
Abstract
In Egypt, little is known about the genetic background of Escherichia coli isolates harboring extended-spectrum β-lactamase (ESBL). Five hundred twenty Enterobacteriaceae were prospectively collected (May 2007–August 2008) at the Theodor Bilharz Research Institute (Cairo). Among the collected Enterobacteriaceae, 56% (n = 291) were E. coli and 32% (n = 165) Klebsiella pneumoniae. A total of 16% (n = 83) of all isolates were ESBL, 19% (n = 55) of the E. coli and 14% (n = 23) of the K. pneumoniae. The proportion of E. coli ESBL producers did not differ significantly between in and outpatients (20% vs. 17%) but was significantly different for non–E. coli ESBL producers (18.5% vs. 1.2%: p = 0.0001). The majority of E. coli ESBL producers (75%) was isolated from urine. All the ESBL-producing Enterobacteriaceae available for molecular study (n = 74) produced CTX-M-15. Among the CTX-M-15-producing E. coli isolates; 40% belonged to phylogenetic group A, 32% to D, and 26% to B2. ERIC-2 PCR profiles were obtained for all these E. coli isolates and multilocus sequence typing for those belonging to group B2. Genotyping analyses showed strain diversity; however, some clusters had profiles indistinguishable from that of previously published clones. Multilocus sequence typing showed that 75% of E. coli group B2 belonged to clone ST131. This indicates that a new country in Africa is adversely affected by clones of E. coli–producing CTX-M-15.
Introduction
In Egypt, a high prevalence of infections caused by ESBL-producing E. coli and Klebsiella spp. has been reported in both academic teaching and general hospitals.13,24 Moreover, some research estimates that Egypt ranks among the leaders of the world with respect to ESBL incidence. 4 However, little is known about the genetic background of E. coli populations harboring ESBLs in Egypt. We prospectively collected Enterobacteriaceae clinical isolates from inpatients and outpatients seen at the Theodor Bilharz Research Institute (TBRI) during a 16-month period. These isolates were characterized using molecular genetic techniques to describe dominant genotypes in E. coli contributing to the worldwide epidemiological survey of ESBL-producing Enterobacteriaceae.
Materials and Methods
Setting
A prospective surveillance study was performed at TBRI from May 2007 to August 2008. TBRI is a medical research institution affiliated with the Academy of Scientific Research and Technology in Egypt. It is located in an urban area in Giza, Cairo, Egypt, and comprises a 300-bed hospital with outpatient clinics. It provides services for adults only. Inpatients were patients hospitalized and having a positive clinical sample at least 48 hr after admission, and outpatients were either patients who attended the TBRI outpatient clinics or patients hospitalized and having a positive clinical sample during the first 48 hr after admission.
Bacteria
Nonrepetitive Enterobacteriaceae isolates obtained from all clinical samples received by the microbiology laboratory during the study period were included in the study. Bacterial species were determined using the API 20E system (bioMérieux, SA, Marcy l'Etoile, France) and clinical isolates were preserved in agar stab cultures until use. Representatives of previously published E. coli clones were used as controls in the ERIC-2 PCR analysis: clones ST131, ST95, and ST141 for group B2 isolates; ST709, ST744, ST167, all from clonal complex ST10, and ST606 for group A isolates; and ST117, ST393, and ST69 for group D isolates.21,26 Strains E. coli ATCC 25922 and K. pneumoniae ATCC 700603 were used as internal controls for antibiotic susceptibility and ESBL detection, respectively.
Antibiotic susceptibility and ESBL detection
Antibiotic susceptibility was determined by the agar disk diffusion method and ESBLs were detected by the double-disk synergy test as previously described. 14 The following antibiotics were tested: amoxicillin, amoxicillin/clavulanate, piperacillin/tazobactam, cefoxitin, cefotaxime, ceftazidime, cefepime, aztreonam, imipenem, gentamicin, amikacin, cotrimoxazole, ciprofloxacin, nalidixic acid, norfloxacin, and nitrofurantoin. Results were interpreted using the Clinical and Laboratory Standards Institute criteria. 10
blaCTX-M, blaTEM, and blaSHV gene amplification and sequencing
Total bacterial DNA was purified using DNA QIAmp DNA mini kits (Qiagen, Valencia, CA) according to the manufacturer's instructions. Genes encoding β-lactamase enzymes were amplified using previously described primers. 20 PCR products were purified using QIAquick PCR purification kit (Qiagen) following the manufacturer's instructions. Sequencing reactions were carried out using the Perkin Elmer Big Dye kit. v3.1 (Applied Biosystems, Foster City, CA). Sequence data were collected using an ABI Prism 3100 automated sequencer coupled to data collection software version 2.0, and sequencing analysis software 5.1.1. Nucleotide sequences obtained were assembled using BioEdit (version 7.0.5.3) and aligned with GenBank reference sequences using the Clustal X application within BioEdit.
