
Abstract
To define the risk factors and clinical outcomes of community-onset bacteremia caused by extended-spectrum β-lactamase (ESBL)-producing Escherichia coli (ESBLEC), we analyzed 50 consecutive cases of community-onset bacteremia caused by ESBLEC at a secondary hospital in South Korea from 2005 to 2010. Risk factors were assessed by conducting a case-double control study in which cases were compared with (1) control patients with community-onset bacteremia due to non-ESBLEC, and (2) those with community-onset bacteremia not caused by E. coli. Clinical outcome was assessed among patients with community-onset E. coli bacteremia. Community-onset bacteremia due to ESBLEC accounted for 6.7% of all community-onset E. coli bacteremia. In addition, an increasing proportion of ESBLEC among patients without any healthcare risk factors was observed. Comparison with both control groups revealed that the recent use of antibiotics (odds ratio [OR], 4.3; 95% confidence interval [CI], 1.5–12.3) was an independent risk factor for ESBL acquisition. Factors influencing the 30-day mortality were a high Acute Physiology and Chronic Health Evaluation (APACHE) II score (OR, 1.5; 95% CI, 1.1–2.0) and severe sepsis or septic shock (OR, 26.6; 95% CI, 1.5–470.7) and malignancy (OR, 11.9; 95% CI, 1.1–134.8). Increased mortality was not statistically associated either with ESBL production or with inappropriate empirical therapy. ESBLEC has emerged as a significant cause of community-onset bacteremia in this hospital, suggesting that ESBLEC are widely disseminated in the South Korean community.
Introduction
Materials and Methods
Study design and patients
This retrospective cohort study was conducted at Daejeon St. Mary's hospital, a 560-bed university-affiliated, secondary care, community-based hospital located in Daejeon, South Korea. Daejeon has a population of 1.5 million people and this hospital has around 20,450 admissions per year. The microbiology database was retrieved from the clinical microbiology laboratories in order to identify the patients with community-onset bacteremia due to E. coli and other pathogens.
The risk factors for community-onset bacteremia due to ESBLEC were evaluated using a case-double control design.20,22 The case patient group included all the episodes of community-onset bacteremia caused by ESBLEC that were diagnosed at this hospital during the period from January 2005 through December 2010 (hereafter referred to as the ESBLEC group). The case patients were compared with two groups of controls selected from two base populations: (I) the community-onset E. coli bacteremia population and (II) the community-onset bacteremia of all causes population. Control group I included patients who were selected from the population of community-onset bacteremia due to non-ESBL-producing E. coli (hereafter referred to as the non-ESBLEC group) diagnosed during the same or following month as the corresponding case patient. Control group II was composed of patients selected from the population with community-onset bacteremia of all causes, provided that E. coli proved not to be the cause of bacteremia, diagnosed during the same month as the corresponding case patient (hereafter referred to as the community-onset bacteremia group) (Fig. 1). Control patients were selected by computer generated random number sampling using the culture register numbers in the microbiology laboratory of this hospital.
