
Abstract
One of the most potent therapeutic and diagnostic agents in contemporary medicine is the monoclonal antibody (mAb). mAbs can perform a variety of tasks in breast cancer (BC), including identifying and delivering therapeutic medications to targets, preventing cell development, and suppressing immune system inhibitors including directly attacking cancer cells. mAbs are one of the most effective therapeutic options, particularly for HER2, but they have not been well studied for their use in treating other forms of BC, particularly triple negative breast tumors. Bispecific and trispecific mAbs have created new opportunities for more targeted specific efficacy, which has a positive impact on the viability of antigen specificity. They are more versatile and effective than other forms of treatment, emerging as most popular option for treating BC. However, mAbs have a limit in treatment due to certain adverse effects, including fever, shaking, exhaustion, headache, nausea, and vomiting, as well as rashes, bleeding, and difficulty breathing. To examine the current and prospective future capacities of mAbs with regard to the detection and treatment of BC, the present review highlights advantages and disadvantages of mAb approach.
Introduction to Monoclonal Antibodies and Breast Cancer
Monoclonal antibodies
Role of monoclonal antibodies in cancer
The multitasking monoclonal antibodies (mAbs) have various methods for destroying cancer cells. Some mAbs function by sabotaging the checkpoint system, which is a signaling system produced by the cancer cell. 1 Your immune system’s checkpoints prevent it from responding to invaders and unintentionally harming healthy tissue. 2 By putting checkpoint proteins on their surface to defend them from immune system attack, cancer cells can shut down the system. 3 Some mAbs block these checkpoints, enabling T cells in your immune system to kill cancer cells that are their target. 4
mAbs and their function in breast cancer
The development of mAbs that specifically target growth factor receptors has been a highly significant advancement in the treatment of breast cancer (BC) over the last decade. 5 Conventional cancer therapies are generally indiscriminate and harmful to both healthy and malignant cells. 6 To improve the success rates of treatment and reduce harm to healthy cells, researchers are currently working on the development of novel anticancer drugs that selectively focus on the molecular abnormalities present in tumor cells. 7 Advancements in the comprehension of tumor pathobiology and molecular biology have facilitated the development of these specialized medications targeting BC. 8 BC is among the various types of cancer that exhibit the presence of the human epidermal growth factor receptor (HER; erbB) family. These receptors possess tyrosine kinase activity. 9 The vascular endothelial growth factor (VEGF) receptor has become a focus for treating BC due to its significant involvement in the formation and spread of tumors through angiogenesis. 10 The primary offenders are antibodies that specifically target VEGF and the extracellular domain of erbBs. 11
Applications
Numerous diseases, including inflammatory, cancerous, autoimmune, and cardiovascular conditions, can be treated with them. Targeted specificity, which is their primary method of action, is one of the many important benefits that mAbs provide as therapeutic agents. 12 As a result, they have a reduced toxicity and side effect profile than many small molecule medicines, which frequently accompany them. 13 Furthermore, because immunoglobulins have discrete subunit functionality, several immune system counterparts work in concert with other mAb components, such as the complement cascade that the Fc region of Immunoglobulins G (IgGs) initiates to destroy cells. 14 Therefore, it is anticipated that the therapeutic potential of MAbs would increase as more immune-modulated capabilities are discovered in the upcoming years. 15
Breast cancer
Breast tissue is where BC starts when cells change and proliferate out of control, creating a tumor. It may migrate to neighboring tissues and maybe to other body parts, where it may develop into other tumors. 16 Metastasis is a prevalent phenomenon in many types of cancer. BC, which primarily affects women over 50, is the second most common malignancy in women after skin cancer. 17 Although it is uncommon, men can have BC; in the United States, there are roughly 2600 instances each year or less than 1% of all cases. 18 While transgender males are less at risk than cisgender women, transgender women are at higher risk than cisgender men. 19
Etiology and risk factors
The development of BC is attributed to the abnormal division and rapid growth of breast cells. Age is a significant risk factor for BC, and the risk increases after reaching the age of 55. 20 Incidence of BC is significantly higher in females than in males. Genetic testing can identify that a specific defective gene, inherited from parents, is responsible for 5%–10% of breast tumors. 21 Smoking, alcohol intake, and obesity are associated with an elevated risk of both initial development and recurrence of BC. Previous radiation therapy, especially targeting the head, neck, or chest, raises the likelihood of BC in women. 22 Individuals who do hormone replacement therapy (HRT) have a higher likelihood of developing BC compared with those who do not use HRT. 23
There are multiple distinct forms of BC, which include infiltrating ductal carcinoma, ductal carcinoma in situ, infiltrating lobular carcinoma, lobular carcinoma in situ, triple negative BC (TNBC), and inflammatory BC. 24
Stages
The staging of cancer is used to describe the extent or severity of the disease in the body. The dimensions, position, and magnitude of the tumor, along with the presence of metastasis, all factor into this determination. The main stages of BC are as follows. 25

mAbs and mAbs equipped with chemotherapeutics. mAbs, monoclonal antibodies.

Production of mAbs. mAbs, monoclonal antibodies.