Molecular analyses of E. coli isolates
E. coli isolates were sorted into the major phylogenetic groups (A, B1, B2, and D) by multiplex PCR as previously described. 9 All E. coli isolates of phylogenetic groups A, B2, and D were typed by using the ERIC-2 PCR method as previously described in comparison with reference clonal strains. 26 Specific PCR experiments were performed, as previously described, to identify those group B2 E. coli isolates belonging to serogroup O25b and those with the pabB gene specific for clone ST131.7,8 Multilocus sequence typing (MLST) was performed on all group B2 isolates as previously described using the E. coli MLST scheme described at http://mlst.ucc.ie/mlst/dbs/E.coli, which is based on sequencing of internal regions of seven housekeeping genes adk, fumC, gyrB, icd, mdh, purA, and recA. 26
Statistical analysis
The chi-squared test and, for small numbers, Fisher's exact test were used for comparison of categorical data. Continuous variables were compared using the Mann–Whitney test. p ≤ 0.05 was considered statistically significant.
Results
Epidemiology of ESBL-producing Enterobacteriaceae
During the study period, 520 nonrepetitive clinical isolates of Enterobacteriaceae were collected. These isolates came from 320 (62%) inpatients and 200 (38%) outpatients (Table 1). Overall, the percentage of Enterobacteriaceae producing an ESBL was 16% (83/520) (Table 1). There was no significant difference between patients with an ESBL-negative isolate (n = 437) and those with an ESBL-positive isolate (n = 83) with regard to age (mean 48 vs. 49.5 years) or sex (male/female ratio: 1.1 vs. 1.5) (data not shown). Although a significantly higher percentage of ESBL-producing Enterobacteriaceae was observed in inpatients than in outpatients (19% vs. 11%; p < 0.007) (Table 1), the percentage of urinary ESBL-producing enterobacterial isolates was not significantly different between inpatients and outpatients, 17% versus 14%, respectively (data not shown). Inpatients with Enterobacteriaceae isolates were mainly distributed in urology, gastroenterology, and surgical wards, but the percentage of those with ESBL-positive enterobacterial isolates was significantly higher in intensive care unit than in the other hospital wards (47% vs. 16.5%; p < 0.001) (data not shown).
Two Morganella morganii, one Enterobacter cloacae, one Providencia rettgerii, one Citrobacter freundii.
n, number; +, isolate producing ESBL.
ESBL, extended-spectrum β-lactamase.
Among the collected Enterobacteriaceae isolates (Table 1), E. coli and K. pneumoniae were the main species identified (56% and 32%, respectively). Nineteen percent of the E. coli isolates and 14% of the K. pneumoniae isolates were ESBL producers, whereas 8% of the other species identified were ESBL producers (two Morganella morganii, one Enterobacter cloacae, one Providencia rettgerii, and one Citrobacter freundii).
The percentage of ESBL-producing E. coli isolates did not differ significantly between in and outpatients with an E. coli clinical isolate (20% vs. 17%), whereas the percentage of ESBL-producing K. pneumoniae isolates significantly differed between in and outpatients with a K. pneumoniae clinical isolate (18% vs. 2%, p < 0.02) (Table 1).
Antibiotic susceptibility
Antibiotic susceptibility testing (data not shown) showed that ESBL-positive enterobacterial isolates had significantly higher resistance rates to ciprofloxacin (91%), gentamicin (71%), and piperacillin/tazobactam (62%) than the ESBL-negative isolates, 54%, 45%, and 39%, respectively (p < 0.05). In contrast, the resistance status of isolates to amikacin, nitrofurantoin, and cotrimoxazole was not affected by the ESBL status of the isolates. None of the isolates were resistant to imipenem.
