
Abstract
There is limited clinical information regarding community-onset bacteremia caused by extended-spectrum β-lactamase (ESBL)–producing Klebsiella pneumoniae. This study was performed to evaluate risk factors and clinical outcomes of community-onset bacteremia caused by ESBL-producing K. pneumoniae. A total of 435 patients with community-onset K. pneumoniae bacteremia were included and data from patients with ESBL-producing K. pneumoniae bacteremia were compared to those with non-ESBL-producing bacteremia. Isolates with ESBLs were microbiologically characterized. Of 435 patients with community-onset K. pneumoniae bacteremia, 33 (7.6%) were infected with ESBL producers, of which 25 were further classified as healthcare-associated infections. The most common underlying diseases were solid tumors (n = 20, 60.6%) and diabetes mellitus (n = 10, 30.3%), and the most common infection was intra-abdominal infection (n = 20, 60.6%). Multivariate analysis showed that corticosteroid use (odds ratio [OR] = 13.73, 95% confidence interval [CI] = 1.93–97.6, p = 0.009), percutaneous tubes (OR = 7.30, 95% CI = 2.41–22.12, p < 0.001), and prior receipt of antibiotics (OR = 5.65, 95% CI = 2.43–14.16, p < 0.001) were significant factors associated with ESBL producers. When the 30-day mortality rate was evaluated, no significant difference was found between ESBL group and non-ESBL group (12.1% [4/32] vs. 16.0% [35/192]; p = 0.429). Among 16 isolates, for which the ESBL characterization was performed by PCR, the most common types of ESBLs were SHV (n = 16) and cefotaxime-M-2 (n = 5). Pulsed-field gel electrophoresis analysis of the ESBL-producing organisms showed extensive clonal diversity. ESBL-producing K. pneumoniae is a significant cause of bacteremia, even in patients with community-onset infections, particularly in patients with corticosteroid use, percutaneous tube, prior receipt of antibiotics, or healthcare-associated infections.
Introduction
Despite the high prevalence of hospital-acquired ESBL-producing K. pneumoniae infections, little is known regarding community-acquired ESBL-producing K. pneumoniae infections. Even though previous studies have reported the clinical and microbiological epidemiology of ESBL-producing E. coli infections, there are clinical and epidemiological differences between K. pneumoniae and E. coli infections, in relation to virulence and clinical outcome. Therefore, it is important that the risk factors for infections by ESBL-producing K. pneumoniae be identified to develop effective strategies to manage these infections. This study was performed to evaluate clinical features and outcomes of community-onset ESBL-producing K. pneumoniae bacteremia and to identify the risk factors for ESBL-producing K. pneumoniae bacteremia among patients admitted to the Emergency Department (ED).
Materials and Methods
Study population and design
We reviewed the medical records of individuals found to have K. pneumoniae bacteremia from January 2002 to September 2009 at Samsung Medical Center (Seoul, South Korea), a 1950-bed tertiary care university hospital. Patients were included in the study if their blood cultures were drawn in the ED within 48 hours of admission and the culture results were positive for K. pneumoniae. The annual ED census of the hospital is approximately 55,000 visits.
A case–comparator study was performed to evaluate clinical features and outcomes of patients with community-onset ESBL-producing K. pneumoniae bacteremia who were admitted to the ED. We compared data from patients with community-onset ESBL-producing K. pneumoniae bacteremia with those from patients with non-ESBL-producing bacteremia. For the comparison group, patients found to have non-ESBL-producing K. pneumoniae bacteremia between January 2006 and September 2009 were included.
The data collected included age, gender, underlying disease, type of infection, and antimicrobial regimen. The presence of the following comorbid conditions was documented: neutropenia, recent surgical procedure, corticosteroid use, immunosuppressant use, presence of an indwelling urinary catheter, and percutaneous tube. Since this study was observational, patient management and antimicrobial treatment regimens were chosen by the patients' physicians without any guidelines or intervention from the study investigators. This study was approved by Institutional Review Board of Samsung Medical Center (Seoul, Korea).
