
Abstract
Abstract
This study describes the clinical and molecular characteristics of methicillin-resistant Staphylococcus aureus (MRSA) isolates that emerged after an index case in a tertiary-care oncology hospital in Mexico City and identifies whether these isolates were related with the index case. All MRSA strains isolated from January 2006 until December 2007 were included. The clinical and demographic characteristics of patients were analyzed; molecular typing by pulsed-field gel electrophoresis was used to characterize the isolates. We included 44 MRSA isolates from 55 patients. Thirty-eight patients (86.4%) were classified with nosocomial infection and the remainder with healthcare-related infection. A single pulsed-field gel electrophoresis pattern (C) was identified with minor variations (two subtypes). The isolates analyzed were staphylococcal chromosome cassette mec type II (related with the New York-Japan strain). This case underscores the need to intensify strategies that identify and limit the spread of multiresistant pathogens imported by infected patients referred from other healthcare centers.
Introduction
Methicillin-resistant S. aureus (MRSA) is a worldwide problem associated with increased morbidity and mortality among hospitalized patients; therefore, identification of the risk factors influencing its spread in hospitals is of great concern for the prevention of nosocomial infections. 8 The major reservoirs of staphylococci in hospitals are colonization of patients and healthcare workers (HCW), as well as infected patients. Carriers have a higher risk for developing endogenous infection or transmitting infection to HCW and patients. Transient hand carriage of the organism, usually by HCW, account for the major mechanism for transmission. 9
Patients with cancer are placed at a high risk of developing severe infections with Gram-positive organisms including MRSA because of the frequent use of invasive devices, extensive surgeries, antineoplastic therapy, and immunosuppression associated with malignant disease.5,17
Multiple DNA-based methods have been employed to characterize isolates of MRSA that allow better discriminatory power than phenotypic analyses. 23 These studies have demonstrated the clonal spread of epidemic MRSA strains within hospitals, between hospitals within a country, and even between countries and continents.9,10,12 In Mexico, the prevalence of MRSA varies widely, ranging from 7% to 30%.2,4
MRSA was first isolated in July 2004; subsequently, it was isolated sporadically. In January 2006, an outbreak was identified; the index case was a female patient with osteosarcoma with an exposed prosthesis infection who experienced continuous secretion through the wound and a hospital stay of 38 days over four different time periods. The case was resolved finally with limb amputation during the patient's last hospitalization in March 2006. Since January 2006, the month of the patient's arrival at the hospital, MRSA was continuously isolated from different patients with nosocomial infection or healthcare-related infection (HCRI).
The purpose of the present study was to describe the clinical and molecular characteristics of MRSA isolates that emerged after the index case and to identify whether these isolates were related with the index case.
Materials and Methods
Hospital setting
The Instituto Nacional de Cancerología (INCan) is a tertiary-care oncology center, located in Mexico City; it has 150 beds and a 6-bed intensive care unit. The hospital has 7,500 discharges and 3,450 surgeries per year; 700 patients with long indwelling central venous catheters are continuously cared as outpatients—ambulatory patients followed by the IV team monthly, and 24,000 outpatient visits are performed for chemotherapy-IV-infusion per year. The microbiology laboratory receives on average 14,000 samples annually. The hospital has a Nosocomial Surveillance Program in operation since 1987.
Clinical data
The medical and laboratory records of patients with a clinical isolate of MRSA during January 2006 to December 2007 were retrospectively reviewed. Only one isolate per case of infection was included. Data were collected on demographic characteristics, underlying diseases, length of hospitalization, infection sites and complications, date of MRSA isolation, type of specimen, susceptibility pattern, other bacteria recovered from the same sample, antimicrobial treatment, type and date of surgeries, use of central venous catheter, and date of insertion. After MRSA isolation, we analyzed the outcome (alive, death, or lost to follow-up) and antimicrobial therapy for MRSA infection (type and dose of antibiotics). Survival or follow-up time was calculated from date of MRSA isolation to death, or to the date when the infection was resolved. We considered antimicrobial therapy to be appropriate if the antimicrobial agent prescribed showed clear inhibitory in vitro activity against the clinical isolate.
We screened for nasopharyngeal carriage of MRSA from staff surgeons, medical and surgical residents, and nurses.