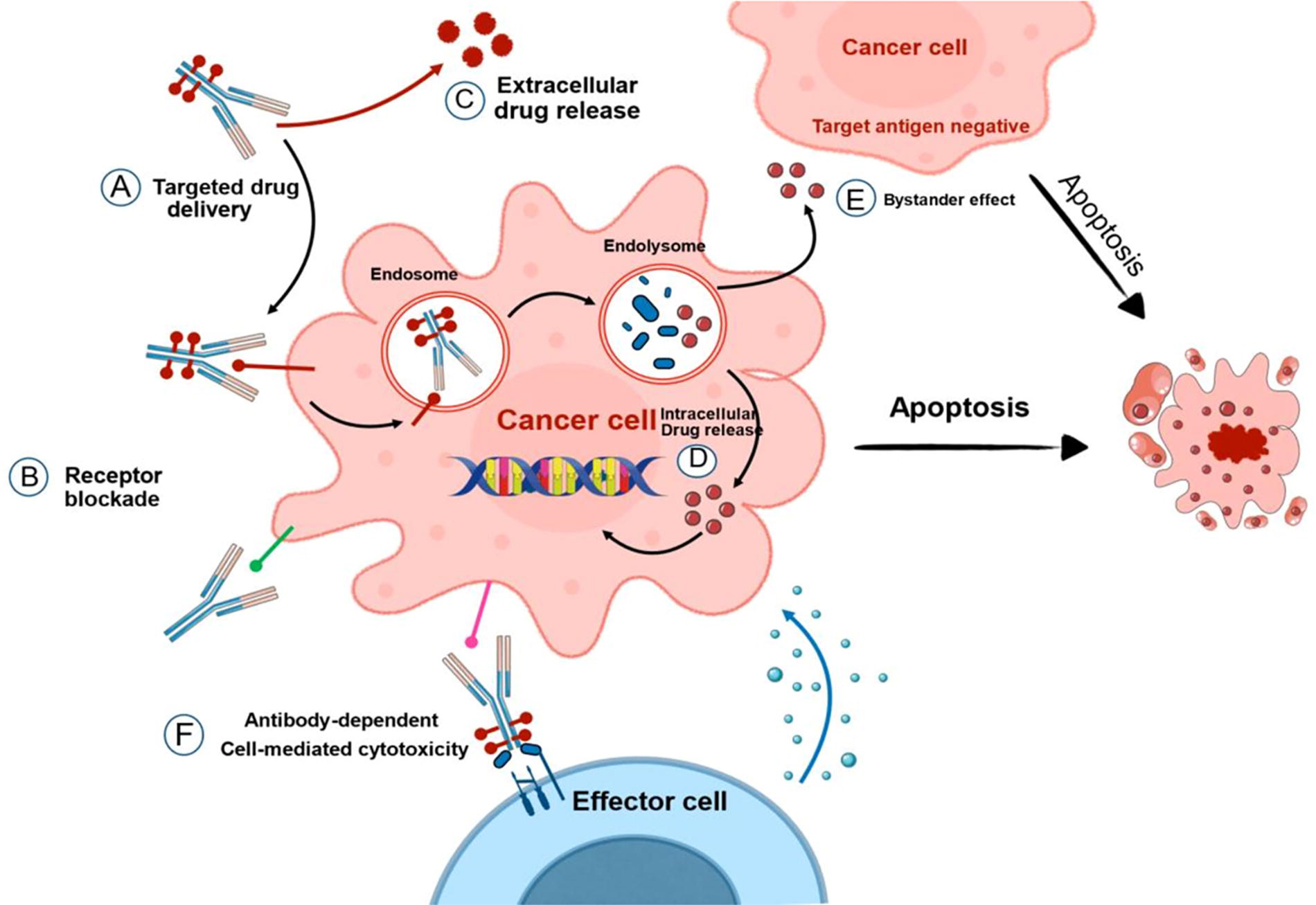
Applications of mAbs in breast cancer. mAbs, monoclonal antibodies.
