
Abstract
Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) is becoming increasingly common worldwide. The purpose of this study was to identify the prevalence and molecular characteristics of MRSA bloodstream isolates in hospitals. Clinical data from patients with MRSA bacteremia between 2003 and 2005 were collected. Isolates were classified as hospital-acquired (HA-MRSA), health care-associated (HCA-MRSA), or CA-MRSA according to the time of isolation and the risk factors for colonization. Available strains were tested for the presence of mecA, staphylococcal cassette chromosome mec (SCCmec), and by multilocus sequence test. Among 129 cases, 78 nonduplicated isolates were analyzed. The proportion of CA-MRSA, HCA-MRSA, and HA-MRSA was 2.6% (2), 23.1% (18), and 74.4% (58), respectively. According to multilocus sequence test and SCCmec, there were seven genotypes with sequence types (STs) and SCCmec types. The predominant genotype, ST5-MRSA-II, was found in 57.7% (45). All type IVA isolates was ST72 (9), and ST72-MRSA-IVA was identified in CA-MRSA (2, 100%), HCA-MRSA (1, 5.6%), and HA-MRSA (6, 10.3%), respectively. In summary, CA-MRSA bacteremia was not common in our hospital during the period.
Introduction
Recently, MRSA has been increasingly isolated from community-acquired infections as well as hospital-acquired infections. Community-acquired MRSA (CA-MRSA) has historically been found in persons with known risk factors for colonization, but more recent cases also involve colonization and transmission in persons without risk factors. 10 For clarity, MRSA infection in patients with recent exposure to a health care setting or other known risk factors at the time of admission should be termed health care-associated MRSA (HCA-MRSA) infection, instead of using the term CA-MRSA. 32
A large prospective population-based study of MRSA infections found that CA-MRSA infections are more likely to occur in younger individuals and in individuals from minority ethnic groups or of low socioeconomic status, whereas risk factors for HA-MRSA infection include older age, immunosuppression, dialysis, recent surgery, and use of invasive devices. 23 Recent use of antimicrobial agents is also a risk factor for both CA- and HA-MRSA infections. 23 Skin and soft tissue infections account for 75% of CA-MRSA infections, but they account for only 37% of HCA-MRSA infections. 23
The mecA gene, responsible for methicillin resistance in S. aureus, is carried on a mobile genetic element termed staphylococcal cassette chromosome mec (SCCmec). A genetic lineage of MRSA with SCCmec type IV is frequently found in CA-MRSA infections. SCCmec type IV is smaller, thus, potentially more mobile, and less likely to carry other antimicrobial resistance genes than SCCmec types I and II, which are typically found in HA-MRSA strains.1,10,20,25,30 Further, Panton-Valentine leukocidin (PVL) is rare among HCA-MRSA strains, but it is commonly present in CA-MRSA strains.
Regardless of the origins, the emergence of MRSA within the community is a major threat with several important clinical implications. Treatment failure with accompanying complications or death may result if an antistaphylococcal β-lactam antibiotic is used and the infecting strain proves to be resistant. Infections caused by methicillin-resistant strains may be more difficult to manage or more expensive to treat, perhaps because vancomycin is inherently less efficacious in such cases.4,31
Knowing the specific epidemiological pattern of isolates at an individual hospital is important for the management of clinical diseases. Despite the high prevalence of MRSA infections at tertiary hospitals in Korea, there have been only a few reports describing CA-MRSA infection and the molecular epidemiology of MRSA isolates.3,5,16,17,28 The purpose of this study was to identify the prevalence and molecular characteristics of MRSA isolates in our hospital. We also attempted to correlate molecular characteristics and antibiotic resistance patterns.
Materials and Methods
This study was conducted at Kyung Hee University Medical Center, an 850-bed, tertiary referral center serving primary care, emergency, and hospitalization needs in Seoul, Korea. A single representative isolate from each patient who had MRSA (recovered from one or more blood cultures) between January 1, 2003 and December 31, 2005 was included in the study. Demographic, clinical, and microbiological data were retrospectively collected by reviewing medical records. Patients with polymicrobial infections with other bacteria and clinically insignificant bacteremia based on the criteria of systemic inflammatory response syndrome (SIRS) 2 were excluded.
