
Abstract
Two mutants of Escherichia coli (V1 and V2) with acquired mechanisms of resistance to fluoroquinolones were isolated sequentially from blood cultures of a patient with cholangiocarcinoma treated repeatedly with ofloxacin; a third mutant (V3) was isolated under ciprofloxacin therapy. All mutants were related clonally. V1 was susceptible to quinolones but with diminished susceptibility to ofloxacin. V2 was hypersusceptible to nalidixic acid but had high-level resistance to ofloxacin. V3 was resistant to all quinolones. Ofloxacin selected for original gyrA and parC mutations, leading to the unusual and misleading resistance phenotypes of V1 and V2, whereas efflux played a major role in the increased resistance of V3.
Introduction
We report the case of a 62-year-old man who presented in February, 2009, for jaundice and weight loss. Biliary endoscopy and biopsies revealed a cholangiocarcinoma. An endoprosthesis was placed to assure biliary drainage, and this procedure was accompanied by a 10-day course of 200 mg of ofloxacin two times a day (b.i.d.)(first course of ofloxacin). Antitumoral treatment consisted of endoscopic phototherapy and chemotherapy. Phototherapy began on March 30 and was associated with a second 10-day course of 200 mg of ofloxacin b.i.d. Two days after the end of this second course, a first episode of angiocholitis occurred and E. coli V1, cultured from blood, appeared susceptible to fluoroquinolones. The infection was successfully treated with amoxicillin-clavulanate (1 g t.i.d. for 10 days). On August 1, the patient experienced a second episode of angiocholitis and received a third course of ofloxacin (200 mg b.i.d.), but remained febrile after 5 days of treatment. Two blood cultures yielded E. coli V2 resistant to ofloxacin. Treatment was switched successfully to 1 g of ceftriaxone once daily (o.d.) for 10 days. On August 25, the patient was put on continuous prophylactic antibiotics (500 mg of ciprofloxacin b.i.d. for 10 days followed by 1 g of amoxicillin–clavulanate t.i.d. for 10 days). On September 8, at the end of the first ciprofloxacin course, he experienced a third episode of angiocholitis. Two blood cultures yielded E. coli V3 resistant to all fluoroquinolones. The patient died from his cancer in October of 2010.
Materials and Methods
Antimicrobial susceptibility was determined by the disk diffusion method (www.sfm.asso.fr/) and minimum inhibitory concentrations (MICs) by the Etest (AB Biodisk, Solna, Sweden). Resistance was defined by zone diameter and MIC breakpoints according to the interpretive criteria of the Comité de l'Antibiogramme de la Société Française de Microbiologie (CA-SFM; www.sfm.asso.fr) and of the European Committee on Antimicrobial Susceptibility Testing (EUCAST; www.eucast.org), respectively.
Molecular typing was achieved by enterobacterial repetitive intergenic consensus PCR (ERIC-PCR) 5 and repetitive extragenic palindromic PCR (rep-PCR). 15 Amplification and sequencing of the quinolone resistance-determining regions of gyrA, gyrB, parC, and parE were performed as previously described. 10
Implication of efflux was appreciated by determining the MICs of quinolones with or without 26 mg/L of efflux inhibitor phenylalanine arginine β-naphthylamide (PAβN). Increased efflux activity was defined as a threefold or more decrease in the MIC of at least one quinolone. 14 Detection of a putative qnr gene and of the aac(6′)-Ib-cr gene variant was performed as described previously.4,6
Results
The three strains had identical ERIC-PCR and rep-PCR patterns (data not shown), indicating a clonal relationship. V1 was categorized as susceptible to all quinolones tested (Table 1). However, the MIC of ofloxacin was at the susceptibility breakpoint (0.5 mg/L) and the zone diameter (26 mm) was just 1 mm above the susceptibility breakpoint and smaller than that of nalidixic acid (28 mm) (Fig. 1). V2 was hypersusceptible to nalidixic acid, with an MIC two-fold lower that that of V1, highly resistant to ofloxacin, levofloxacin, and moxifloxacin, and intermediately resistant to norfloxacin. V2 was still categorized as susceptible to ciprofloxacin (Table 1 and Fig. 1). V3 had low-level resistance to ciprofloxacin and norfloxacin, but high-level resistance to other fluoroquinolones (Table 1 and Fig. 1). Although differences in fluoroquinolone clinical categories exist between the EUCAST and Clinical and Laboratory Standards (CLSI), 13 if the MIC breakpoints for fluoroquinolones defined by the CLSI had been used in our study instead of those of the EUCAST, the categorizations of the strains would have been identical, with only one exception: V2 would have been classified as susceptible to norfloxacin instead of resistant.