Overview of clinical trials investigating mAbs
The table describes the mAbs which were undergoing clinical trials to investigate their applications in BC treatment (Fig. 4). It also includes the combination drugs along with mAbs, which enhance the therapeutic outcomes of respective mAbs. 34 Still numerous clinical trials have been going on to establish and increase the benefits of mAbs in BC therapy. Table 1 gives in detail an overview of clinical trials investigating mAbs. 35
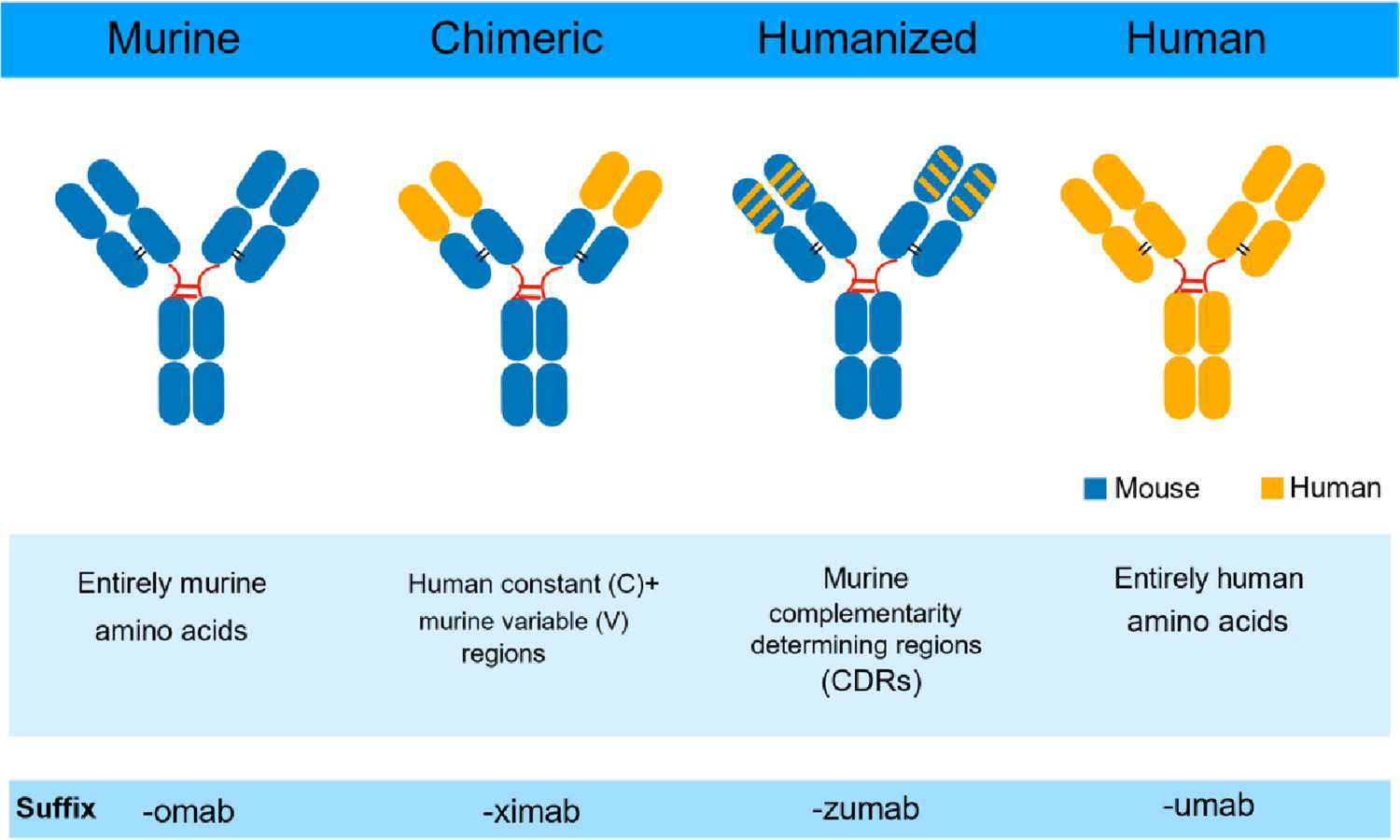
Types of monoclonal antibodies.
Overview of Clinical Trials Investigating Monoclonal Antibodies
The detailed description of the data collected is as follows:
Along with the abovementioned major drugs, many other various types of mAbs such as nivolumab, avelumab, oleclumab, panitumumab, toripalimab, and so on have been used in different clinical trials with different chemotherapy combinational agents. 48
Completed clinical trials data
Efficacy of mAbs in treating BC
Trastuzumab is an essential component of the initial treatment for HER2-positive MBC. The clinical landscape may evolve due to the introduction of novel anti-HER2 therapeutics. 106 Similar response rates were observed with capecitabine combined with lapatinib (48%), continuing trastuzumab along capecitabine (48%), pertuzumab in conjunction with trastuzumab (24%), and neratinib (24%). 107 Trastuzumab emtansine (T-DM1) exhibited a response rate ranging from 26% to 64%. Various HER2-targeted therapies can provide additive or synergistic effects, improving outcomes (Fig. 5). 108 Patients with HER2-positive MBC who are administered trastuzumab often experience the development of brain metastases. 109 Three ideas elucidate this phenomenon as follows: The disease exhibits a pronounced tropism for the central nervous system (CNS) and demonstrates a more aggressive behavior; trastuzumab enhances patient survival and leads to brain metastases, which are generally a late manifestation of the disease; nevertheless, it does not penetrate the intact blood–brain barrier.109,110 Trastuzumab did not seem to increase the incidence of brain metastases, based on data from clinical studies. No recognized prospective trials have evaluated trastuzumab in MBC patients with brain metastases. 111 Retrospective investigations have shown that patients with HER2-positive disease who received trastuzumab treatment experienced a longer time to develop CNS metastases and improved survival compared with those who did not receive the medication. 112 The management of systemic extracranial disease demonstrated that trastuzumab enhanced the prognosis of CNS metastases. 113
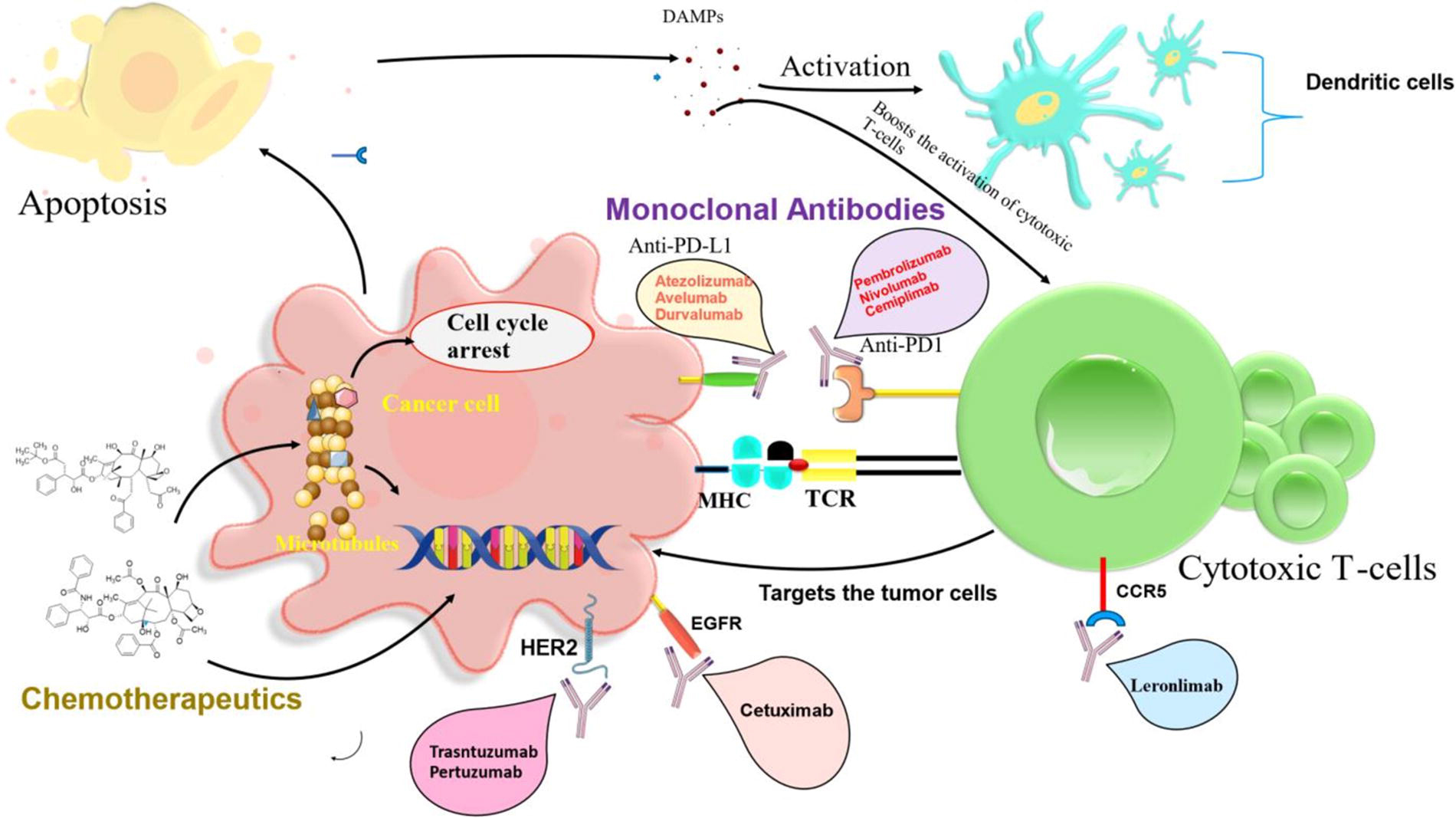
Various classes of drugs used alone or in combination in breast cancers.
Immune efficacy
A 185-kDa transmembrane tyrosine kinase protein called HER2 (Her-2/neu, c-erbB-2) increases the aggressiveness of breast tumors (BCs). 114 Of the initial breast tumors in humans, 15%–20% overexpress HER2, which is linked to decreased disease-free and overall survival (DFS) rates. For all phases of HER2-positive BC, trastuzumab combined with chemotherapy is an effective treatment. 115 Other anti-HER2 mAbs have been effective in treating patients with HER2-positive tumors, either alone or in conjunction with trastuzumab. 93
In the integrated system of antitumor host defense, several cells and molecules work collaboratively, including innate and adaptive immune responses. 116 Innate immunity refers to the capacity of natural killer (NK) cells, monocytes, and neutrophils to recognize and eliminate tumor cells independent of antigens. 117 T and B lymphocytes that are specific for BC antigens, such as HER2, may be able to recognize and eliminate tumor cells. Evasion of innate and adaptive immunity is considered crucial for the progression and propagation of BC. 118 The anticancer effects of mAbs may also be significantly influenced by innate and adaptive immunity, according to mounting evidence. 119