Definition
Isolates were classified as community-acquired, health care-associated, or hospital-associated according to the modified criteria of Naimi et al. 23 Isolates were considered to be HA-MRSA if they had no evidence of infection at presentation, and the first blood specimen positive for MRSA was collected more than 48 hours after admission. Isolates were considered to be HCA-MRSA if the case met one of the following criteria: isolation of MRSA within 48 hours after admission with a history of hospitalization, surgery, dialysis, or residence in a long-term care facility within 1 year of the MRSA culture date, a permanent indwelling catheter or percutaneous medical device (e.g., tracheostomy tube, gastrostomy tube, or Foley catheter) present at the time of culture, or a known positive MRSA culture before the study period. Isolates that did not meet any of above health care-associated features were classified as CA-MRSA. CA-MRSA infections within 48 hours after admission were defined as no underlying medical conditions if the patient had no documented chronic underlying condition and did not qualify for the health care-associated category.
Characterization and antimicrobial susceptibility of isolates
MRSA isolates were tested for phenotypic resistance to oxacillin by the salt agar dilution method, according to the guidelines of the Clinical Laboratory Standards Institute. 6 In vitro susceptibility tests were performed by a broth microdilution test as described by Clinical Laboratory Standards Institute guidelines. The antimicrobial agents tested were oxacillin, penicillin, amoxicillin-clavulanic acid, cefazolin, clindamycin, erythromycin, tetracycline, rifampin, ciprofloxacin, trimethoprim-sulfamethoxazole, teicoplanin, and vancomycin.
Molecular characterization
All available strains were tested for the presence of mecA, ccr gene complex, and SCCmec by polymerase chain reaction (PCR), multilocus sequence tests (MLSTs), and pulsed-field gel electrophoresis (PFGE). Presumptive assignment of SCCmec types was by multiplex PCR strategy described by Milheiriço et al. 21 Conventional ccr gene PCR typing was performed as described by Okuma et al. 24 Chromosomal DNA for MLST and multiplex PCR for SCCmec typing were extracted with the G-spin genomic DNA extraction kit (iNtRon Biotechnology). Multiplex PCRs were carried out with Premix taq (Ex taq) for MLST and the Maxime PCR Premixe kit (i-StarTaq; iNtRon Biotechnology) for SCCmec and PVL. MRSA genotypes were defined based on sequence type (ST) and SCCmec type as proposed by Robinson and Enright. 29 The PVL gene was screened by the PCR method of Lina et al. 19
MLST was performed as previously described. 8 Allele number and ST were determined with the use of a database at the MLST website (http://saureus.mlst.net/). Clustering of related STs, which were defined as clonal complexes (CCs), was determined using the program eBURST (based upon related STs). 9
Strain relatedness among all CA-MRSA or SCCmec type IV isolates and a random sample of HA-MRSA isolates was investigated by PFGE with SmaI restriction endonucleases (Roche) as previously described. 12
Statistical analysis
Statistical analysis was performed using the chi-square test or Student's t-test with SPSS version 12.0 software. A p-value < 0.05 was considered statistically significant.
Results
Prevalence of CA-MRSA and HA-MRSA blood isolates
During the period of the study, there were a total of 241 cases of nonduplicated S. aureus bacteremia (total 567 isolates). The proportion of MRSA was 53.5% (129/241). Ninety-seven MRSA blood isolates were monobacterial and clinically significant by the criteria of SIRS. Seventy-eight isolates were available from the stocks of the microbiology laboratory and were analyzed in this study. Fifty-eight isolates (74.4%) were classified as HA-MRSA, 18 (23.1%) as HCA-MRSA, and only 2 (2.6%) met the strict criteria for CA-MRSA (Table 1).
CA-MRSA, community acquired methicillin resistant Staphylococcus aureus; HCA-MRSA, health care-associated MRSA; HA-MRSA, hospital-acquired MRSA.
Antimicrobial susceptibility
The MIC of oxacillin ranged from 32 to >256 μg/ml. The majority of the isolates tested were resistant to erythromycin (91.0%), ciprofloxacin (87.9%), and gentamicin (83.3%) (Table 2). All isolates were susceptible to vancomycin. Most MRSA strains were multiresistant to more than three classes of antibiotics, whereas CA-MRSA isolates were resistant to only clindamycin or erythromycin, respectively (Table 2).
