
Abstract
Community-based information on antibiotic susceptibility of urinary bacteria is useful in clinical practice, including empiric therapy. Owing to evidence of coselection of metal and antibiotic resistance, there is growing concern on testing of such selective pressure in clinical as well as environmental bacterial isolates. We examined arsenic tolerance and antibiotic resistance in urinary isolates and their possible coselection among arsenic-exposed subjects. Urinary arsenic levels were assessed by atomic absorption spectrophotometer. Antibiotic resistance and arsenic tolerance of urinary bacteria were observed by modified Kirby-Bauer and minimum inhibitory concentration methods, respectively. The percentage of one, two, and multidrug-resistant urinary isolates were 30.4%, 37%, and 30.4%, respectively. Isolates showed variable tolerance to arsenic species. Gram-negative isolates were more tolerant to arsenic species than Gram positive. Although statistically insignificant, arsenic tolerance tended to increase from total susceptible to two-drug resistance. However, multiple drug resistance was not induced by the urinary arsenic (p > 0.05). We observed moderately positive correlation between urinary arsenic level to arsenic tolerance of isolates (p < 0.05). Although tolerance significantly correlated to urinary arsenic level, coselection/coresistance of arsenic to the antibiotic resistance in urinary isolates is inconclusive and remains to be further elucidated.
Introduction
In healthy community people, asymptomatic bacteriuria (ABU) is common and its prevalence varies by age, gender, and sexual activity. 4 Therefore, we may consider the ABU as a concomitant condition among arsenic-exposed people. ABU is often considered as a predictor of subsequent urinary tract infection (UTI)—one of the most common bacterial infections.6,8 With the growing concerns over drug-resistant bacteria and their geographical variations, information regarding antibiotic susceptibility of urinary bacteria isolated from community people is useful for clinicians in practicing empiric therapy of community-acquired UTI. 7
Bacteria may possess intrinsic or acquired resistance not only to drugs but also to diverse metals.1,6 Bacterial resistance to arsenic is genetically determined by expression of ars operon.2,18 There are reports that metal and antibiotic resistances are genetically linked and such co- or cross-resistance has mainly been reported for mercury, lead, copper, and nickel.1,17,19 Owing to this, we hypothesized that urinary arsenic might induce or coselect antibiotic resistance among the bacteria thriving in the urine or bladder.
In this article, we indicate antibiotic resistance and arsenic tolerance among urinary isolates and observe their inconclusive co- or cross-resistance. Also, we observe the correlation between arsenic tolerance of bacteria and urinary arsenic levels.
Materials and Methods
Study sites and population
Communities at program areas of Filters for Families in Nawalparasi district, an organization involved in arsenic mitigation program in Nepal, were selected as study sites. These included five Village Development Committees (Jahada, Sarawal, Sunawal, Sukrauli, and Swati) and one municipality (Ramgram). From data of Filters for Families, 60 households were randomly selected that had arsenic concentration exceeding 50 μg/l. We included two interested members from each targeted household (preferably one male and one female) aged over 5 years for midstream spot urine sample collection. To avoid getting apparently high urinary arsenic levels in our study subjects apart from drinking water, we excluded during sampling the subjects with history of fish consumption within past 2 days. Before any data collection, the informed consent was obtained from each subject.
Urine sampling and analysis
Sampling
After explaining the purpose and method of sample collection, each subject was asked to provide midstream urine into a sterile urine culture plastic tube. The samples were refrigerated at − 4°C and cultured before 72 hr.
Urine culture
The urine samples were cultured by the conventional method on MacConkey agar (without crystal violet and sodium chloride and with sodium taurocholate) to produce isolated colonies. The urine samples were also half-streaked on blood agar plates. Bacterial isolates from the MacConkey agar culture plates were subcultured on the nutrient agar and identified using staining technique and a battery of selected biochemical tests and other specific tests. As a routine tests, these included Gram staining, catalase and oxidase tests; IMViC test; indole, methyl red, Voges-Proskaur, and citrate utilization tests; triple sugar iron, urease, and motility tests; oxidation/fermentation and sugar utilization tests; coagulase tests; and novobiocin susceptibility testing.