ESBL characterization
Of the 83 isolates phenotypically identified as ESBL producers, only 74 (47 E. coli, 22 K. pneumoniae, and 5 other species) were available from subcultures. PCR amplification of the bla genes and DNA sequence analysis showed that the 74 isolates produced CTX-M-15. The association of CTX-M-15 and SHV-12 was detected in one E. coli isolate.
Molecular analysis of the 47 available CTX-M-15-producing E. coli isolates
The genetic background of the 47 CTX-M-15-producing E. coli isolates showed that they were almost evenly distributed into three of the four E. coli phylogenetic groups: 40% group A, 32% D, and 26% B2. Only one isolate belonged to group B1. ERIC-2 PCR revealed a great diversity among the isolates of each phylogenetic group (Tables 2 and 3). The 14 isolates of group A that were typed displayed 10 different profiles and 6 of the isolates had a profile similar to that of representatives of either clone ST709 (n = 1) or clone ST744 (n = 5), both belonging to clonal complex ST10 (Table 2). Similar diversity was detected in the 15 isolates of group D (Table 2). Ten profiles were observed; three patterns, PfD3 (n = 4), pfD6 (n = 2), and PfD9 (n = 2), consisted of multiple isolates whereas the remaining seven isolates each had a unique pattern. For the 12 isolates of group B2, five profiles were determined (Table 3). One of these profiles was shared by five isolates (42%). This profile was indistinguishable to that of the representative of clone ST131 and thus named PfB2 ST131. Another profile shared by four other isolates of group B2 differed from profile PfB2 ST131 by one band (800 bp). However, it differed from profiles PfB2 3, 4, and 5 by more than one band (Fig. 1) and was this labeled PfB2 2. The isolates with profiles PfB2 ST131 and PfB2 2 were positive for O25b and pabB PCR experiments whereas isolates with profiles PfB2 3, 4 and 5 were negative. The MLST experiment showed that the isolates with profiles PfB2 ST131 and PfB2 2 belonged to ST131, whereas those with profiles PfB2 3, 4, and 5 profiles belonged to ST73, ST127, and ST405, respectively (Table 3).
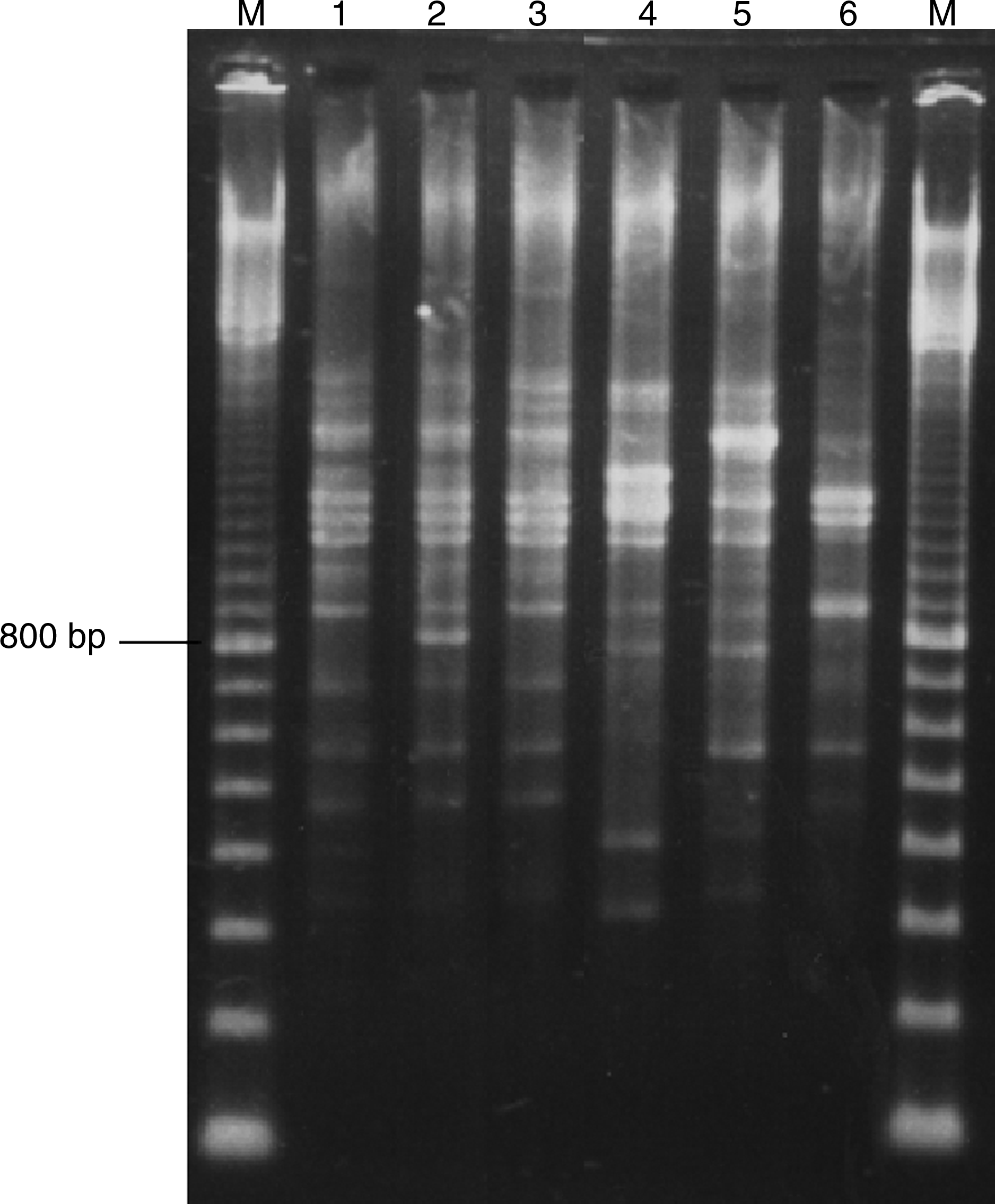
ERIC-2 PCR profiles of Egyptian group B2 Escherichia coli producing CTX-M-15 in comparison with that of a representative of clone ST131. Lane 1, representative of clone ST131; lane 2, Egyptian isolate E 450 (profile PfB2 2); lane 3, Egyptian isolate E 46 (PfB2 ST131); lane 4, Egyptian isolate 275 (profile PfB2 3); lane 5, Egyptian isolate E 298 (profile PfB2 4); lane 6, Egyptian isolate E 971 (profile PfB2 5). M, weight marker (100 bp ladder). The band corresponding to 800 bp is indicated.