Antimicrobial susceptibility testing
All MRSA isolates were identified by standard microbiological procedures. 15 Detection of methicillin resistance was carried out according to the Clinical and Laboratory Standards Institute guidelines using oxacillin disk test. 7 Antimicrobial susceptibility testing was performed by the automated MicroScan method (Dade-Behring, Sacramento, CA) for penicillin, oxacillin, amikacin, amoxicillin, cefotaxime, cephalothin, cefazolin, imipenem, trimethoprim–sulfamethoxazole, erythromycin, clarithromycin, clindamycin, ciprofloxacin, chloramphenicol, gentamicin, rifampin, tetracycline, and vancomycin. S. aureus ATCC 29213 was utilized for quality control as recommended by the Clinical and Laboratory Standards Institute guidelines. 7
Molecular typing
Pulsed-field gel electrophoresis (PFGE) was used to identify MRSA clones. Whole-genomic DNA was prepared as described previously. 6 After digestion with SmaI endonuclease, DNA was separated in a CHEF-DRII apparatus (Bio-Rad, Birmingham, United Kingdom). 6 Strains BK2464, HD288, HU25, and EMRSA16, representing the NY/Japan-USA, Pediatric-Portugal, Brazilian, and EMRSA-16-United Kingdom clones, respectively, were included in PFGE gels for comparison. These strains were kindly provided by Prof. Herminia de Lencastre from the Molecular Genetic Laboratory, Instituto de Tecnologia Química e Biologica da Universidade Nova de Lisboa. The criteria of Tenover et al. were used to compare different clones. 22 Staphylococcal chromosome cassette mec (SCCmec) type was determined by a multiplex polymerase chain reaction strategy. Strain BK2464 was used as SCCmec control. 19 Molecular analysis was performed at the Instituto Nacional de Salud Pública in Cuernavaca, Mexico. Detection of mecA gene was performed at the Instituto Nacional de Ciencias Médicas y Nutrición in Mexico City. Computer analysis of the banding patterns obtained by PFGE was conducted with NTSYSpc ver. 2.0.2.11 software (Applied Biostatistics, Setauket, NY) after visual inspection. Each gel included the reference strain S. aureus NCTC 8325 to normalize PFGE profiles. For cluster analyses, Dice coefficients were calculated to compute matrix similarity and were transformed into an agglomerative cluster by the unweighted pair-group method with arithmetic average. 21
Statistical methods
Comparison of categorical variables and percentages between groups was carried out by the Pearson chi-square test or Fisher's exact test, as appropriate. Logistic regression analysis was performed to find the association between variables. A p-value of ≤0.05 was considered statistically significant. Statistical analysis was performed using Epi-Info (ver. 6) and STATA (ver. 9.1) software.
Results
The first case of this outbreak was a 23-year-old female patient with a bone tumor diagnosed in August 2002 at another hospital. The patient experienced a recurrence in March 2005; the tumor was surgically removed and diagnosed as osteosarcoma. In October and November 2005, at the same hospital, a tibial limb excision was performed and a joint prosthesis was placed. Purulent secretion began to drain a few days later and the prosthesis was exposed. The patient received multiple antimicrobial treatments in addition to several surgical debridements. On January 2006, the patient was referred to the INCan hospital, where osteomyelitis and joint prosthesis infection were diagnosed; the culture of the purulent secretion taken at hospital admission yielded MRSA. Vancomycin and amikacin were initiated and limb amputation was performed in March 2006 with complete resolution of the infection.
From January 2006 to December 2007, 64 MRSA clinical isolates were identified from 55 patients. Forty-four strains (80%) were collected and stored at the laboratory of microbiology.
Thirty-eight infections (86.4%) were classified as nosocomial, and the other six (13.6%) were HCRI. Over the study period, the MRSA clinical isolates were recovered from diverse anatomical sites from different patients (Fig. 1).

Date of isolation and type of sample from methicillin-resistant Staphylococcus aureus (MRSA) strains.
Twenty-two patients were men (50%). Thirty-one patients (70.5%) had a hematologic malignancy, 11 (25%) had a solid tumor, and 2 (4.6%) had no neoplastic disease (biliary stenosis of unknown cause and vertebral mycobacterial infection). The most common infections were surgical site infection (29.5%), pneumonia (27.3%), and bacteremia (13.6%). The infection was polymicrobial in 13 patients (29.5%), and the most common coinfectant microorganism was Escherichia coli (n = 7). Thirty-two patients (72.7%) had received antimicrobials during the previous 3 months. Other characteristics are shown in Table 1.