Definitions
K. pneumoniae bacteremia was defined as the presence of K. pneumoniae in the blood, documented by at least one positive blood culture. The site of infection was determined by the patients' physicians on the basis of the isolation of K. pneumoniae from the presumed portal of entry and clinical evaluation. Community-onset infection was defined as an infection diagnosed within the first 48 hours of hospitalization. Because many cases of bacteremia that are present or incubating upon admission to the hospital are, nonetheless, healthcare-associated, we refer to nonnosocomial bacteremia as community-onset rather than community-acquired. 7 Episodes of community-onset bacteremia were further classified as healthcare-associated if any of the following criteria were present:8,9 history of >48-hour hospital admission in the previous 90 days, hemodialysis, intravenous medication, home wound care in the previous 30 days, or residence in a nursing home or long-term care facility. Without meeting these criteria, cases were considered to be community-associated. Neutropenia was defined as an absolute neutrophil count of <500 neutrophils/mm3. Severe sepsis was defined as sepsis with one or more clinical signs of organ dysfunction. Antimicrobial therapy was considered appropriate if the treatment regimen included ≥1 antibiotic found to be active against the causative microorganisms on in vitro susceptibility testing and if the dose and route of administration conformed to current medical standards.
Initial response to treatment was assessed 72 hours after starting antimicrobial therapy and was classified as follows for the comparison of outcomes: “complete response” to designate patients who had resolution of fever and all signs of infection; “failure” to designate patients who experienced no improvement or experienced deterioration in any of their clinical parameters, and those who died. The main outcome measure used was 30-day mortality.
Microbiological analysis
Species identification was performed using VITEK II (bioMerieux, Hazelwood, MO) a standard identification card. Antimicrobial susceptibility testing and ESBL confirmatory testing were performed using the broth microdilution method or the disk diffusion method, following the recommendations of the Clinical and Laboratory Standards Institute. The ESBL-related genes such as TEM, SHV, cefotaxime (CTX)-M, and OXA were amplified by PCR from clinical isolates as described previously. 13 The MICs of the antibiotics tested were determined by the broth microdilution method. Quality control was performed using strains E. coli 25922 and P. aeruginosa 27853. Pulsed-field gel electrophoresis (PFGE) was performed using a CHEF Mapper XA (Bio-Rad Laboratories, Hercules, CA), as described previously. 5
Statistical analysis
The Student's t-test was used to compare continuous variables, and the χ2 or Fisher's exact test were used to compare categorical variables. To identify the independent risk factors for mortality, a stepwise conditional logistic regression analysis was used to control for the effects of confounding variables. All risk factors with a p-value <0.25 at the bivariate level were included in the multivariate logistic model predicting the 30-day mortality. Odds ratios and their 95% confidence intervals were calculated. All p-values were two-tailed, and p < 0.05 was considered statistically significant.
Results
Characteristics of community-onset bacteremia caused by ESBL-producing K. pneumoniae
Of 435 patients with community-onset K. pneumoniae bacteremia, 33 patients (7.58%) had ESBL-producing K. pneumoniae bacteremia, of which 25 (75.8%) were further classified as having healthcare-associated infections. The annual prevalence of community-onset ESBL-producing K. pneumoniae is shown in Fig. 1. The most common underlying diseases were solid tumors (n = 20, 60.6%), followed by diabetes mellitus (n = 10, 30.3%), and the most common sites of infection were intra-abdominal (n = 20, 60.6%), followed by the urinary tract (n = 9, 27.3%). Data from the 33 patients were compared to 219 patients with non-ESBL-producing K. pneumoniae bacteremia. The clinical characteristics of the study population and the factors associated with ESBL-producers are listed in Table 1. Univariate analysis revealed that significant factors associated with the ESBL-producing group were healthcare-associated infection, corticosteroid use, indwelling urinary catheter, percutaneous tube, and prior receipt of antibiotics (all p < 0.05) (Table 1). No significant differences were found in sites of infection or presence of severe sepsis. Multivariate analysis using a logistic regression model showed that corticosteroid use, percutaneous tube, and a prior receipt of antibiotics were the significant independent factors associated with community-onset ESBL-producing K. pneumoniae bacteremia (all p < 0.05) (Table 2). The underlying diseases of eight cases with community-associated bacteremia were biliary tract diseases such as stone or cancer (n = 5) and polycystic liver disease (n = 1). The remaining two cases had no identified underlying disease and had bacteremic urinary tract infection. Two cases had a prior receipt of antibiotics.