Profiles corresponding to the profile of representatives of clones ST709 and ST744.
Asc, ascitic; Clinics, outpatients clinics; GE, gastroenterology; ICU, intensive care unit; In, inpatient; NA, not available; Out, outpatient; SR, surgery; UR, urology.
Profiles corresponding to the profile of representative of clone ST131.
ST405 was first identified in an isolate of group B2 11 and very recently in isolates of group D.23,30
+, PCR positive;−, PCR negative.
Discussion
In this study, we determined the genetic background of ESBL-producing E. coli isolates obtained from outpatients (n = 200) and inpatients (n = 320) taken in charge in an urban tertiary-care hospital of a medical research institute located in Cairo, Egypt. To our knowledge, this is the first report from Egypt to address this aspect of ESBL-producing bacteria.
The overall proportion of ESBL-producing enterobacterial isolate was 16%. Higher ESBL detection proportion than ours was suggested in previous studies from Egypt: 38% by El Kholy et al. 13 and 61% by Mohamed Al-Agamy et al. 24 This observed difference may be due to lack of confirmatory testing for ESBL production in Enterobacteriaceae resistant to extended-spectrum cephalosporins isolated from blood, in the first study, and the small number of isolates under study comprising only E. coli isolates, in the second study.
In the current study, the proportion of ESBL producers was higher in E. coli (19%) than in K. pneumoniae (14%). This finding differs from other countries in the region (e.g., Saudi Arabia, Israel, and Turkey), where ESBL-producing Klebsiella spp. isolates exceeded ESBL-producing E. coli isolates.1,16,28 Two aspects of our study may have influenced this outcome: a great proportion of our Enterobacteriaceae clinical isolates came from outpatients (200 out of 520) and the percentage of enterobacterial isolates from patients in intensive care unit was small (6%). These factors may account for the higher proportion of ESBL-producing isolates of E. coli, knowing that E. coli is currently the enterobacterial species most concerned with ESBLs and that ESBL-producing E. coli is the cause of infection found in the community. 5
There was no significant difference in the proportion of urinary ESBL-producing E. coli between inpatients and outpatients. This observation may indicate the dissemination of these pathogens in the community in Cairo.