One endocarditis, one nephrostomy infection, one CVC site infection, and one meningitis.
During the previous 3 months.
CVC, central venous catheter; MRSA, methicillin-resistant Staphylococcus aureus; s.d., standard deviation.
Thirty-eight (86.4%) patients were diagnosed with an episode of nosocomial infection, of which 18 (47.4%) received appropriate antimicrobial treatment: 6 of them died, 2 from infection (mean time, 18.5 ± 12 days) and 4 from another cause (55.2 ± 37.6 days) (p = 0.268). Twenty patients (45.5%) did not receive appropriate antimicrobial treatment. Ten of them died, six from infection (mean time, 3.7 ± 2.3 days) and four from another cause (mean time, 47.2 ± 39.4 days) (p = 0.02). Mean survival for patients was 7.4 ± 8.4 days. The remaining patients recovered and were discharged.
There were six patients classified with HCRI; two of these received appropriate treatment and were alive. Four patients did not receive appropriate treatment and died: two from infection and two from another cause. Mean survival time was 51.2 ± 35.9 days (p = 0.004).
We performed 173 nasopharyngeal cultures from staff and found 24 (13.9%) methicillin-susceptible S. aureus and 2 MRSA (1.1%; 1 from a nurse and 1 from a surgical resident). We were able to include only the latter isolate in the molecular analysis. However, the nurse did not receive treatment, and a new nasal culture done at 16 weeks later did not show MRSA. The surgical resident received ciprofloxacin for another cause, and a nasal culture taken at 8 weeks later was negative.
All clinical isolates showed resistance to penicillin, oxacillin, amoxicillin, cefotaxime, cephalothin, cefazolin, clindamycin, imipenem, ciprofloxacin, chloramphenicol, erythromycin, and clarithromycin. No isolate was resistant to rifampin, amikacin, tetracycline, gentamicin, trimethoprim–sulfamethoxazole, or vancomycin.
PFGE analysis identified a single clonal type, designated pattern C, with two subtypes observed (C13 and C31) that differed in up to three band positions. Lanes 1 and 10 represent lambda ladders used as molecular size (MW) markers; lane 2, control strain NCTC 8325; lanes 3 and 4 (1 INCan [index case] and 52 INCan), patterns C; lane 5 (4 INCan), profile C13; lanes 6–9, control strains: BK2464 (New York/Japan-USA clone), HD288 (Pediatric clone), HU25 (Brazilian clone), and EMRSA-16 (United Kingdom clone) (Fig. 2). Clone C showed a high degree of similarity with both the Pediatric clone (89.5%) and New York/Japan clone (80.0%) (Fig. 3). Characterization by SCCmec typing of clone C representatives demonstrated that isolates in this clone were SCCmec type II. Statistical analysis did not detect important demographic or clinical differences in any of the three patients who presented clonal subtypes.