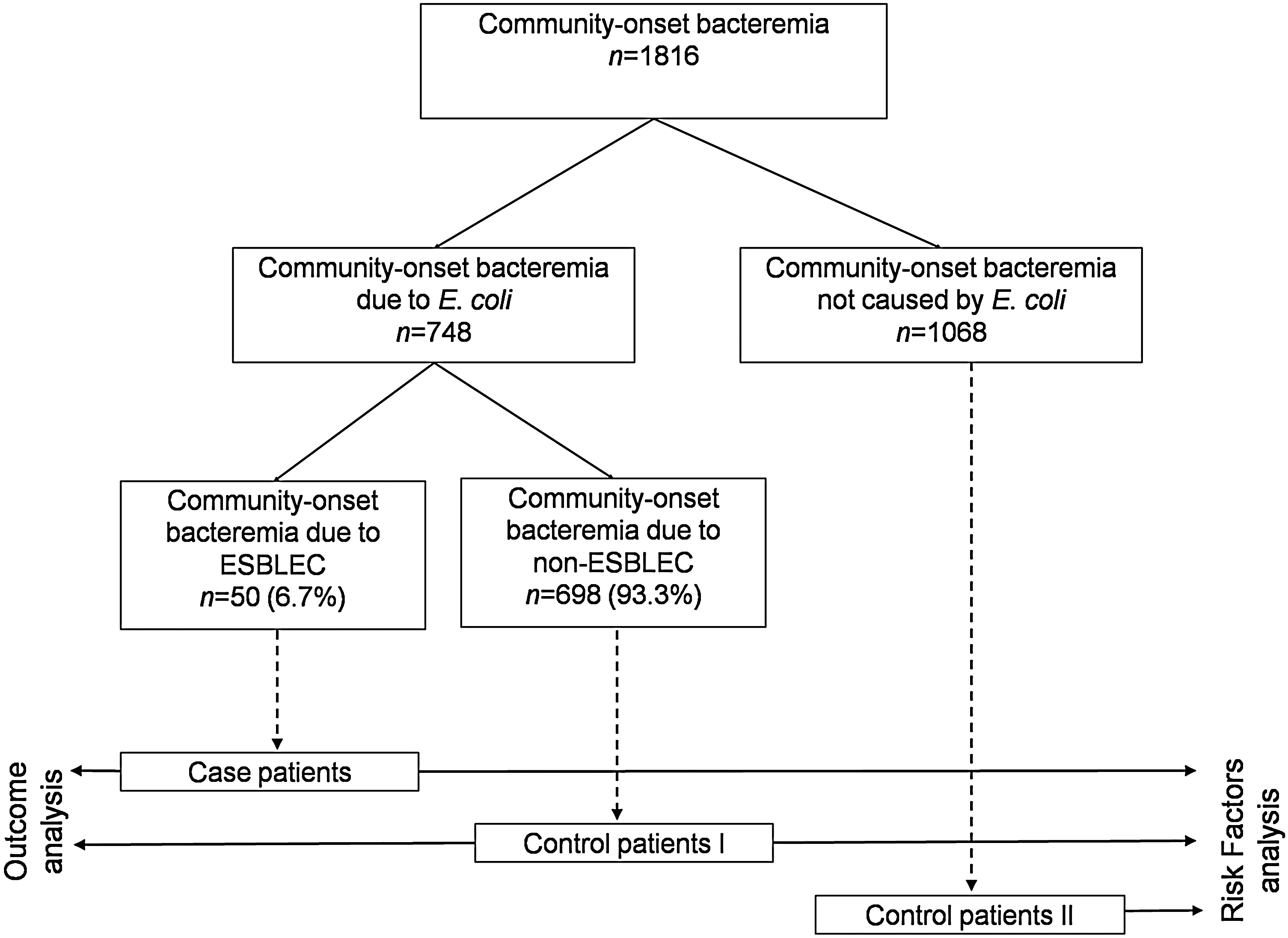
Overview of patient cohorts and base populations of the study. ESBLEC, extended-spectrum β-lactamase-producing Escherichia coli.
The clinical features and outcomes of community-onset bacteremia due to ESBLEC were analyzed by comparison with those of control group I (non-ESBLEC group). The main outcome measured was the 30-day mortality rate. We also compared survivor and nonsurvivor subgroups to determine the factors influencing mortality. This study was approved by the ethics committee of our hospital (DC 10EBSI0001).
Microbiology
Species identification and susceptibility tests were performed with the MicroScan NegCombo Panel Type 32 (Dade Behring, Sacramento, CA) in accordance with the manufacturer's instruction. ESBL production was confirmed by the double disk synergy test as described by the Clinical Laboratory Standards Institute. 4 In brief, disks containing 30 μg of cefotaxime and ceftazidime, either alone or coupled with 10 μg of clavulanate (Oxoid Ltd., Cambridge, United Kingdom), were placed at distances of 20 mm (center to center). When the inhibition zone differed by ≥5 mm between at least one of the combination disks and its corresponding single antibiotic disk, the strain was identified as an ESBL producer.