Molecular characterization
All isolates were tested by MLST and SCCmec typing. We identified seven MRSA genotypes (ST-MRSA-SCCmec type) including their variants based on STs and SCCmec types as proposed by Robinson and Enright 19 (Table 3). Each of these SCCmec types also had one or more subtypes classified by unexpected fragments or the absence of some fragments in multiplex PCR products. 16 The predominant genotype was ST5-MRSA-II, which was found in 45 isolates (57.7%), followed by ST239-MRSA-III (11, 14.1%) and ST72-MRSA-IVA (9, 11.5%). The PVL gene, assumed to be associated with CA-MRSA, was not detected in any of the MRSA isolates in this study.
Assignment of SCCmec types was by multiplex polymerase chain reaction strategy described by Milheiriço et al. 21
SCCmec, staphylococcal cassette chromosome mec; ST, sequence type.
MLST analysis
MLST analysis revealed 5 STs in 78 MRSA isolates (Table 3). The most prevalent type overall was ST5 (51, 65.4%), followed by ST239 (14, 17.9%) and ST72 (9, 11.5%). ST 5 was the most prevalent type in HA-MRSA (38, 65.5%) and HCA-MRSA (12, 66.7%), whereas ST72 was most common in CA-MRSA (9, 100%). eBURST revealed three CCs in 78 isolates. CC5 (ST5) and CC8 (ST72, ST239, and ST254) accounted for 98.7% of isolates. An ST291 isolate was classified as CC813.
SCCmec types
Of the 78 MRSA isolates, the most common SCCmec type was type II, found in 46 isolates (Table 3). SCCmec type II was also the most prevalent in both HCA-MRSA (8, 44.4%) and HA-MRSA (37, 63.8%). All SCCmec type IVA strains were ST72 (9, 100%). ST72-MRSA IVA was identified in two (100%) of CA-MRSA, one (5.6%) of HCA-MRSA, and six (10.3%) of HA-MRSA isolates (Table 4).
