
Abstract
Introduction
The essential oils of thyme, oregano, mint, cinnamon, cumin, salvia, clove, and eucalyptus have been found to possess the strongest antimicrobial properties. 33 Many of them appear to have a wide spectrum of antibiotic activity against microflora that provokes hospital-acquired infections. The broad and complex activity of essential oils, as well as their synergy of action, can make them a valued weapon against multidrug resistant bacterial strains. What is more, there is no evidence of emergence of resistant bacteria after their usage, and this is highly promising in the treatment of human diseases.25,34,43,49
The aim of the study
The aim of this work was to investigate the antimicrobial properties of thyme essential oil obtained from thyme (Thymus vulgaris L.) against standard and clinical strains of bacteria isolated from patients, clinical staff, and the hospital environment.
Materials and Methods
Bacterial strains
The standard strains, Staphylococcus aureus ATCC 433000, Enterococcus faecalis Van B ATCC 51299, En. faecalis, vancomycin VA-sensitive ATCC 29212, Enterococcus faecium, VA-sensitive ATCC 35667, Enterococcus durans, VA-sensitive ATCC 6656, Escherichia coli ATCC 25922, and Pseudomonas aeruginosa ATCC 27853 came from the collection of the Medical and Sanitary Microbiology Department, Medical University of Lodz.
The clinical strains of Staphylococcus, Enterococcus, Escherichia, and Pseudomonas genera were collected from different materials originating from patients and medical staff, as well as the environment of various wards from two hospitals in Lodz: internal diseases, surgery, urology, laryngology, and intensive care unit. Bacterial strains were isolated from abdominal cavity exudates (n=4), bronchial secretions (n=5), nose (n=9), ear (n=3), pharynx (n=6), hands (n=2), ulcers (n=14), wounds (n=22), bedsores (n=12), abscesses (n=1), groin (n=5), bile (n=1), toe (n=1), anus (n=6), sputum (n=1), blood (n=2), urine (n=14), drains (n=2), hospital staff (n=2), disinfecting dispensers (n=2), hospital beds (n=2), and cupboard swabs (n=4).
Bacterial strain identification
S. aureus strains were identified to the genus according to standard microbiological methods: culturing on Columbia Agar (bioMerieux) with 5% blood, culturing on Mannitol Salt Agar (bioMerieux), using Slidex-Staph Kit (bioMerieux), and determining the ability of bacteria to produce catalase and coagulase (bioMerieux). Microorganisms were identified to the species by using API 20 Staph tests (bioMerieux). Bacteria were incubated at 37°C for 24 hours. S. aureus ATCC 29213 strain was used as a control.
Enterococci were identified to the genus according to standard microbiological methods: culturing on Columbia Agar (bioMerieux) with 5% sheep blood, culturing on Enterococcosel Agar (Emapol), determining the presence of D antigen according to Lancefield (Slidex-Strep Kit, bioMerieux), and determining the ability of bacteria to produce catalase, pyrrolidonyloarylamidase (Lachema). The microorganisms were identified to the species by using API 20 Strep tests (bioMerieux). The bacteria were incubated at 37°C for 24 hours. As a control, En. faecalis Van B ATCC 51299, En. faecalis ATCC 29212, En. faecium ATCC 35667, and En. durans ATCC 6656 strains were used.
Es. coli strains were identified according to standard microbiological methods such as culturing on Columbia Agar (bioMerieux) with 5% blood and culturing on Mac Conkey Agar (bioMerieux) and were identified to the species by using API 20 E tests (bioMerieux). Bacteria were incubated in 37°C for 24 hours. As a control, Es. coli ATCC 25922 strain was used.
P. aeruginosa strains were identified according to standard microbiological methods including culturing on Agar and Columbia Agar (bioMerieux) with 5% blood, culturing on Mac Conkey Agar (bioMerieux), and determining the ability of the bacteria to produce oxidase (bioMerieux). The microorganisms were identified in the species by using API 20 NE tests (bioMerieux). The bacteria were incubated in 37°C for 24 hours. As a control, P. aeruginosa ATCC 27853 strain was used.
Essential oil analysis
Commercial essential oil from thyme—T. vulgaris L. (Lamiaceae) was purchased from the manufacturer (POLLENA-AROMA) and analyzed by GC-FID-MS in the Institute of General Food Chemistry, Technical University of Lodz, using a Trace GC Ultra apparatus (Thermo Electron Corporation) MS DSQ II detectors and FID-MS splitter (SGE). Operating conditions: apolar capillary column Rtx-1 ms (Restek), 60 m×0.25 mm i.d., film thickness 0.25 μm; temperature program, 50°C–300°C at 4°C/minute; SSL injector temperature 280°C; FID temperature 300°C; split ratio 1:20; carrier gas helium at a regular pressure 200 kPa.; FID temperature 260°C; carrier gas, helium; 0.5 ml/min; split ratio 1:20. Mass spectra were acquired over the mass range of 30–400 Da, ionization voltage of 70 eV, and ion source temperature of 200°C.