Definitions
Cases of bacteremia were defined as a community-onset when a positive blood culture was obtained at the time of hospital admission or <48 hours after hospitalization. The patients, who had been hospitalized within 2 weeks before admission or who had been transferred from other hospitals, were defined as having nosocomial infections. Episodes of community-onset bacteremia were classified as healthcare-associated if any of the following criteria were present. (1) The patient received intravenous therapy, wound care, or specialized nursing care at home or in a day hospital during the 30 days before bacteremia, including the performance of urinary or digestive tract endoscopy or other invasive procedures. (2) The patient attended a hospital or hemodialysis clinic within the 30 days before bacteremia. (3) The patient was hospitalized for >2 days in an acute care hospital or the patient resided in a nursing home or long-term care facility during the year before bacteremia. Otherwise, the cases were considered to be strictly community associated.6,20
Empirical antimicrobial therapy was considered appropriate when the treatment regimen that included at least one active antimicrobial agent to which the organism was susceptible in vitro at the recommended doses was initiated during the first 24 hours after the blood sample was obtained; otherwise, it was considered inappropriate. 23 Oxyimino-β-lactams (cefotaxime, ceftriaxone, ceftazidime, and aztreonam) were considered inappropriate regardless of susceptibility. 12
The following variables were collected by reviewing the medical records: age, gender, the comorbidities and the severity of any underlying conditions according to the Charlson comorbidity index, 3 surgery or invasive procedures performed during the preceding 30 days, receipt of antimicrobial agents during the preceding 3 months, the source of bacteremia, the presence of severe sepsis or septic shock at presentation, 2 the severity of illness at presentation according to the Acute Physiology and Chronic Health Evaluation (APACHE) II score, 14 antimicrobial treatment, and mortality. Among the primary foci of infection, skin and soft tissue, bone and joint, and lung, gastrointestinal, or genitourinary infection was defined on the basis of a previous definition 10 ; catheter-related infection was defined according to the Infectious Diseases Society of America (IDSA) guidelines. 9 Primary bacteremia was defined as conditions in which no primary focus could be determined.
Statistical analysis
Data analysis was performed using SPSS software, version 12.0 (SPSS). Statistical significance was assessed via the chi-square test or Fisher's exact test for the categorical variables and Student t test or the Mann–Whitney U-test for the continuous variables. Logistic regression analysis was used for the multivariate analysis. Variables achieving a probability of less than 0.2 by univariate analyses were introduced into the multivariate analysis to determine the different factors in the two groups independently. Variables were selected using a stepwise backward process. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. All P-values were two-tailed and a P-value of <0.05 was considered statistically significant.