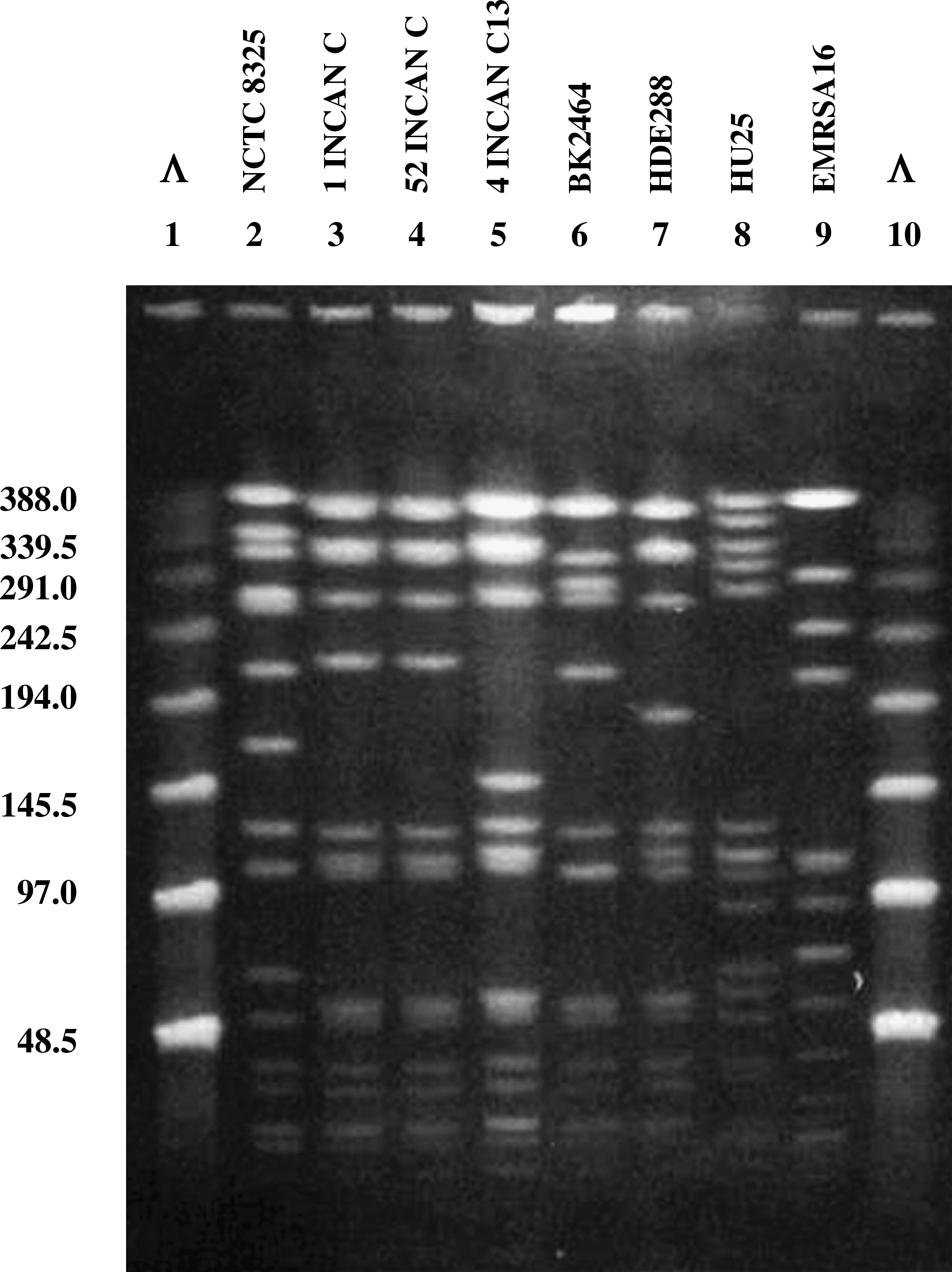
Pulsed-field gel electrophoresis profiles of MRSA clinical isolates from the Instituto Nacional de Cancerología (INCan) and representatives of international MRSA clones.

Dendrogram comparing MRSA clone C from INCan-Mexico with different international MRSA clones. For cluster analyses, Dice coefficients were calculated to compute matrix similarity and transformed into an agglomerative cluster with the unweighted pair-group method with arithmetic average.
Discussion
In this report, we describe the first MRSA outbreak in a tertiary-care oncology hospital in Mexico City. Analysis of MRSA isolates demonstrated that the source of this MRSA outbreak was a transferred female patient with a complicated bone-joint-prosthesis infection, who had been referred from another hospital. Further, all 44 strains characterized showed a multidrug-resistant profile, including β-lactams, cephalosporins, carbapenems, macrolides, quinolones, clindamycin, and chloramphenicol.
We observed an increase in the rate of S. aureus during the study period. MRSA is still an important cause of nosocomial infections at the hospital, even with intensification of a preventive nosocomial infections campaign that includes reinforcement in hand washing policies, placement of alcohol dispensers in all hospital and ambulatory-care areas, emphasizing of contact precautions for all patients with proven MRSA infection, and active surveillance of cultures.
An outbreak described at an oncological center in Houston identified 70 nosocomial MRSA isolates. There were 3 predominant clones in 25 of 33 strains (76%); 11 patients with clone A (SCCmec type II). Following the implementation of interventional measures, a significant decrease in nosocomial MRSA isolates was noted. 13 It shows that measures implemented by a good infection control program are an additional tool to control bacterial resistance.
A study performed at a cancer hospital center in Ireland reported an MRSA incidence of 20.3% in patients with febrile neutropenia and bacteremia. A worrying trend was the high level of methicillin resistance noted among S. aureus isolates (89.3%), and the increasing rates in recent years. 14 Our study showed the same trend.
