
Abstract
Tuberculous meningitis is the most severe form of tuberculosis and causes substantial morbidity and mortality in adults and children. The prevalence of multidrug-resistant (rifampin-isoniazid) strains requires the use of more toxic second-line drugs. We report a case of tuberculous meningitis in a 3-year-old Italian child.
Introduction
Case Report
We report a case of tuberculous meningitis in a 3-year-old Italian child. In June 2010, he was admitted to the Pediatrics Department of the Hospital of Cosenza in Italy. He had fever for more than 2 weeks and was irritable and lethargic. On admission, his white blood cell count was 14.8 × 106 cells/μl (normal range: 4.0–11.0) and C-reactive protein level was 1.66 mg/dl (normal range: 0.10–0.80). The chest radiograph was normal. Cerebrospinal fluid (CSF) showed a white cell count of 16 cells/mm3 (normal range: 0–5) with 80% lymphocytes. The other values obtained were as follows: IgG (CSF) 6.03 mg/dl (normal range: 0.48–5.86), albumin (CSF) 54 mg/dl (normal range: 13.90–24.60), and glucose (CSF) 43 mg/dl (normal range: 40–70). Serology for parvovirus, Rickettsia, Borrelia, Epstein-Barr virus, and cytomegalovirus were negative. Polymerase chain reaction (PCR) results for the CSF were negative for herpes simplex viruses12,14 and enteroviruses, but the PCR results were positive for Mycobacterium TB complex (MTB Q-PCR Alert Kit; Nanogen Advanced Diagnostic). Acid-fast bacilli (AFB) from CSF were not detected using Ziehl-Neelsen staining.
The child had not been administered the BCG vaccination. The tuberculin skin test (TST) was negative, but the QuantiFERON-TB (QFT) Gold assay was positive. According to the existing data, 8 QFT is more sensitive than the TST in detecting active TB in children.
Computerized tomography showed tetraventricular hydrocephalus, and magnetic resonance imaging showed basal meningeal enhancement, which is the most common radiological feature of tuberculous meningitis. 10 The treatment was based on prednisone (oral administration [os] daily dosage 2 mg/kg), rifampicin (os daily dosage 15 mg/kg), isoniazid (os daily dosage 10 mg/kg), ethambutol (os daily dosage 20 mg/kg), pyrazinamide (os daily dosage 40 mg/kg), and amikacin (injectable second-line drug, daily dosage 20 mg/kg), but the patient showed little clinical improvement and persistent fever. The incidence of MDR-TB is low in Italy, at approximately 4%, 9 but it was decided to administer amikacin to protect the patient against MDR-TB. The choice of amikacin was based on the fewer renal and auditory toxicities compared with streptomycin given the patient's age. After 15 days, the CSF showed a white cell count of 128 cells/mm3 (normal range: 0–5) with 90% lymphocytes, IgG (CSF) 19.40 mg/dl, albumin (CSF) 114 mg/dl, and glucose (CSF) 37 mg/dl. The increase in the white cell count, IgG, and albumin in the CSF can be explained by the ineffective therapeutic approach. AFB were detected in the CSF using Ziehl-Neelsen staining (positive; Fig. 1), and PCR performed using CSF was positive for Mycobacterium TB complex. After 15 days of incubation, the culture for the same sample of CSF was positive, confirming that the bacteria were alive and that therapy was ineffective. After 1 month, drug resistance data were available: testing of susceptibility to first-line agents showed resistance to isoniazid, rifampicin, and streptomycin, and the strain was identified as MDR. The treatment was changed to ethambutol, prednisone, pyrazinamide, and amikacin at the same dosages as previously described for 2 months; ciprofloxacin (os daily dosage 30 mg/kg); and 10 days later, ethionamide (os daily dosage 20 mg/kg). In the absence of other available drugs, it was decided to administer ciprofloxacin; the use of ciprofloxacin is no longer recommended but may be necessary to treat a life-threatening disease such as MDR-TB meningitis. CSF taken 5 days after the beginning of treatment was negative for mycobacterial growth (the culture was incubated for 6 weeks). The mycobacterial cultures of CSF were repeated three more times and were always negative. A ventricular peritoneal shunt was performed to treat the hydrocephalus.