Many human tissues contain hyaluronan, an extracellular glycosaminoglycan, and a variety of solid tumors in humans accumulate hyaluronic acid (HA). To construct a complex network inside the extracellular matrix, HA noncovalently associates with the N-terminal globular domains of proteoglycans such as aggrecan or versican, along with additional hyaladherins or hyalectans. 120 The buildup of HA in tumors is linked to malignancy and indicates a more aggressive form of the disease. 121 Compression of blood vessels, an increase in interstitial fluid pressure, and impaired perfusion are all effects of elevated HA levels in tumors, sometimes in conjunction with collagen. 122 In preclinical animal models, the removal of HA from solid tumors characterized by high-HA tumor microenvironments (TMEs) mitigates these physiological effects, resulting in tumor vasculature reperfusion, enhanced accumulation of chemotherapeutic agents, and suppression of tumor growth. 123 Malignant cells may also be protected from immune cell monitoring by the pericellular matrix with high HA content. The tumor stromal compartment’s pro-tumorigenic effect is further enhanced by its high HA concentration. 124
Targeted mAb
Targeted mAb therapies have lately achieved significant advancements in response and survival rates with less toxicity, solidifying mAbs as an integral element of the anticancer toolbox. 125 BC, gastric cancer, colon cancer, and more solid tumors are sanctioned indications for the anticancer agents trastuzumab (p185HER2) and cetuximab Epidermal Growth Factor Receptor (EGFR). 126 When HER2 or EGFR expression is increased in human malignancies, trastuzumab or cetuximab, respectively, limits tumor growth. Cetuximab and trastuzumab have had positive clinical results. 127 Previous descriptions of these mAb resistance mechanisms include a wide range of topics. Recently, the tumor Extracellular Matrix (ECM’s) possible contribution to treatment resistance has come to light. 128 Antibody-dependent cell-mediated cytotoxicity (ADCC) is a mechanism of efficacy for mAb therapies (Fig. 3). 129 While the therapeutic antibody binds to antigens on the tumor cell surface, the Fc region of the antibody is recognized by the immune cell surface FcIIIA (CD16) receptor. 130 And the target tumor cell is subsequently eliminated by immune cells, particularly NK cells. 131 ADCC plays a vital effector role in mAb-based therapy by directly eliminating target tumor cells, which may lead to tumor antigen presentation and the activation of tumor antigen-specific T cell responses. 132
Safety and tolerability of mAbs in BC
Safety
Highly targeted medicines with less toxicity include mAbs. mAbs not only cause the immediate killing of cancer cells but also immune activation and tumor cell toxicity. 133 mAbs have drawbacks, including their size, which may make it difficult for them to penetrate tumors, the expression of heterogeneous antigens, and the production of tumor antigens in normal cells. 134 There are numerous anti-HER mAbs being developed to treat various malignancies. 135
In 1975, Köhler and Milstein published their fundamental work on the generation of mouse mAbs utilizing the hybridoma approach (Fig. 2). 136 Since then, technological developments have enabled the transition from mouse to humanized and fully human mAbs, with fewer potentially immunogenic animal components. As a result, mAbs have achieved significant clinical success. 137
Since the United States Food and Drug Administration (USFDA) approved the first mAb in 1986, more than 30 years have passed, and antibody engineering has undergone significant change. 138 Because of their excellent specificity, current antibody medications have fewer and fewer side effects. Therapeutic antibodies have thus emerged as the most common type of novel medications created in recent years. 139 The USFDA has approved 79 therapeutic mAbs, including 30 mAbs for the treatment of cancer, out of 570 therapeutic mAbs that have been investigated in clinical trials, according to 2019 statistics. 140 The USFDA has approved 150 mAbs to date, with 151 undergoing clinical testing (Table 2). 141
FDA Approved Monoclonal Antibodies (2020–24)
Murine mAbs, chimeric mAbs (where murine variable [V] regions are grafted onto human constant [C regions]), humanized mAbs, which consist of a human Ig scaffold with only the complementarity-determining regions (CDRs) of murine origin, and, most recently, fully human mAbs have all undergone progressive development. 142 The CDRs of a mAb attach to specific targets, resulting in signals or antagonistic behavior. The Fc region of a mAb is made up of the hinge and constant heavy-chain domains (CH2 and CH3), which also perform other functions such as complement fixation and binding to Fc receptors. 143 The way mAbs are named reflects the type of mAb; for example, the ‘xi’ in rituximab indicates that it is a chimeric mAb. 144
Tolerability