Antibiotic susceptibility testing
We used the standard modified Kirby-Bauer disk diffusion method for this testing. Mueller-Hinton agar and antibiotic disks were purchased from HiMedia, Lab, and manufacturer's instructions were followed for the testing. Antibiotics for the testing were chosen considering their antibacterial spectrum, species of bacteria, availability, and their recent trend of use to treat community-acquired UTI in Nepal. The antibiotics used during antibiotic susceptibility testing for urinary isolates included amoxicillin, cotrimoxazole, ciprofloxacin, ceftriazone, norfloxacin, erythromycin, cloxacillin, cephalexin, and vancomycin, ofloxacin, nitrofurantoin, gentamycin, and amikacin.
Minimal inhibitory concentration
We used two inorganic arsenic salts—sodium arsenate (Na2HAsO4·7H2O) and sodium arsenite (NaAsO2)—to determine the minimal inhibitory concentration (MIC) of bacterial isolates. Pentavalent form of arsenic, As(V), in sodium arsenate is less toxic than its trivalent form, As(III), in sodium arsenite. The MIC determination was performed by the conventional method. 6 The optimized working solutions were prepared after several hit-and-trial experiments until the best results were obtained. MIC values of As(III) to urinary bacteria were determined by tube dilution method using 200 parts per million (ppm) As(III) working solution. However, MIC values of As(V) to urinary bacteria were determined by preparing solutions of different concentrations (ranging from 200 to 1,000 ppm at succession of 80 ppm) using 4% As(V) working solution.
Total arsenic measurement of urine
Total arsenic concentration in urine samples were measured by an atomic absorption spectrophotometer (SOLAAR 969AA Spectrometer; Thermo Elemental), equipped with a hydride generator (HG-AAS). One milliliter of each sample was digested with low heat with 25 ml concentrated H2SO4 and 5 ml HNO3 in a Kjeldhal flask over the Kjeldhal digestion unit. Five milliliters of HNO3 was further added along with 0.5 ml HClO4 and digested again until no color remained. The sample was then diluted by adding 10 ml de-ionized water and treated with prereductants—NaI and HCl for 30 min. During analysis, NaBH4 solution along with HCl was passed over the air acetylene flame into quartz tube to atomize arsenic. The HG-AAS was calibrated by using As(V) standard solutions that had gone through the same procedures as the sample solution. Assay accuracy was ensured by inclusion of reference materials, NIES CRM No. 18 (Human Urine, National Institute for Environmental Sciences, Tsukuba, Japan) with total arsenic of 0.137 ± 0.011 mg/l. The detection limit of the HG-AAS for arsenic in urine was 10 μg/l.
Statistical analysis
Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) software version 11.5 (SPSS, Inc.). Correlation and mean difference between two continuous variables were calculated as Pearson's correlation coefficient and t-test, respectively. A p-value of < 0.05 was considered statistically significant.
Results
Urinary isolates and antibiotic susceptibility patterns
We cultured 118 urine samples of which 44 (37.2%) showed growth of bacteria. Growth of urinary isolates was higher in females (28/66:42.2%) than in males (16/52:30.7%). The highest positive growth (16/34:47%) was observed in age group 31–45 years followed by in age group 15–30 years (14/36:38.8%). Of total 46 urinary isolates, Escherichia coli was the most common (9:19.6%) followed by Pseudomonas aeruginosa (8:17.4%). The percentage of multidrug-resistant (MDR: greater than or equal to three drug resistance), two drug-resistant, one drug-resistant, and total susceptible isolates were 30.4%, 37%, 30.4%, and 2.2%, respectively. Acinetobacter spp. and Staphylococcus epidermidis were the most drug-resistant isolates: three out of four isolates were MDR for each (Table 1).
As, arsenic; DR, drug resistance; ppb, parts per billion; TS, total susceptible.