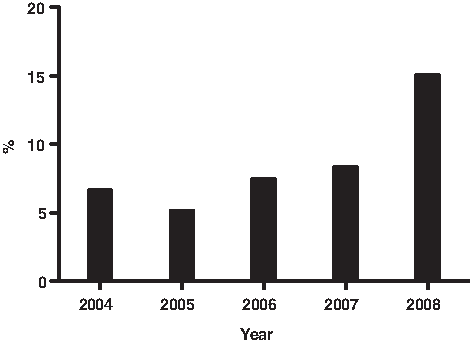
Trend of annual prevalence of community-onset extended-spectrum β-lactamase (ESBL)–producing Klebsiella pneumoniae bacteremia. The proportions of ESBL-producing K. pneumoniae isolates among community-onset K. pneumoniae bacteremia were 6.6% (4/61) in 2004, 5.1% (4/78) in 2005, 7.4% (5/68) in 2006, 8.3% (5/60) in 2007, and 15% (6/40) in 2008.
Data are presented as n (%) of cases, unless otherwise indicated.
Include peritonitis (primary or secondary), pancreaticobiliary tract, or intra-abdominal abscess.
ESBL, extended-spectrum β-lactamase; SD, standard deviation.
Treatment outcomes of community-onset bacteremia caused by ESBL-producing K. pneumoniae
Of 31 patients with ESBL-producing bacteremia, 21 patients (67.7%) received inappropriate initial antimicrobial therapy, whereas only 2 (0.9%) of 214 patients with non-ESBL-producing bacteremia received inappropriate initial antimicrobial therapy (p < 0.001). A total of 30 patients with ESBL-producing bacteremia whose outcomes could be evaluated were compared with 198 patients with non-ESBL-producing bacteremia (Table 3). When early outcomes (72 hours) following the initiation of antimicrobial therapy were assessed, the failure rate was 21.2% (7/30) in the ESBL group and 19.2% (42/198) in the non-ESBL group, which was not statistically significant (p = 0.467). No significant difference was found in the 30-day mortality of both groups (12.1% [4/32] vs. 16.0% [35/192]; p = 0.429) (Table 3).
ESBL characterization and antimicrobial susceptibility of ESBL-producing K. pneumoniae isolates
The results of antimicrobial susceptibility testing, reported as resistance rates of K. pneumoniae isolates causing community-onset bacteremia, are as follows; 30.3% [10/33] for piperacillin/tazobactam, 69.6% [16/23] for amoxicillin/clavulanic acid, 60.6% [20/33] for ciprofloxacin, 12.1% [4/33] for amikacin, 54.5% [18/33] for gentamicin, 39.4% [13/33] for trimethoprim/sulfamethoxazole, and 0% [0/33] for imipenem. Sixteen isolates of ESBL-producing K. pneumonia were included for further microbiological study of ESBL characterization and molecular epidemiology. A SHV-specific PCR was performed with these 16 isolates, with positive results for all isolates. CTX-M-2-specific PCR was positive for five isolates and these isolates were positive for more than two ESBL-related genes. Table 4 shows the ESBL types confirmed by PCR and their antimicrobial susceptibility.
CTX, cefotaxime.
Nineteen isolates producing ESBLs were included in the PFGE analysis. The results of PFGE showed extensive diversity (Fig. 2). Most strains showed unrelated patterns, even though they had the same β-lactamases.