The cardiac tolerability of trastuzumab is relevant as HER2 is overexpressed or amplified in 20%–25% of breast tumors, which correlates with a poor prognosis and reduced overall survival. 145 Trastuzumab is a humanized mAb derived from recombinant DNA that specifically binds to the extracellular region of the HER2 protein. 146 Trastuzumab was later sanctioned for monotherapy in patients with HER2 overexpressing MBC who have received one or more chemotherapy regimens and in conjunction with paclitaxel for those who have not undergone any chemotherapy for metastatic disease. 147 In this study, the response rate was 50% for the trastuzumab plus chemotherapy group, compared with 32% for the chemotherapy-only group, demonstrating enhanced response rates and an increase in survival to 25.1 months for the trastuzumab plus chemotherapy cohort, versus 20.3 months for the chemotherapy cohort alone. Despite notable differences, the cardiac dysfunction induced by trastuzumab exhibits clinically similar characteristics to that caused by anthracycline chemotherapy. 148
Combination therapy with mAbs in BC
The use of mAbs in oncology has become more important and highly beneficial in the BC treatment. The combination therapy of mAbs is highly suitable because of limited overlapping toxicity and lack of pharmacokinetic interactions. By the combination therapy of mAbs, different pathways can be targeted and, thus, exhibits leading additive or synergistic effects. 71
Combination of TRA-8 with adriamycin or paclitaxel for TRA-8 sensitive BC
The anti-DR5 mAb Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand 8 (TRA-8) binds to the human death receptor DR5 and has efficacy against BC tumors. 170 In TRA-8 sensitive BC cell lines, the combination of TRA-8 with chemotherapeutic agents such as adriamycin (an anthracycline) or paclitaxel (a taxane) yields a superior antitumor impact compared with either agent administered independently. 171 In certain cell lines, the therapeutic effect will be additive, whereas in others, it will be synergistic. 172
Trastuzumab in combination with other antitumor medications for HER2-positive BC
Trastuzumab, a mAb to herceptin, specifically targets the HER2 gene and promotes cell death via ADCC. This medicine exhibits a synergistic impact when administered in conjunction with other antitumor agents such as nimotuzumab, carboplatin, 4-hydroxycyclophosphamide, docetaxel, and vinorelbine. 173 The combination of trastuzumab and chemotherapy for one year will enhance the patient’s survival outlook. 174 In the treatment of HER2-positive MBC, the combination of trastuzumab and docetaxel demonstrated superior efficacy compared with docetaxel monotherapy. 175 In MBC, the combination of trastuzumab and chemotherapy exhibits a superior objective response rate and a reduced rate of disease progression. 176 Adverse consequences of trastuzumab-based therapy encompass congestive heart failure and a decrease in left ventricular ejection fraction. 177
Pertuzumab–Trastuzumab–Docetaxel combination for HER2+ BC
The amalgamation of pertuzumab, trastuzumab, and docetaxel is sanctioned for the management of HER2-positive breast carcinoma. 178 HER+ tumors exhibited significantly elevated rates of pathological complete response (pCR) and invasive disease-free survival compared with HER- tumors. The adverse effects of this medication are febrile neutropenia and diarrhea. 179
Rational combination therapy
The clinical benefit of antibodies is maximized when they are rationally combined with other anticancer medications and substances that target the immunosuppressive TME. 180
Combination of immune checkpoint blockade (Pembrolizumab) with Trastuzumab for HER2+ BC
Immune checkpoint blockade (ICB) antibody inhibitors have a significant impact on the treatment of BC. Combining trastuzumab with ICB helps overcome the resistance to trastuzumab monotherapy. 181 Trastuzumab and pembrolizumab, the ICB, exhibit a synergistic effect that results in excellent results in HER2+. 182
Combination of trastuzumab with lapatinib for HER2+ BC
Lapatinib is a kinase inhibitor that inhibits the activity of HER1 and HER2 tyrosine kinases, as well as cell proliferation. 183 Lapatinib and trastuzumab together appear to promote immune-mediated trastuzumab-dependent cytotoxicity. 184
AC regimen for HER2+ and node+ BC treatment
Node-positive, HER2+ BC patients are being randomly assigned under the National Surgical Adjuvant Breast and Bowel Project-B31 protocol to either four cycles of AC (adriamycin and cyclophosphamide) followed by four cycles of paclitaxel or the same regimen plus trastuzumab in combination with paclitaxel. Trastuzumab is also given either concurrently with paclitaxel therapy or following the conclusion of AC and paclitaxel therapy. 185