Among 25 Gram-negative urinary isolates, 96% (24/25) and 76% (19/25) isolates were susceptible to norfloxacin and ciprofloxacin, respectively. Among 21 Gram-positive urinary isolates, 76.1% (16/21) were susceptible to ciprofloxacin and ceftriazone. Eighty percent (20/25) of Gram-negative and 90.5% (19/21) of Gram-positive isolates were resistant to amoxicillin (Table 2).
Ak, amikacin; Am, amoxicillin; Cef, ceftriazone; Cep, cephalexin; Ci, ciprofloxacin; Clo, cloxacillin; Co, cotrimoxazole; Ery, erythromycin; Gen, gentamycin; I, intermediate; Ni, nitrofurantoin; Nor, norfloxacin; Of, ofloxacin; S, susceptible; R, resistant; Van, vancomycin.
MIC and antibiotic resistance
Urinary isolates showed variable tolerances (or MIC values) to arsenic species. The overall (mean of the means) tolerance of all isolates to As(V) and As(III) were 509.67 and 10.46 ppm, respectively. The overall mean fold toxicity of As(III) over As(V) was 48.72 times. Among Gram-negative and -positive isolates there was significant difference in tolerance to As(V) but not to As(III) (Table 3).
ppm, parts per million.
We observed increasing tolerance to both arsenic species by all susceptible to two-drug resistant isolates and fall-down in case of MDR. However, such difference was statistically insignificant (p > 0.05) (Figs. 1 and 2). The mean arsenic tolerances of non-MDR and MDR isolates to As(III) were 9.17 and 8.92 ppm and to As(V) were 533.75 and 458.57 ppm, respectively. These differences were also statistically insignificant (Table 4). One-way analysis of variance also showed that there was no significant difference in mean arsenic tolerance by one, two, and multiple drug-resistant isolates (data not shown). However, the three most common isolates, E. coli, P. aeruginosa, and Staphylococcus saprophyticus, showed significant mean difference in tolerance to As(V) (p < 0.05) (Table 5).
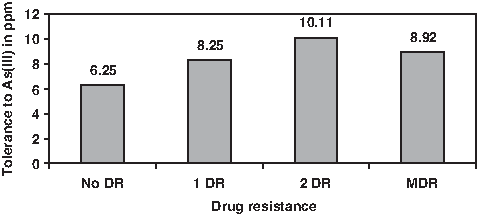
As(III) tolerance in urinary isolates. DR, drug resistance; MDR, multidrug resistant.
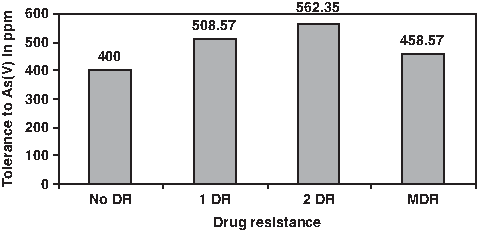
As(V) tolerance in urinary isolates.
MDR, multidrug resistant; SD, standard deviation.
Post ad hoc analysis of significant variables, that is, grouping variables to tolerance to As(V), showed significant mean difference in between S. saprophyticus and P. aeruginosa.
Var, variable.
We observed moderately positive significant correlation of urinary arsenic levels to both As(V) and As(III) tolerances of the isolates. The correlation was stronger to As(III) than to As(V). There was no correlation between tolerance of As(V) and As(III) of the isolates (Table 6).
Discussion
We observed considerable number of antibiotic-resistant urinary bacteria from our study subjects in the community setting. Coselection of increasing antibiotic resistance and MDR to arsenic tolerance of isolates was not clear cut; however, arsenic tolerance correlated to urinary arsenic level.
Bacteriuria was more common in females than in males. Large proportion of our study subjects was of reproductive age. Women are more prone to bacteriuria than men due to short urethra and its proximity to anus, and chances of bacterial contamination of female urethra increases during sexual activity. Bacterial growth increased from age group < 14 years to age group 31–45 years following the general conception that the prevalence of ABU increases with the age.4,6,16 Like bacteriuria, age and gender are the risk factors of arsenic disease in the same population. 13
Our results of antibiotic susceptibility testing may be useful in choosing appropriate antibiotics for empiric therapy of bacteriuria/community-acquired UTI in our study area. Both Gram-negative and Gram-positive isolates were highly resistant to amoxicillin; hence, amoxicillin finds almost no clinical utility. From the antibiotic sets we used, ciprofloxacin and norfloxacin are the most clinically usable antibiotics to all Gram-negative isolates, and ciprofloxacin and ceftriazone to all Gram-positive isolates. Selectively used gentamycin and vancomycin for P. aeruginosa and S. faecalis were found to be 100% effective.