Nevertheless, the causes of MRSA propagation remain controversial, and contradictory conclusions have been drawn from different studies. 20 Additionally, MRSA are also resistant to different classes of antibiotics and have been reported to acquire resistance to gentamicin and related aminoglycosides. 9 All strains in this series demonstrated susceptibility to gentamicin and glycopeptides.
It was found that 71% of the patients had received antimicrobials recently. Detailed knowledge of susceptibility to antimicrobial agents is essential to facilitate the development of effective strategies to combat the growing problem of resistance. 3 Clinicians should obtain material for culture and susceptibility testing from all suspected sites including abscesses and skin infections, especially those with necrotic areas. 23
Molecular typing techniques allow identification of pandemic clones of MRSA and enable the monitoring of MRSA clones circulating in different hospitals and at different time intervals in a country.12,18 The identification of well-defined clonal groups provides a basis for understanding the dissemination of particular clones in the hospital environment and will aid in preventing further dissemination of MRSA. These techniques should help to predict the emergence of new and even more serious strains of multidrug-resistant bacteria (e.g., New York-Japan, Pediatric clone, USA 300, and USA 400). Such a rapid, extensive spread of MRSA can be due to multiple episodes of horizontal transference and recombination of the mec gene, as suggested by clonal analysis. 10
Nosocomial-associated MRSA have been reported at other hospitals in Mexico, with a wide geographic spread of MRSA-specific clones in the country11,24 similar to that demonstrated with other clones in South America, Europe, and the United States.1,10 In this study, a predominant MRSA clone (clone C) related with New York-Japan and Pediatric clone was detected in this hospital outbreak; it showed three PFGE subtypes and SCCmec type II. The MRSA clone found in this outbreak has been already reported in Mexico at the Hospital Civil Fray Antonio Alcalde in Guadalajara and at the Hospital de Pediatría del Centro Médico Nacional-Siglo XXI in Mexico City, where it has been circulating since 1999 and 2001, respectively.11,24 An outbreak described at an oncological center in Houston identified 70 nosocomial MRSA isolates. There were three predominant clones in 25 of 33 strains (76%); 11 patients with clone A (SCCmec type II). 13 It is noteworthy to mention that the first reports of vancomycin-resistant MRSA were from genetic linage USA 100, which is also known as the New York-Tokyo clone, which is very similar to the Mexican clone C. The SCCmec typing system is used to distinguish between healthcare-associated MRSA and community-acquired MRSA clones. 25 In the United States, two clones, designated as USA 300 and USA 400 by the Centers for Disease Control and Prevention, have been identified as the primary clone types that cause community-acquired MRSA infections. These clones have frequently been associated with the Panton-Valentine leukocidin virulence factor and the presence of SCCmec type IV. 16 In contrast, hospital-acquired or healthcare-associated MRSA strains usually lack genes for Panton-Valentin leukocidin and are associated with other SCCmec (types I, II, or III). MRSA with SCCmec type II tend to be resistant to β-lactams, carbapenems aminoglycosides, macrolides, clindamycin, fluoroquinolones, and glycopeptides, whereas SCCmec type IV are usually resistant to β-lactams and erythromycin but retain susceptibility to clindamycin, trimethroprim–sulfamethoxazole, and fluoroquinolones. Healthcare-associated genotypes are frequently multidrug-resistant.14,16
This study highlights the need for hospital clinicians to be aware of the common bacteria isolated in their unit and their unusual antibiotic susceptibility. Microbes possess the capacity to evolve in response to their environment; the major impetus for developing resistance is selective pressure resulting from antibiotic use.3,9 Although MRSA is now endemic at the hospital, the number of MRSA isolates identified in the past 18 months has decreased since infection prevention and control measures have been implemented. 13
Identification of carriers, isolation of colonized or infected patients, use of barrier precautions, and reinforcement of health workers' hand washing are important strategies for detection and limiting MRSA spread. In the setting of clinical bacteremia, the clinician should immediately initiate empirical therapy with appropriate antimicrobials to cover the possibility of MRSA. Until isolation confirms or denies this, infectious disease consultation is warranted in these cases.
In conclusion, our data show that MRSA has spread to the entire hospital from an index patient who arrived with a surgical site infection from another institution. This case underscores the need to intensify strategies that identify and limit the spread of multiresistant pathogens in tertiary-care hospitals by infected patients referred from other healthcare centers.
Footnotes
Disclosure Statement
All authors report no conflicts of interest relevant to this article.