays. 40
Efficacy and safety of the neutralizing anti-SARS CoV-2 mAbs varied across the studies. Proportion of patients with hospitalization, change in viral load, and symptom resolution were the common efficacy end points evaluated in nonhospitalized mild COVID-19 patients, and 28-day mortality or all-cause mortality was the primary end point in hospitalized patients. ACTIV-3 and RECOVERY trial were conducted in hospitalized patients, whereas other studies were conducted in mild COVID-19 nonhospitalized patients.
Rate of hospitalization within 30 days was ranging from 2% to 6% with treatment of these neutralizing mAbs. The other drugs that received EUA for mild COVID-19 nonhospitalized patients were oral antiviral preparations such as molupiravir and paxlovid (combination of nirmatrelvir and ritonavir). These drugs should be administered within 3–5 days of symptom onset. Phase 3 clinical MOVe-OUT trial conducted with molnupirvair in mild-to-moderate non-hospitalized patients with at least one risk factor showed 7.3% hospitalization for any cause or had died through day 29 compared with 14.1% in placebo group. The difference was significant and it was reported −6.8 percentage (95% CI, −11.3 to −2.4; p = 0.001). 41
With paxlovid, significant difference (−5.81% [95% CI, −7.78 to −3.84]; p < 0.001) was observed in the incidence of COVID-19–related hospitalization or death by day 28 and it was 0.72% and 6.45% in paxlovid and placebo group, respectively. 42
The C + I combination (REGEN-COV) is available as prefilled syringe subcutaneous injection and also for IV infusion. This drug was approved for both mild-to-moderate COVID-19 patients who are at high risk for progression to severe COVID-19, including hospitalization or death and PEP of COVID-19 in individuals who are at high risk for progression to severe COVID-19 and not fully vaccinated or who are not able to induce an adequate immune response to COVID-19 vaccination. It has been mentioned in the U.S. FDA prescriber information that mAbs, such as REGEN-COV, may be associated with worse clinical outcomes when administered to hospitalized patients with COVID-19 requiring high flow oxygen or mechanical ventilation.
This drug was tested in the RECOVERY trial in hospitalized patients. About 6% of hospitalized patients were on invasive mechanical ventilation at the base line. It has been reported that fever, sudden hypotension, and thrombotic events were numerically high in the C + I group than in the usual care group. Seven SAEs were reported in these trials in the test group. The dose used in this trial was high and it was casirivimab 4 g and imdevimab 4 g.
In the PROVENT trial, T+CG had shown protective effect against COVID-19 in unvaccinated individuals, and during the testing with drug, the variants identified in the study population were Alpha, Beta, and Delta variants. The results of this trial will be applicable to people infected with these variants but not to Omicron variant. The same situation was observed when C + I combination was tested as PEP.
The National Institutes of Health (NIH) COVID-19 Treatment Guidelines Panel recommends the use of tixagevimab/cilgavimab as PrEP and recommends against the use of the combinations bamlanivimab/etesevimab and casirivimab/imdevimab as PEP (NIH). 43
There is only one study reporting the effectiveness of these mAbs against Alpha and Gamma variants. The C + I combination showed significant decreases in hospitalization or ICU admission or faster virological cure of mild-to-moderate COVID-19–infected patients with Gamma variant. At present, Omicron variant is the major variant of concern, and efficacy against this variant is not known.
Bruel et al. reported noticeable differences in the sensitivity of BA.1 and BA.2 Omicron variants to therapeutic neutralizing mAbs. They compared the sensitivity of BA.1 and BA.2 variants to neutralization by nine therapeutic mAbs. The BA.2 variant showed sensitivity to cilgavimab, inhibition partly by imdevimab, and resistance to sotrovimab. In patients' sera, this anti-Omicron neutralizing activity was reduced when C + I and T+CG were given to immunocompromised individuals. 44
More clinical studies need to be conducted to know the effectiveness of these mAbs against variants of Omicron for either treatment or disease prevention. The U.S. FDA has revised its EUA in April 2022 on sotrovimab and mentioned that sotrovimab is no longer authorized to treat COVID-19 in any U.S. region due to the majority of COVID-19 cases were caused by the Omicron BA.2 subvariant. In in vitro assays, sotrovimab has not shown neutralization against Omicron variant. 9
The significant reduction in viral load was observed more with B + E than with C + I on day 7. The broad-spectrum antiviral drug aprotinin was tested in phase 3 clinical trial, ATAC (aprotinin treatment against COVID-19), and results showed that aprotinin nebulization caused significant reduction (p = 0.016) in viral load levels on day 5 in hospitalized moderate COVID-19 patients. Reduction was 3.9 log10 copies/mL compare with base line. Aprotinin is a host proteases inhibitor and proteases are used by the virus to cleave the viral “spike” protein and subsequently be able to recognize surface receptors on epithelial cells to infect. Neutralizing mAbs and aprotonin target the viral spike protein. 45
In a phase 2a trial, administration of 800 mg of molnupiravir in mild COVID-19 patients showed significant difference in the least squares mean viral load change from baseline n day 7 compared with the placebo group (−0.534 log10 copies/mL [p = 0.006]) 46
In the RECOVERY trial, the primary efficacy was all-cause mortality and it was less in seropositive (16%) patients than in seronegative (24%) patients, and other outcomes were better in seronegative patients.
Among the AEs reported, gastrointestinal-related AEs were most commonly reported followed by infusion-related reactions. SAEs were reported in majority of the studies included. Most of these mAbs are available as injection for IV route of administration and requires hospital setup for administration of these drugs. Infusion-related reactions were the most common AEs reported in these studies
Most of the studies conducted with mAbs for treatment of nonhospitalized COVID-19 patients observed the outcomes for 1 month maximum and it was 6 months in prophylaxis studies. No study has reported the duration of protection of these mAbs against COVID-19. For PrEP, T+CG is authorized to be administered every 6 months and with advisory note that the combination is not a substitute for COVID-19 vaccination. 11
Conclusion
The anti-SARS CoV-2 mAbs with EUA by U.S. FDA have shown reduced hospitalization in mild-to-moderate patients with infusion-related reactions as common adverse effects. When these mAbs were given as prophylactic agents, the occurrence of symptomatic COVID-19 decreased. As the response to mAbs in seropositive COVID-19 patients could not be assessed, further studies in this cohort is required.
The important limiting factor for wider use of these mAbs is their cost. Most of these studies were conducted in unvaccinated individuals and against Alpha, Gamma, and Delta variants. There are unanswerable questions regarding the use of these drugs such as duration of protection, efficacy in immune disorder patients, and against the emerging variants.
Limitations
Meta analysis was not done due to difference in interventional drugs, drug combination, dosage, and multiple arms in the studies reported.
Footnotes
Acknowledgment
The authors are very thankful to Dr. Bhavani Sankara Bagepally Scientist D, ICMR-NIE, Chennai, Tamilnadu, India, for his help during article collection.
Authors' Contributions
Concept design of the study was carried out by M.E. and V.R.K. Methodology was by M.E. and G.R. Articles collection was by G.R. and K.R.M. Figure was drawn by L.F.C. Article draft was taken care by G.R., M.E., and V.R.K. Article review was by D.B., G.M.R., and R.P.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.