Combination of trastuzumab with cyclin-dependent kinase inhibitor (flavopiridol) for HER2+ BC
Trastuzumab and the cyclin dependent kinase inhibitor flavopiridol work synergistically to prevent the survival of BC cells that overexpress the HER2 gene. 186
Combination of bevacizumab with vinorelbine for refractory MBC
In phase II clinical studies, vinorelbine and bevacizumab were used to treat patients with resistant MBC. 187
Combination of bevacizumab with capecitabine
In the bevacizumab phase III clinical study for BC, patients with metastatic disease who had previously received treatment were randomly assigned to receive either capecitabine alone or capecitabine + bevacizumab as part of their treatment. 188 The major end point of the study, the ORR, improved significantly when bevacizumab was added to capecitabine (19.8% versus 9.1%), although there was no difference in progression-free survival. 189
Resistance to mAbs
Although mAb therapy has proven effective in cancer treatment, clinical resistance to these agents continues to pose a substantial challenge. 134 The majority of individuals exhibit refractory disease within one year, with just a minor proportion of patients responding to treatment. Therapeutic resistance may be categorized as innate (primary) or acquired (secondary), with diverse mechanisms contingent upon the context. 190
Innate resistance
Innate resistance primarily arises from alterations that exist in tumor cells before treatment. 191
Acquired resistance
Acquired resistance results from immune selection pressure and immunoediting of the tumor during treatment. 192 Preclinical models and clinical trials utilizing mAb treatment have revealed the induction of alternative growth signaling pathways, epithelial–mesenchymal transition (EMT), inadequate effector cell responses, mutations in the antibody target, and various other resistance mechanisms. 193 The efficacy of mAb therapy is limited by the expression of target molecules on tumor cells that the antibodies may attach to. 73 Although mutations in the CD20 gene can confer irreversible resistance to rituximab in lymphoma patients, such alterations were rarely observed at the onset of treatment. 194 HER2 expression remained unchanged in BC patients treated with trastuzumab, despite conflicting results from in vitro studies. 195 It is shown that Signal Transducer and Activator of Transcription 1 (STAT1)-mediated pathways can lead to the downregulation of HER2 upon exposure to IFN-γ. 196 Moreover, trastuzumab-induced ADCC triggers the release of IFN from NK cells, subsequently leading to the downregulation of HER2 expression in a STAT1-dependent manner, so resulting in concomitant resistance to trastuzumab. 197 PD-L1 is recognized to be increased on the surface of tumor cells due to the activation of IFN-induced STAT1 signaling, which confers resistance to NK cell-mediated ADCC. 198 Primary resistance to trastuzumab in BC is linked to genetic features associated with EMT. 199 A subset of patients undergoing extended trastuzumab therapy for HER2 positive/PTEN negative breast tumors exhibited EMT, which facilitated acquired resistance. 200 Mutations in the antibody target and associated downstream signaling molecules may induce acquired resistance to mAb therapy by activating alternative growth or survival signaling pathways. 201
The absence of MHC Class I Polypeptide-Related Sequence A (MICA) and other ligands for the Natural Killer Group 2 Member A (NKG2A)-Human Leukocyte Antigen (HLA)-E axis in cancer cells, which stimulate NK cells, can inhibit NK cells from initiating ADCC. 202 The downregulation of many cell surface proteins associated with the immunological synapse in reaction to cetuximab and trastuzumab is a recently identified distinct mechanism of ADCC resistance. 203 Clinical resistance often entails less cytotoxic immune effector cell responses, with antibody-dependent cell-mediated cytotoxicity (ADCC) regarded as the principal therapeutic mechanism of mAb treatment. 132 Capuano et al. elucidated a distinctive mechanism of immunological weariness, demonstrating that CD16 ligation resulted in NK cells, continuously exposed to rituximab, losing their cytotoxic capabilities. 204 Checkpoints on NK cells can regulate ADCC as well. The blockade of these receptors enhanced trastuzumab-based responses in BC patients. 205 Poliovirus receptor-like receptors, including TIGIT, are recognized for their role in trastuzumab-mediated ADCC of cancer cells by NK cells. 197