Pulsed-field gel electrophoresis
PFGE of ST72-MRSA-IVA isolates revealed three different types. CA-MRSA isolates from 2004 and 2005 showed different types on PFGE. One isolate of CA-MRSA, HCA-MRSA, and HA-MRSA from 2004 and three HA-MRSA isolates from 2005 had the same PFGE pattern and were similar to one HCA-MRSA from 2003 (Fig. 1).
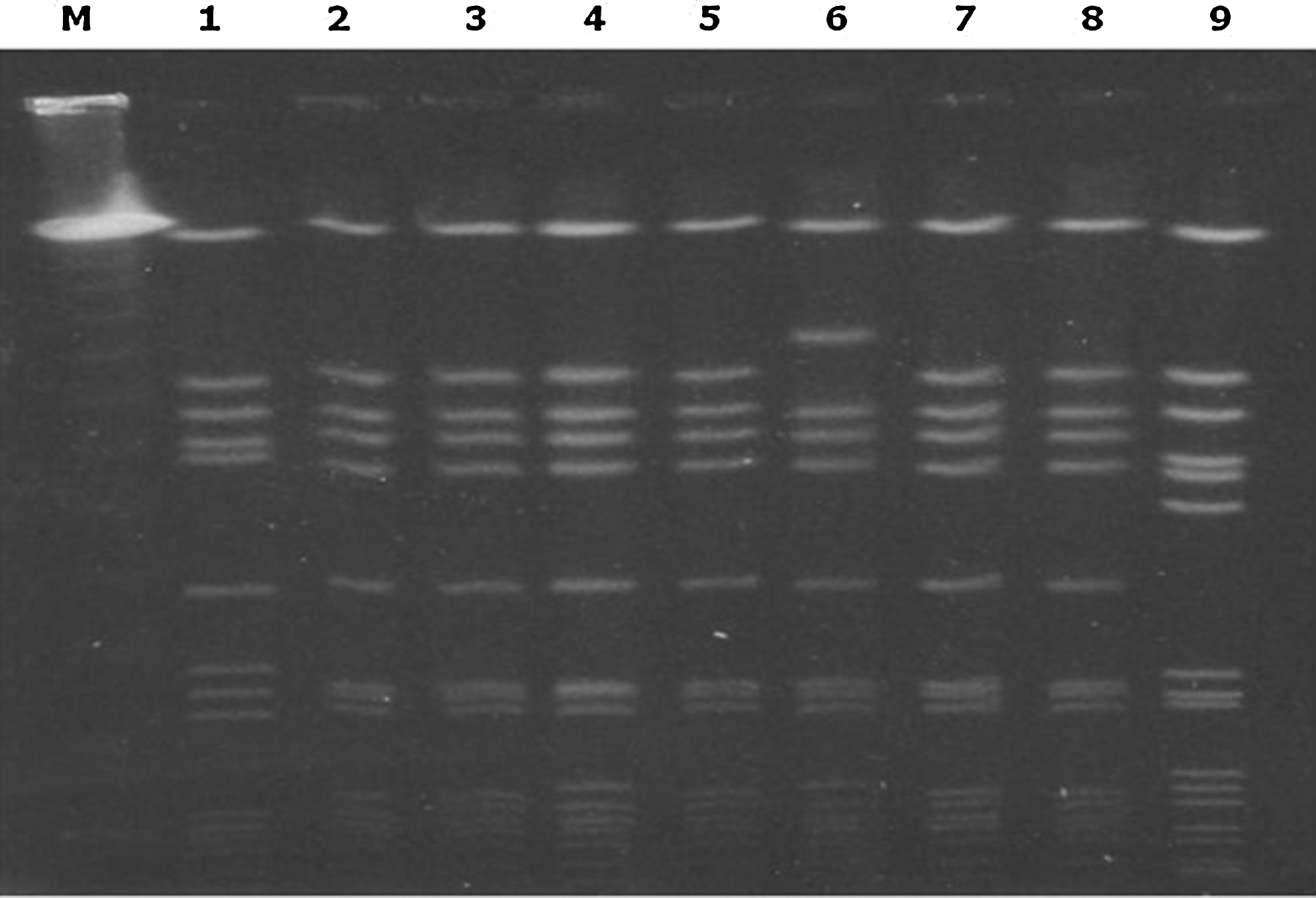
Pulsed-field gel electrophoresis DNA pattern using SmaI for sequence type 72-methicillin resistant Staphylococcus aureus-IVA isolates. Lane M, lambda molecular weight marker; lane 1, HA in 2003; lanes 2–4, HCA, CA, and HA in 2004, respectively; lanes 5–9, HA, CA, HA, HA, and HA in 2005, respectively. CA, community-acquired isolate; HCA, health care-associated isolate; HA, hospital-acquired isolate.
Discussion
The main findings of this study were as follows: (1) True CA-MRSA bacteremia was not common during the study period; (2) the molecular characteristics of HCA-MRSA strains were similar to HA-MRSA; (3) the predominant genotype was ST5-MRSA-II (45, 57.7%), followed by ST239-MRSA-III (11, 14.1%); and (4) SCCmec type IVA was identified in CA-MRSA (2, 100%), HCA-MRSA (1, 5.6%), and HC-MRSA (6, 10.3%).
We included only cases satisfying the SIRS criteria to exclude cases with simple colonization or contamination. Strict criteria were also used to define true CA-MRSA cases without any risk factors. Most episodes of MRSA bacteremia in our hospital were hospital-acquired (77.4%) or health care-associated (23.1%).