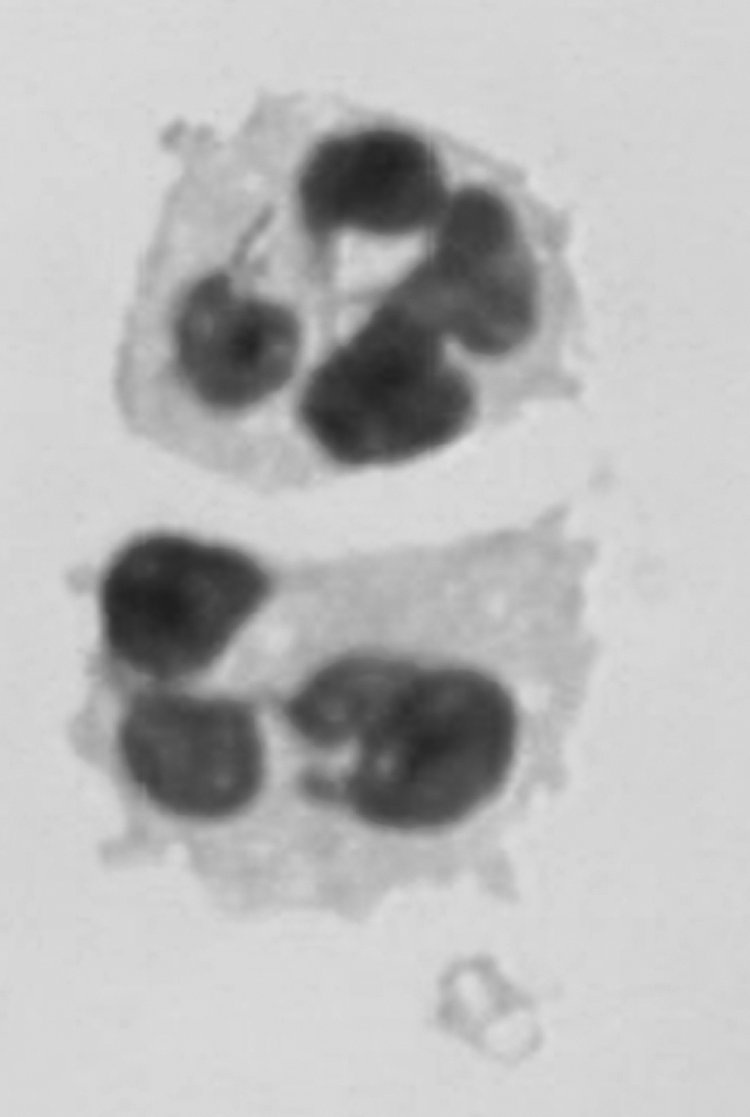
Acid-fast bacilli from cerebrospinal fluid visualized by Ziehl-Neelsen staining.
TB in young children (under 5 years old) is often transmitted from a household member. Upon diagnosis, the parents were interviewed and asked to describe the daily activities and routines of the child at home and in his social environment. The TSTs of parents were negative. The parents were not aware of any contact with TB patients. The source of the transmission of TB to children through nonhousehold exposure is difficult to determine. Twenty days before, the child had been hospitalized in northern Italy because of surgical treatment of varicocele; it is probable that during the time in the hospital or during the flight he may have had contact with MDR-TB.
The PCR test is an important tool that has strongly supported the clinical suspicions in the early stage of infection, because the detection of AFB by Ziehl-Neelsen staining is rare in patient with
To date, the child had not experienced any sequelae, but continued maintenance therapy for 9 months. The maintenance therapy consisted of ciprofloxacin, pyrazinamide, and ethionamide.
Footnotes
Disclosure Statement
No competing financial interests exist.