Results
Incidence and risk factors for community-onset bacteremia caused by ESBL-producing E. coli
A total of 748 episodes of community-onset E. coli bacteremia were identified during the study period. Among them, 50 episodes (6.7%) were caused by ESBLEC (Fig. 1) and the percentage of ESBL producers among the E. coli isolates causing community-onset bacteremia increased over time from 1.2% (1/84) in 2005 to 10.2% (17/167) in 2010. The distribution of cases throughout the study period is shown in Fig. 2. Among the community-onset bacteremia caused by ESBLEC, 29 episodes (58%) were healthcare-associated and 21 cases (42%) were considered strictly community-associated. We observed an increasing rate of bacteremia due to ESBLEC in the patients without any healthcare risk factors (Fig. 2).
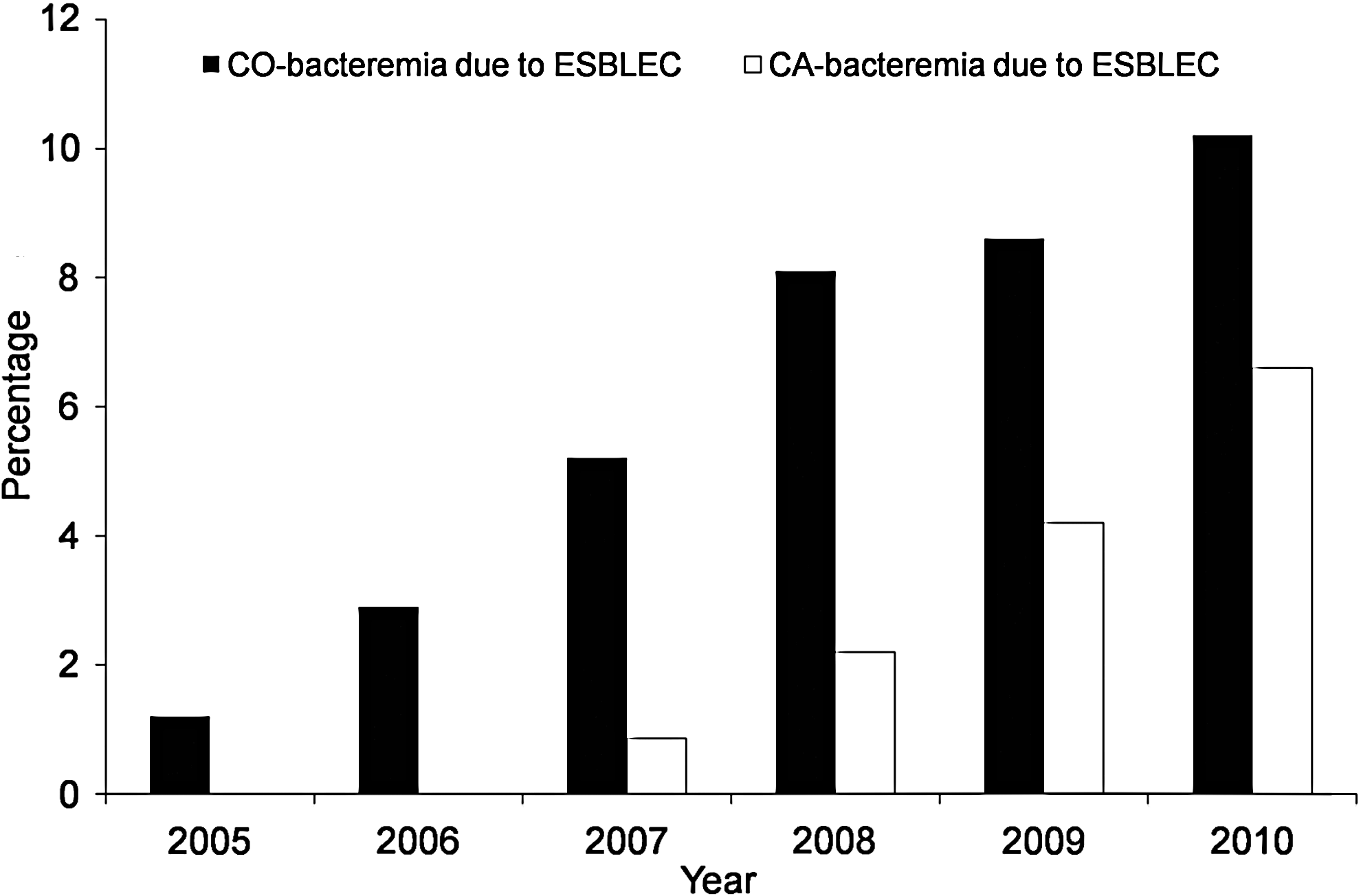
Distribution of community-onset bacteremia (CO-bacteremia) and community-associated bacteremia (CA-bacteremia) due to ESBLEC.
The demographic and clinical characteristics of the case and control patients are shown in Table 1. Each control group consisted of 100 patients. The results of the univariate analysis are shown in Table 1. The risk factors common to both populations according to the univariate analysis were healthcare-associated infections, the presence of malignancy or chronic kidney disease, and the recent use of antibiotics. Multivariate analysis revealed that the recent use of antibiotics was the only independent risk factor for community-onset bacteremia caused by ESBLEC in both populations. Healthcare-associated infection was identified as an independent risk factor only in the community-onset E. coli bacteremia population, whereas female gender and the presence of obstructive urinary diseases were independent risk factors for the acquisition of ESBLEC in the community-onset bacteremia population. The results of multivariate analysis of the variables in each population are summarized in Table 2.
CI, confidence interval; OR, odds ratio; IV, intravenous; COPD, chronic obstructive pulmonary disease; CCI, Charlson comorbidity index.
Clinical features and outcomes of community-onset bacteremia caused by ESBL-producing E. coli
The clinical characteristics of the case patients are shown and compared with those of the control patients in the community-onset E. coli bacteremia population in Table 3. The source of bacteremia did not significantly differ between the case patients and control patients in this population. The 30-day mortality rate was higher for the patients with community-onset bacteremia due to ESBLEC than for those patients with community-onset bacteremia due to non-ESBLEC, although this difference was not statistically significant. However, the patients with ESBLEC were more likely to receive inappropriate empirical therapy than those patients with non-ESBLEC bacteremia. The comorbidity index and the APACHE II score were also higher in the patients with ESBLEC.