The synthesis of several proteins essential for the immunological synapse is also required for NK cell-mediated ADCC. While this may seem less critical for trastuzumab-mediated ADCC, ADCC is somewhat reliant on recognition via Intercellular Adhesion Molecule 1 (ICAM-1) and CD18. 206
Future directions for mAb therapy
The uses and methodologies of mAbs are continually advancing to enhance therapy outcomes for BC patients. These innovative therapeutic methods have markedly enhanced survival rates. 207 The enhancements in survival rates for patients with HER2-positive BC have been facilitated by the advent of HER2-targeted therapies, such as trastuzumab, pertuzumab, and more recently, tucatinib and trastuzumab deruxtecan. 208 Currently, early BC patients undergoing chemotherapy and dual antibody therapy exhibit survival rates of 90%. 209
Notwithstanding this accomplishment, the emergence of mAb resistance has been increasing, mostly contributing to disease progression and suboptimal therapeutic outcomes. 210 Consequently, rigorous research is underway in the preclinical, translational, and clinical domains to develop innovative and more efficacious therapies for HER2, a very sensitive target. 211
ADCs
Targeting HER2 has advanced thanks to the increased use of ADCs, which can now have their linkers, payloads, or antibody scaffolds modified for maximum effectiveness. 212 Several HER2-targeted ADCs of the next generation are presently being tested in clinical studies. 213 To increase the effectiveness and tolerability of these new drugs, several payloads and linker technologies have been used in their design (Fig. 1). 214
A166
Trastuzumab is conjugated with the auristatin derivative duostatin-5 as the payload of A166, an ADC. 212 A phase I trial involving 27 evaluable patients yielded initial efficacy data in 2020, demonstrating a disease control rate of 59% and partial responses in 7 patients (26%) at dose levels of 3.6 mg/kg and 4.8 mg/kg. 213 Current results are pending for this ongoing experiment (NCT03602079). 215
Trastuzumab duocarmazine
The HER2 ADC SYD985, often referred to as vic-trastuzumab duocarmazine, has a trastuzumab backbone connected by a cleavable linker to a duocarmycin payload, a potent DNA alkylating agent, which includes its inactive prodrug form, seco-duocarmycin. 213 Given that the payload in this context is membrane-permeable, it may also infiltrate adjacent cells, regardless of HER2 expression. 216 The HER2-positive and “HER2-low” breast tumors, characterized as HER2 1+ or 2+/ Fluorescence In Situ Hybridization (FISH) nonamplified, demonstrated indications of anticancer efficacy in the phase 1 study of this ADC. 213
Bispecific antibodies
An alternative approach is the development of bispecific antibodies that enhance efficacy by targeting two separate HER2 epitopes. 217
Therapeutic approaches for TNBC
TNBC has gained from immunotherapy, and initiatives to stimulate the immune response in HER2-positive cases are currently in progress. 218 Immunotherapy can be approached through several methods, including checkpoint inhibitors, cellular treatment, vaccines, and the conjugation of effector T cells with HER2 antibodies, among others. 219
Combination of ADC with antitumoral drugs
A novel class of drugs has been developed based on the complementary actions of HER2 inhibition and chemotherapy. 220 ADCs are pharmacological entities that combine the anticancer effects of both of these methods. It has FDA approval. 221
Combination of trastuzumab with lapatinib
The Adjuvant Lapatinib and/or Trastuzumab Treatment Optimization trial is the inaugural study to report in 2014 on the efficacy of dual anti-HER2 therapy with trastuzumab and lapatinib (either sequentially or concurrently) versus trastuzumab monotherapy. 222 Patients with HER2-positive primary BC participating in the APHINITY trial are receiving pertuzumab alongside trastuzumab and standard nonanthracycline chemotherapy. 223 The KATHERINE study examines the effects of postoperative T-DM1 compared with trastuzumab in patients with HER2-positive disease who exhibit less than a pCR following preoperative therapy with a trastuzumab-based regimen. 224
Combination of trastuzumab with ZD1839
A phase II trial by the Eastern Cooperative Oncology Group is administering a combination of ZD1839 and trastuzumab to patients with MBC exhibiting HER-2 overexpression. 225 By inhibiting HER-2 transactivation, EGFR inhibition may enhance trastuzumab response rates. In trastuzumab-resistant tumors, where compensatory signaling by EGFR may hinder the response to trastuzumab, such a combination may also be considered. 226