CTX-M enzymes are the most prevalent ESBLs spreading among bacteria in most parts of the world. 3 Molecular analysis and sequencing of ESBL produced by our isolates demonstrated the exclusive identification of CTX-M-15 in all isolates independently of the species. Previous studies have already observed that CTX-M-15 is the most commonly reported ESBL in the Middle East region and North Africa.17,25,33,35
As the majority of our ESBL producers were E. coli isolates and as all were producers of the worldwide disseminating CTX-M-15 enzyme, we attempted to analyze the genetic background of these isolates. 26 Phylogenetic groups B2 and D are known to be the groups most extraintestinal pathogenic E. coli isolates belong to; these were present in 26% and 32% of our isolates, respectively. 32 However, E. coli isolates of group A, that is the group which E. coli commensal isolates belong to, were identified in 40% of our ESBL-producing clinical isolates of E. coli. 32 This percentage is higher than that (13.6%) found by Lavigne et al. in France but very similar to that (40.2%) found by Oteo et al. in Spain.19,27 Moreover, we identified as previously reported by Oteo et al. that a great proportion of our group A isolates belonged to the clonal complex ST10. 27
Among our 12 group-B2 E. coli isolates, 9 (75%) of belonged to clone ST131 according to the MLST typing system. We observed, for the first time, that isolates of clone ST131 can have ERIC-2 PCR profiles with small banding pattern differences. Until now, banding pattern differences within isolates of clone ST131 had been observed with the pulsed-field gel electrophoresis typing method and not with the ERIC-2 PCR typing method. 21
In the first description of the intercontinental clone ST131, isolates from Africa were not explored.11,26 However, clone ST131 has recently been detected in Central African Republic and Tunisia.7,12 Thus, this study confirms the presence of this clone in another country in Africa. Our study has also demonstrated that one CTX-M-15-producing E. coli of group B2 belongs to clone ST73. This clone was found to produce CTX-M-14 in Japan. 31 It has also recently been identified in non-ESBL-producing, adherent-invasive E. coli isolates including two isolates coming from nonepidemiologically linked patients suffering from Crohn's disease and one from a patient with a urinary tract infection. 22 Finally, one of the two remaining clones identified in our group B2 isolates showed a sequence type, namely, ST405, which was first identified in a group B2 CTX-M-15-producing E. coli isolate from Portugal 11 and has very recently been identified in isolates of group D subtype D2.23,30 Overall, our study confirms that E. coli clone dissemination is a way by which CTX-M-15 disseminates, notably in the community, in Cairo.
Organisms producing ESBLs are typically known to be resistant to multiple classes of antibiotics. CTX-M-15-positive isolates in our study were found to be significantly more resistant to ciprofloxacin than the ESBL-negative isolates. The association between CTX-M-15 ESBL producers, particularly for those of clone ST131, and resistance to ciprofloxacin has been found to range from 87% to 100%.2,15,26 Ciprofloxacin, which is an oral antibiotic and intravenous antibiotic available in Egypt without prescription, is frequently used for treating hospital- and community-acquired urinary and gastrointestinal infections in our institute. Our epidemiological data might suggest that the frequent use of ciprofloxacin in Egypt may be the driving force for selecting E. coli–producing CTX-M-15.
In conclusion, this study represents the first molecular epidemiological study performed on both hospital and community enterobacterial isolates producing ESBLs from Egypt. It suggests that ESBLs of the CTX-M-15 type are equally pervasive in both hospital and community settings in this country.
Footnotes
Acknowledgments
This study was supported by TBRI Microbiology project (79 D), Egypt-France Scientific and Technological Cooperation Program “Imhotep” (contract No 57 for project FGY/FRA5-007/N° 20726WB), the cooperative program between TBRI and Beaujon Hospital, and Clinical Trials and Military Studies Research Fund of the U.S. Navy Medical Research Unit 3, Cairo.
The opinions and assertions contained herein are the private ones of the authors and are not to be construed as official or as reflecting the views of the Department of the Navy, Department of Defense, or the U.S. Government.
Disclosure Statement
All authors declare that no commercial associations exist that might create a conflict of interest in connection with this study.