APACHE II score, Acute Physiology and Chronic Health Evaluation II score; ESBLEC, nonextended-spectrum β-lactamase-producing Escherichia coli; UTI, urinary tract infection.
However, comparison between survivor and nonsurvivor groups using multivariate analysis revealed that the independent risk factors for mortality were a higher APACHE II score, severe sepsis, or septic shock at the time of presentation, and the presence of malignancy (Table 4). In this study, increased mortality was not significantly associated with either ESBL production or inappropriate empirical therapy. Further sub-analysis was performed for the ESBLEC and non-ESBLEC groups, respectively, and it demonstrated that the mortality rate was not significantly different between the patients treated with inappropriate empirical therapy and those treated with appropriate therapy in each group: 7/33 vs. 2/17 for the patients with ESBLEC (p=0.410; OR, 2.02; 95% CI, 0.37–10.99); 0/9 vs. 8/91 for the patients with non-ESBLEC (p=0.354). Among patients with community-onset bacteremia caused by ESBLEC, mortality occurred only in the patients with healthcare-associated bacteremia (HA-bacteremia), whereas no death was observed in those patients with community-associated bacteremia (CA-bacteremia), even though there was no difference in the rate of inappropriate empirical therapy (14/21, 66.7% vs. 19/29, 66.5%, respectively; p=0.93). For the patients with CA-bacteremia due to ESBLEC, the APACHE II score was lower than for HA-bacteremia patients (mean 10.1±4.6 vs. 14.9±7.8, respectively; p=0.015) and the urinary tract was more frequent primary site of infection (18/21, 85.7% vs. 16/29, 55.2%, respectively; p=0.022; OR, 4.9; 95% CI, 1.2–20).
Antimicrobial susceptibility of ESBL–producing E. coli
The antimicrobial resistance rates of ESBLEC were 4% for amikacin, 30% for gentamicin, 38% for tobramycin, 12% for piperacillin/tazobactam, 54% for ciprofloxacin, and 44% for trimethoprim/sulfamethoxazole. None of them were resistant to meropenem or imipenem.
Discussion
This study showed that ESBLEC has been increasingly identified as a cause of community-onset bacteremia. Although the incidence of bacteremia caused by ESBLEC in patients without any healthcare risk factors was still low (21/748, 2.8%), the incidence and the number of the overall community-onset bacteremia cases caused by ESBLEC have increased over time.
Previous use of antibiotics has been recognized as a major risk factor for the development of bacterial resistance. When analyzing the risk factors for acquisition of drug resistant bacteria, the risk of antibiotic therapy was often exaggerated when comparing the patients with infections caused by resistant bacteria to those patients with infections caused by nonresistant bacteria. 8 To avoid this limitation, we adopted a case-double control design, which has been proven useful in previous studies.20,22 In this study, the risk factors identified for both the community-onset bacteremia and community-onset E. coli bacteremia populations by using univariate analysis were healthcare-associated infections, malignancy, chronic kidney disease, and the recent use of antibiotics. Among these, the recent use of antibiotics was identified as an independent risk factor for community-onset bacteremia caused by ESBLEC in both populations. This study confirmed that previous exposure to antibiotics was still an independent risk factor for the acquisition of ESBLEC even in the community-onset bacteremia population.
In the community-onset E. coli bacteremia population, the most frequent site of infections was UTIs, followed by intra-abdominal or hepatobiliary tract infections. In contrast to the previous multicenter study in Korea, which demonstrated that primary bacteremia was an independent variable associated with community-onset bacteremia due to ESBLEC, 13 there was only one case of primary bacteremia caused by ESBLEC in this study. This difference might have resulted from the differences in the geographic areas and study populations according to the hospitals where the studies were conducted. This study was conducted in a community-based secondary hospital in only one region, whereas the previous study was performed in tertiary, large referral hospitals in different areas. However, while facing the increasing incidence of UTI caused by ESBLEC among nonhospitalized patients worldwide,18,19,21 it appears to be implausible to conclude that ESBL-producing E. coli should be suspected in patients with Gram-negative bacteremia if the primary foci are not identified.