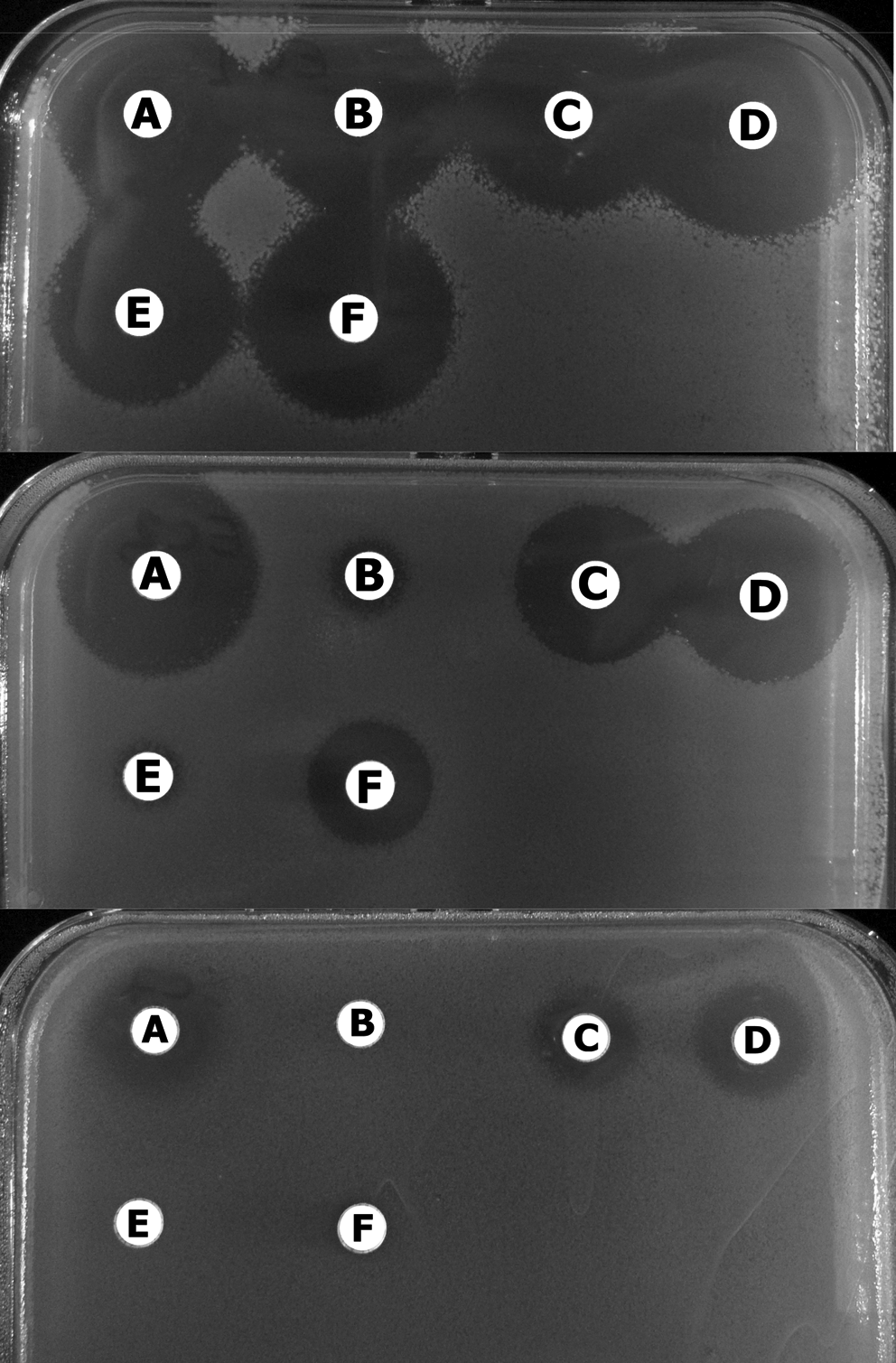
Antibiograms of Escherichia coli mutants V1, V2, and V3 (from top to bottom). (
Values in parentheses correspond to the MIC decrease in the presence of PAβN.