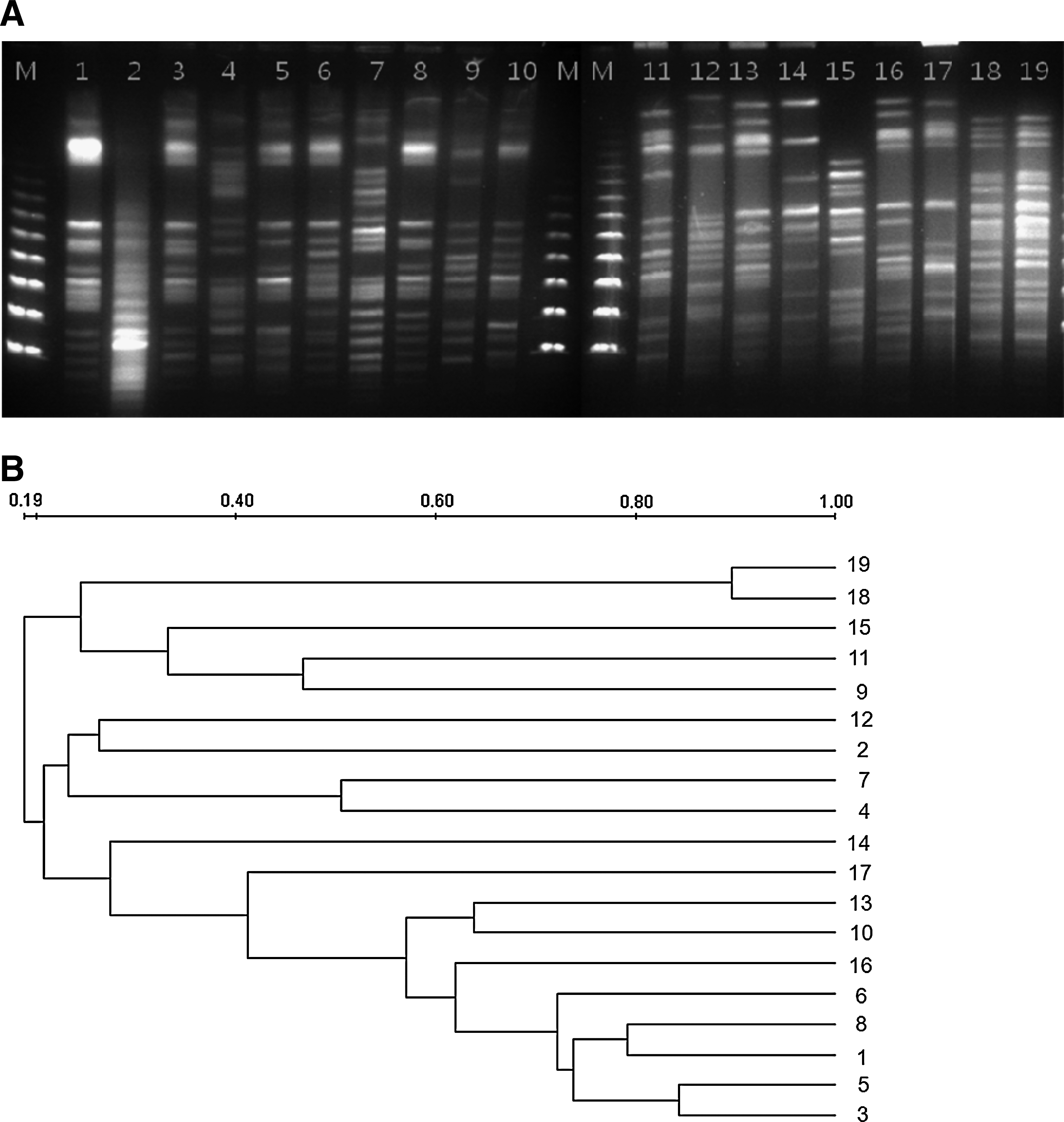
Pulsed field gel electrophoresis
Discussion
The present study showed that ESBL-producing K. pneumoniae is a significant cause of community-onset bacteremia, with relation to healthcare-associated infections. The predominance of SHV and CTX-M enzymes and clonally unrelated isolates were found in the community isolates. ESBL-producing E. coli has emerged in recent years as a cause of community-acquired infections worldwide. Several studies attempted to identify risk factors for ESBL-producing E. coli infections among community-onset bacteremia. An association with healthcare, urinary catheter use, previous antimicrobial use, underlying liver diseases, and unknown primary site of infection were found to be independently associated with ESBL-producing E. coli bacteremia. 21 Our study provides a comprehensive analysis regarding community-onset ESBL-producing K. pneumoniae bacteremia rather than E. coli bacteremia. Corticosteroid use, percutaneous tube insertion, and prior receipt of antibiotics were significant independent factors associated with community-onset ESBL-producing K. pneumoniae bacteremia. Notably, our results demonstrated that the most common site of infection in community-onset ESBL-producing K. pneumoniae bacteremia is intra-abdominal infection, such as in the pancreaticobiliary tract.