In the current study, the initial presentation with severe sepsis or septic shock, a higher APACHE II score and the presence of malignancy were the risk factors independently associated with mortality. Previous studies have suggested that the increased mortality rate in patients with community-onset bacteremia caused by ESBL producers was largely attributable to delayed administration of adequate therapy in patients with ESBL producers, and not ESBL production per se.11,20,25 However, although higher mortality was observed for the patients in the ESBLEC group and the patients treated with inappropriate empirical therapy, neither ESBL production by E. coli nor inappropriate empirical therapy was identified as significant predictors of mortality in this study. When the ESBLEC group and non-ESBLEC group patients were separately analyzed, inappropriate empirical therapy was not associated with increased mortality regardless of ESBL production. Among the ESBLEC group patients, mortality occurred only in patients with HA-bacteremia, whereas no death was observed in those patients with CA-bacteremia. The clinical presentation was less severe, and UTI, which has a low mortality rate, 11 was a more common primary site of infection in patients with CA-bacteremia due to ESBLEC than in those patients with HA-bacteremia. This might explain the lack of mortality in patients with community-associated ESBLEC despite the delay in appropriate therapy among more than half of them, and this might have lowered the statistical power to detect the association between inappropriate empirical therapy and increased mortality. In addition, the severity of illness was significantly higher for the patients who died despite timely receipt of empirical therapy than that in those patients who died with inappropriate empirical therapy (mean APACHE II score 28.5±4.7 vs. 19.9±5.6, respectively, p=0.004). In this regard, it is important to relate the consequences of delayed treatment to individual patients and their risk factors despite the undoubtedly negative impact of inappropriate therapy on the mortality of patients with invasive infections due to resistant bacteria. 5
Carbapenem is considered the treatment of choice for invasive infections caused by ESBL-producing bacteria. 17 Because of the emergence of carbapenem resistance among the Gram-negative bacteria worldwide, the increasing rate of community-onset infection caused by ESBLEC raises serious conflicting issues: the need to use carbapenem when ESBLEC is suspected versus the need to avoid the overuse of carbapenem so as to contain resistance. To overcome this dilemma, the empirical treatment of carbapenem can be suggested only for the patients who present with severe sepsis or septic shock due to UTI or intra-abdominal infections and who have risk factors for ESBLEC. Moreover, use of amikacin as an adjunctive therapy to a β-lactam or fluoroquinolone can be an alternative option for empirical therapy when ESBL production is a concern in patients with urinary tract sepsis because resistance to amikacin in ESBLEC is still low.7,15,16 However, the efficacy of amikacin against ESBL producers has not yet been evaluated much and this needs further evaluation.
This study has some limitations that should be acknowledged. First, it was performed in a single institution. Thus, the study results may not reflect the epidemiology of different centers and/or different geographic areas. Despite this limitation, the rising incidence of community-onset bacteremia due to ESBLEC was observed in this community hospital, and this corresponds to the epidemiologic change worldwide. This study suggests the need for a nation-wide survey on the epidemiology of ESBLEC in community settings. Second, we could not include all patients in the control groups because of the higher number of patients with community-onset bacteremia due to E. coli. However, the control patients were randomly selected among those patients who were matched to the case patients on the basis of the time period. In the community-onset E. coli bacteremia population, the age distribution, gender difference, and clinical outcomes were similar between the control patients and the patients with community-onset bacteremia due to non-ESBLEC. Therefore, the possible selection bias might be small in this study.
In summary, ESBLEC has become increasingly detected as a cause of community-onset bacteremia in our community hospital. The recent use of antibiotics was an independent risk factor for acquiring ESBLEC. The clinical outcomes were significantly affected by the severity of the initial presentation of patients or the presence of malignancy, rather than by ESBL production or inappropriate empirical therapy. Given the spread of ESBLEC into the wider population, ESBLEC bacteremia is likely to increase in patients with no recent healthcare contact. This can be a great challenge to clinicians and to public health in the face of the rising rate of resistance to carbapenem. In this regard, judicious use of antibiotics in the community and appropriate public health control measures are needed to reduce the spread of ESBLEC in the community. Further research on the alternative treatment options for ESBLEC is certainly warranted.
Footnotes
Acknowledgments
This study was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A090760).
Disclosure Statement
All authors report no conflicts of interest relevant to this article.