MICs, minimum inhibitory concentrations; PAβN, phenylalanine arginine β-naphthylamide.
V1 harbored one gyrA mutation, leading to the Gly81-Asp subtitution. PAβN induced a significant reduction in the MICs of levofloxacin and moxifloxacin (Table 1). Thus, efflux was also implicated in resistance. V2 carried an additional parC mutation, leading to the Gly78-Asp substitution. No additional mutation was found in V3 but PAβN caused a marked decrease in the MICs of most quinolones tested (Table 1). Efflux was thus largely involved in the increased resistance of V3. No qnr and aac(6′)-Ib-cr genes were detected.
Discussion
We report the first case of in vivo sequential selection by ofloxacin of very rare substitutions Gly81-Asp in GyrA and Gly78-Asp in ParC, leading to unusual and misleading resistance phenotypes. The gyrA mutant V1 remained susceptible to nalidixic acid, ciprofloxacin, and ofloxacin, although a slight decrease in ofloxacin activity was observed. One has to be aware that ofloxacin can select for such difficult-to-detect mutants. However, these peculiar gyrA single mutants have never been described in clinical E. coli strains without an associated parC mutation.1,2 In vitro, single-step gyrA mutants were selected with ofloxacin, and three out of the 12 mutants studied showed a mutation at codon 81 (Gly81-Cys). 2 The possibility that mutant V1 was already present before the first ofloxacin treatment is very unlikely because this patient had not received any antibiotics in the year preceding his hospitalization.
Thus, it may be that ofloxacin can specifically select for mutants at codon 81. It has been shown that the Ser80 residue of ParC (frequently mutated in quinolone resistance) is coordinated with the quinolone C-3 carboxyl group through a highly mobile hydrogen-bonded water molecule. 9 Gly81-Asp modification in GyrA introduces a negatively charged carboxyl group in the vicinity of Ser83 (homologous to Ser80 in ParC) and may disrupt the contacts of this serine, in particular for molecules like ofloxacin or levofloxacin that possess a bulky group at position C-7 (unlike nalidixic acid) and an O-ring between N-1 and N-8 (unlike other fluoroquinolones).
We showed that efflux was also implicated in resistance of V1. Interestingly, two resistance mechanisms can lead to phenotypes difficult to diffentiate from the wild-type. We used the efflux inhibitor PAβN in our experiments because it is known to be active against resistance–nodulation–division (RND) pumps, the ones associated with clinically significant resistance to fluoroquinolones in Gram-negative bacteria. 12 In E. coli, the RND pump most frequently overexpressed by clinical isolates is AcrAB-TolC. 12 PAβN had better efficiency in decreasing the MICs of levofloxacin and moxifloxacin than those of norfloxacin and ciprofloxacin. Similar differences in PAβN efficiency, depending on the fluoroquinolones tested, have already been reported.8,14 The presence of different affinity sites located inside the major efflux pump of E. coli, AcrB, has been demonstrated, and this suggests that the benefit generated by the conjoint use of PAβN and an antibiotic is due to a variable synergistic effect.11,16
Strain V2 acquired a parC mutation identical to the one in gyrA. Such double mutants have never been described. Again, the higher selective advantage conferred by this substitution for ofloxacin explains the peculiar resistance phenotype of V2: High-level resistance to ofloxacin, but hypersusceptibility to nalidixic acid and diminished susceptibility to ciprofloxacin. This phenotype is misleading because resistance may be overlooked if ofloxacin is not tested. The increased resistance of V3 was caused only by efflux, possibly mediated by a very high level of AcrB overexpression. We cannot rule out the implication in resistance of acquired efflux pump QepA because it has been shown that this pump is also susceptible to inhibition by PAβN. However, this is very unlikely because QepA exports preferentially hydrophilic fluoroquinolones (norfloxacin, ciprofloxacin), 3 whereas V3 presented an increased resistance to all fluoroquinolones tested. Thus, efflux can be implicated in the first steps of quinolone resistance but can also occur in later steps.
In conclusion, ofloxacin specifically selected for exceptional gyrA and parC mutations that led to unusual and dissociated resistance phenotypes. In addition, efflux was also largely implicated in the resistance phenotypes of these sequential mutants.
Footnotes
Acknowledgments
We thank Hervé Jacquier for providing oligonucleotides used for aac(6′)-Ib-cr PCR, and Bertrand Picard and Hervé Jacquier for helpful discussion.
Disclosure Statement
No competing financial interests exist.