Although the frequency of ESBL production by community-acquired K. pneumoniae varies across nations, several reports document their emergence in Europe, Asia, and South and North America.6,12,17 A nationwide study from Italy reported that 2.6% of K. pneumoniae isolates from outpatients were ESBL-positive, 14 and a study from Nigeria demonstrated that CTX-M accounted for 57% of ESBL-producing K. pneumoniae isolates from community-acquired urinary tract infections. 23 In our study, 20.9% (9 of 43) of bacteremic urinary tract infections were ESBL-positive. Although determining the exact prevalence of these organisms in our country (Korea) would require a population-based study, our findings suggest that ESBL producers have already begun to disseminate throughout our community. The extensive diversity of the PFGE patterns of the ESBL-producing strains shown in this study indicates that ESBL-producing strains were endemic in Emergency Department, not just associated with clonal outbreak. The responsible mechanisms are poorly understood, and further investigation to characterize these mechanisms is warranted.
Mortality was not significantly higher for patients with ESBL-producing K. pneumoniae bacteremia than for patients with non-ESBL-producing K. pneumoniae. However, a small number of patients with ESBL-producing K. pneumoniae bacteremia precluded the accurate comparison of both groups with adjustments for comorbid conditions. Previous studies showed that the mortality of bloodstream infections caused by ESBL-producing organisms was higher than that of infections caused by non-ESBL-producing organisms.24,25 Further studies regarding clinical impact of ESBL producers and inappropriate antimicrobial therapy on outcome in community-onset infections are warranted.
Numerous studies have demonstrated that most ESBL-producing Enterobacteriaceae are resistant to multiple antibiotic classes.3,10,22 In a previous study by Ben-Ami et al., community-onset ESBL-producing isolates from most regions displayed high rates of resistance to ciprofloxacin (>70%), which suggests that resistance to fluoroquinolones is prevalent among community-onset ESBL-producing organisms. 3 The resistance rates to ciprofloxacin and TMP-SMX among ESBL-producing K. pneumoniae isolates in our study were 61% and 40%, respectively, which are comparable to rates found in other studies.1–3,6,16,19 Such a high prevalence of resistance to these antimicrobial agents, particularly fluoroquinolones, is a well-known feature of ESBL producers and is of great concern. With regard to the treatment of community-onset bacteremia caused by ESBL-producing organisms, no randomized controlled trials have been performed to date. Our data show that carbapenems remain active against ESBL-producing K. pneumoniae isolates from community-onset bacteremia and are the most reliable agents against ESBL producers. The empirical use of carbapenems should be considered for patients with community-onset intra-abdominal sepsis or urinary tract infections with any risk factor for ESBL-producing organisms, in addition to those presenting with severe sepsis or septic shock caused by gram-negative bacilli. Although carbapenems are considered the drug of choice for serious infections, alternatives such as ciprofloxacin or aminoglycosides, could be alternative. However, the susceptibility profile of our isolates confirms that alternatives for such infections are considerably limited. Despite the findings that ESBL isolates and inappropriate antimicrobial therapy did not affect adversely outcome in our study, previous studies showed that the mortality of bloodstream infections caused by ESBL-producing organisms was higher than that of infections caused by non-ESBL-producing organisms.11,24,25 The limited number of evaluable patients and the possibility of unmeasured confounding variables (e.g., severity of underlying illness and delay in appropriate therapy) make it impossible to draw definitive conclusion regarding the impact of inappropriate antimicrobial therapy on outcome.
The main limitation of the current study is that it was observational and of a retrospective nature. Therefore, the possibility of limitations that preclude accurate comparisons should be kept in mind. With respect to ESBL characterization, the presence of SHV and TEM does not necessarily mean these are ESBLs. Further analyses such as sequence analysis might be needed. Finally, our study was conducted mainly at a large referral center. Thus, many of our patients had serious underlying illnesses, and our findings may not be generalizable to other institutions, particularly community hospitals.
In conclusion, ESBL-producing K. pneumoniae is a significant cause of community-onset bacteremia, with relation to healthcare-associated infections. Community-onset ESBL-producing K. pneumoniae bacteremia was associated with corticosteroid use, percutaneous tube, and prior receipt of antibiotics. Determining the optimal antimicrobial therapy in community-onset K. pneumoniae bacteremia is now becoming a challenge for clinicians in the era of community-onset ESBL-producing bacterial infections.
Footnotes
Acknowledgments
The authors would like to thank Ha Rim Lee for technical support. This study was supported by a research grant from the Korean Society of Infectious Diseases and by the National Research Foundation of Korea grant funded by Korea government (no. 2010-0021572). The bacterial isolates were obtained from Asian Bacterial Bank of the Asia Pacific Foundation for Infectious Diseases.
Disclosure Statement
No competing financial interest exists.