Obesity-associated BC
Humanized monoclonal antibody–blocking fatty acid binding protein 4 (FABP4) activity (PMID: 39054536): The risk of BC is increased by obesity, although the underlying molecular pathways are unclear. Adipose FABP (A-FABP, or FABP4) may provide a new target for the therapy of BC by establishing a connection between the risk of BC and obesity-induced dysregulated lipid metabolism. 227 A study used screened hybridoma clones with specific binding to FABP4, and immunized FABP4 knockout mice with recombinant human FABP4 revealed the creation of humanized mAbs that inhibit FABP4 activity in mice models to treat BC. One clone, 12G2, was chosen for additional analysis because it dramatically decreased the levels of FABP4 in the blood and stopped the growth of breast tumors. Sixteen humanized 12G2 mAb variants were created by grafting its CDRs to specific human germline sequences following confirmation of the therapeutic efficacy of the chimeric 12G2 mAb, which consists of mouse variable regions and human IgG1 constant regions. The humanized V9 mAb consistently inhibited the growth and spread of breast tumors by altering the mitochondrial metabolism of tumor cells. 228
Trastuzumab: Obese women had a lower DFS (HR 1.31, 95% Confidence Interval (CI) 1.07–1.59) than women of normal weight in a secondary analysis of the N9831 trial, which compared chemotherapy with or without trastuzumab in nearly 3400 women with HER2-positive, early-stage BC. 229 Although the trial was not sufficiently powered to detect a statistically significant difference based on the treatment received, this investigation indicates that IV adjuvant trastuzumab may improve clinical outcomes independent of Body Mass Index (BMI). 230
Sacituzumab govitecan-hziy: It is authorized for use in patients with Hazard Ratio (HR)-positive, HER2-negative, triple-negative, or resistant MBC. 231 Pharmacokinetic studies that demonstrate a correlation between body weight and the amount of drug distribution and clearance have led to weight-based dosing. 232 To the best of our knowledge, no research has evaluated how BMI affects sacituzumab govitecan-hziy’s toxicities and clinical results in BC patients. 233
Pembrolizumab: Subsequent pharmacokinetic studies demonstrate that a fixed-dosing method results in no clinically meaningful differences in efficacy and safety, confirming the current FDA recommendation of a fixed dose, even though early clinical trials of pembrolizumab used a weight-based dosing technique. 234 There is a dearth of information on how obesity affects immunotherapy clinical results. 235 In addition, this work raises the possibility that immunotherapy may produce a potent antitumor immune response in obese BC patients, which calls for additional validation through carefully planned clinical studies. 236
Numerous scientific studies, however, have shown that to increase the overall survival rate and quality of life of BC survivors who are obese, we must use various complementing strategies. 237 Therefore, in addition to the standard therapeutic management, it is imperative to use complementary nutritional interventions as adjuvant therapy to reduce obesity and its associated consequences with regard to the prevalence of BC. 238
Conclusion
mAbs are multitaskers that suppress checkpoints, to put it briefly. They were heavily utilized in research applications. These mAbs treat tumors and lessen the harmful side effects of chemotherapy. 239 They also treat autoimmune, cardiovascular, cancer, and inflammatory illnesses. They respond to immune system-targeted, minimally harmful treatment. They might have widespread negative impacts. 240 Cardiovascular patients can tolerate mAbs for BC. For the greatest clinical benefit, these mAbs are combined with other anticancer medications. 11
Footnotes
Acknowledgments
The authors are thankful to the School of Pharmaceutical Education and Research, Jamia Hamdard, and St. Pauls College of Pharmacy, Telangana, for encouragement and support.
Authors’ Contributions
R.S., V.M., S.B., and A.R. contributed to study conception, data collection, and article preparation. B.M., V.S.H., R.K., B.S., and S.T. designed, reviewed the results, and approved the final version of the article.
Ethical Approval
Not required.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
Authors received no funding for this research.