Bacteria have genetic determinants to combat the toxic effects of arsenic ions. In bacteria the most significant effect of As(III) is denaturation of enzymes by binding to their sulfhydryl groups and that of As(V) by the alteration of phosphorylation. This might explain why As(III) is much more toxic than As(V). 2 In aggregate our results also showed that As(III) is nearly 49 times more toxic than As(V) to urinary bacteria. One most characterized genetic system that confers arsenic resistance in bacteria is ars operon, which encodes specific efflux pumps that extrude As(III), thus lowering its intracellular concentration. Bacteria may also confer resistance to As(III) by enzymatic oxidation to less-toxic As(V).2,18
In arsenic-exposed subjects, urinary bacteria thriving in urine counteract mainly to organic arsenic at the range of parts per billion. However, the isolates tolerated well inorganic arsenic up to the level of ppm in vitro, which is much more toxic than pentavalent organic arsenic. Our observance of positive correlation between the arsenic tolerance of urinary isolates and urinary arsenic levels indicates that the arsenic concentration at parts per billion level is sufficient to induce increased tolerance or possibly the resistance in bacteria irrespective of its two forms. Although we observed wide difference in arsenic tolerance levels among the isolates, moderate positive correlation was evident between arsenic tolerance and the urinary arsenic level and is the consequence of arsenic exposure in subjects. Such arsenic exposure in our study subjects occurs predominantly through drinking water. Exposure through food is the second most common route of arsenic exposure, which, in our highly arsenic-exposed subjects through drinking water, has much lower impact and may be attributed to interindividual variation urinary arsenic levels. 22
The increasing trend of arsenic tolerance by more resistant isolates was statistically insignificant and inconsistent. Increase in arsenic tolerance up to two-drug resistant and fall-down in MDR isolates is not a sure indication or a linear relationship in between coselection/coresistance of arsenic and antibiotic. Large samples with ample distribution of isolates in each category are needed for validation. Unlike modified Kirby-Bauer method to determine antibiotic resistance, there are no standard arsenic resistance criteria defined for bacteria. This complicated the determination of coresistance in our study—we were unable to define a threshold concentration above which an isolate could be considered as resistant rather than determined the tolerance instead of resistance. Sabry et al. 17 did not find the coresistance of arsenic and antibiotic in bacterial isolates from sea water, which was evident to metals like lead, copper, and nickel. It seems that reports on coresistance of antibiotics and metals have mainly been elucidated among environmental isolates, and the resistance threshold of arsenic species is found to vary according to the class and habitat of the isolate.5,10,21
Dose–response relationship exists between arsenic exposure and incidence of bladder cancer. 20 Dimethylarsinic acid (DMA) found in urine plays a role in bladder carcinogenicity. Intestinal bacteria often infecting urinary bladder such as E. coli can modify DMA in urine into intermediate products that possess cytotoxic and genotoxic effects and are hypothesized to play a role in carcinogenicity of DMA. 12 Since cystitis (i.e., bladder infection) is assumed to have possible role in bladder cancer, 11 we may hypothesize that bacteriuria may interact with arsenic exposure to the development of bladder cancer.
In conclusion, surveillance of antibiotic susceptibility of urinary bacteria in a specific geographical area can give knowledge about patterns of drug resistance and guidance to clinicians for empiric therapy of community-acquired UTI or bacteriuria. Coselection/coresistance of arsenic to increasing or multiple drug resistance in urinary isolates is not clear cut and remains to be further investigated.
Footnotes
Acknowledgments
We thank International Foundation for Science, Sweden, for funding and are obliged to the people of Nawalparasi district for participation.
Disclosure Statement
No competing financial interests exist.