MRSA isolates in this study showed a high rate of resistance to erythromycin, ciprofloxacin, and gentamicin and a low rate of resistance to chloramphenicol and rifampin. All of the CA-MRSA strains were resistant to oxacillin/β-lactams. One showed additional resistance to clindamycin and another to erythromycin. HA-MRSA and HCA-MRSA strains were multiresistant to more than three classes of antibiotics. Cha et al. reported that the prevalent ST239 and ST5 clones are highly resistant to antimicrobial agents compared with the susceptibilities of less common MRSA clones. 3 ST239 and ST5 strains in this study were also highly resistant to antimicrobial agents such as ciprofloxacin, erythromycin, gentamicin, and clindamycin. Ko et al. reported that most MRSA strains in Asia are multiresistant to more than three classes of antibiotics, whereas a few strains from Korea are resistant only to β-lactam agents and gentamicin. 18
The molecular epidemiology and antibiotic resistance patterns of HCA-MRSA were similar to those of HA-MRSA. In contrast to HCA- or HA-MRSA strains, CA-MRSA strains were susceptible to a variety of non-β-lactam antibiotics. The PVL gene is commonly present in CA-MRSA strains, but it was not detected in any of the MRSA isolates in this study. This finding is consistent with other studies of MRSA in Korea.5,28
As documented in previous studies,3,4,17 ST5-MRSA-II and ST239-MRSA-III were the most prevalent genotypes among MRSA isolates in Korea. ST239-MRSA-III and its variants were also common in HCA- and HA-MRSA isolates. ST239-MRSA-III and its variant isolates obtained after 2003 may have been recently introduced into Korean hospitals. Different clones of MRSA are prevalent in different hospitals in Korea, as shown by Cha et al. 3
It is common practice to define MRSA clones by the combination of SCCmec type and the chromosomal background as defined by MLST. 21 However, many types, subtypes, and variants of SCCmec elements have been reported without following any standardized, internationally agreed rules of nomenclature. 14 There are ambiguities and inconsistencies in the classification of SCC elements in the published literature to date. To address the issues, the International Working Group on the Classification of Staphylococcal Cassette Chromosome Elements (IWG-SCC) recently proposed guidelines for the classification of SCCmec and other SCC elements. 14 In this study, presumptive assignment of SCCmec types was by multiplex PCR previously described. Next, we determined SCCmec types by ccr gene complex as described in the IWG-SCC. 14 The results of presumptive SCCmec types are mostly similar to the SCCmec type by the classification of IWG-SCC. However, the variants described in this study need further characterization to be globally accepted, according to the recently published guidelines of the IWG-SCC.
In this study, SCCmec type IVA was found not only in CA-MRSA strains but also in HCA- and HA-MRSA strains. Although the number of isolates was too small to accurately evaluate statistical significance, CA-MRSA isolates with SCCmec type IVA showed an increase in annual numbers in the hospital environment, as there were only four isolates in 2005. These results suggests that SCCmec type IVA is not a marker for CA-MRSA and that SCCmec type IVA MRSA has clonally spread between the community and hospital. In contrast to previous Korean and US studies showing that ST5 and ST7 are common in SCCmec type IV or IVA, all SCCmec type IVA strains in this study were ST72. Okuma et al. 24 found that CA-MRSA strains containing SCCmec type IV replicate more rapidly than traditional HA-MRSA strains and argued that CA-MRSA may have enhanced ecologic fitness compared with SCCmec type II or III strains. It is unclear how infections with strains containing SCCmec type IV or IVA differ in symptoms and severity from those caused by traditional HA-MRSA strains. 24
Our study has some limitations. First, it was a retrospective study. Second, only patients with bacteremia were enrolled and the number of patients was small. Traditionally, CA-MRSA infections are common in skin and soft tissue or ear infections, so the included cases may not represent CA-MRSA seen at our hospital. We selected blood stream infections, as they are clinically significant and potentially useful for defining the epidemiology of invasive MRSA infections. Third, the data were from only one institute and may, therefore, not reflect local trends. The definition of CA-MRSA used in this study was different from that used in other Korean CA-MRSA-related studies. Using the CDC definition of community-acquired infection (1988) increased the number of CA-MRSA strains in this study to 20 (25.6%). These days, the definition of community-associated infection has changed, particularly in patients with complicated conditions such as malignancy or renal failure. These patients regularly visit outpatient departments and receive care at hospitals, yet they are categorized as harboring community-associated infections. Recent studies have proposed the term “health care-associated infection” for infections in such patients.11,22 We used a modified version of Chaves' criteria for comparison of our results with previously documented studies on the prevalence or molecular characteristics of MRSA in Korea that used the CDC definition (1988). Most of the cases with CA-MRSA infection had known risk factors for MRSA infections, so they might reasonably be reclassified as HCA-MRSA infections.
Footnotes
Acknowledgments
Disclosure Statement
No competing financial interests exist.