Identification of components was based on the comparison of their MS spectra with those of the laboratory-made MS library, commercial libraries (NIST 98.1, Wiley Registry of Mass Spectral Data, 8th Ed. and MassFinder 3.1) and with literature data1,31 along with the retention indices on apolar column (Rtx-1, MassFinder 3.1) associated with a series of alkanes with linear interpolation (C8-C26). A quantitative analysis (expressed as percentages of each component) was carried out by peak area normalization measurements without correction factors.
The standard and clinical strains were cultivated in Columbia agar medium and incubated at 37°C for 48 hours in aerobic conditions. Bacterial suspensions with an optical density of 0.5 on the Mc Farland scale were prepared and analyzed with a Bio Merieux densitometer.
The antibacterial properties of the tested oil were investigated by agar dilution. The essential oil was diluted in ethanol. This solution was mixed with a nutrient broth to obtain concentrations from 0.03125 to 2.5 μl/ml and poured into petri dishes. Inoculum containing 1.5·108 CFU (0.1 ml) per spot was seeded on the surface of the agar with various oil concentrations, as well as on agar with no oil added (strains growth control). Minimal inhibitory concentration (MIC) was determined after 24 hours of incubation at 37°C in aerobic conditions. The analysis of the antibacterial activity of the oil was performed thrice independently.
Susceptibility testing
The following antibiotics (Becton Dickinson) were used for susceptibility testing of S. aureus strains: cefoxitin (FOX; 30 μg) (R≤14, 15≤I≤17, S≥18), erythromycin (E; 15 μg) (R≤13, 14≤I≤22, S≥23), clindamycin (CC; 2 μg) (R≤14, 15≤I≤20, S≤21), nitrofurantoin (F/M; 300 μg) (R≤14, 15≤I≤16, S≥17) (for isolates from urine), VA (30 μg) (S≥15), teicoplanin (TEC; 30 μg) (R≤10, 11≤I≤13, S≥14), tetracycline (TE; 30 μg) (R≤14, 15≤I≤18, S≥19), chloramphenicol (C; 30 μg) (R≤12, 13≤I≤17, S≥18), ciprofloxacin (CIP; 5 μg) (R≤15, 16≤I≤20, S≥21), trimethoprim/sulfamethoxazole (SXT; 1.25 μg/23.75 μg) (R≤10, 11≤I≤15, S≤16), fusidic acid (FA; 10 μg) (S≥22), linezolid (LZD; 30 μg) (S≥21); of Enterococcus genus:
Ampicillin (AM; 10 μg) (R≤16 S≥17), C (30 μg) (R≤12, 13≤I≤17, S≥18), CIP (5 μg) (R≤15, 16≤I≤20, S≥21), E (15 μg) (R≤13, 14≤I≤22, S≤I≤23), fosfomycin (FOS; 200 μg) (R≤12, 13≤I≤15, S≥16) (only for En. faecalis, the isolates from urine), F/M (300 μg) (R≤14, 15≤I≤16, S≥17) (for isolates from urine), gentamicin (GM; 120 μg) (R≤6, 7≤I≤9, S≥10), LZD (30 μg) (R≤20, 21≤I≤22, S≥23), imipenem (IPM; 10 μg) (R≤13, 14≤I≤15, S≥16), penicillin (P; 10 μg) (R≤14, S≥15), streptomycin (S; 300 μg) (R≤6, 7≤I≤9, S≥10), synercid (SYN; 4.5 μg/10.5 μg) (R≤15, 16≤I≤18, S≥19) (only for En. faecium), TE (30 μg) (R≤14, 15≤I≤18, S≥19), TEC (30 μg) (R≤10, 11≤I≤13, S≥14), VA (30 μg) (R≤14, 15≤I≤16, S≥17), of Es. coli strains: amoxicillin/clavulanic acid (AMC; 20 μg/10 μg) (R≤13, 14≤I≤17, S≥18), cefalotin (CF; 30 μg) (R≤14, 15≤I≤17, S≥18), cefazolin (CZ; 30 μg) (R≤14, 15≤I≤17, S≥18), cefuroxime (CXM; 30 μg) (R≤14, 15≤I≤17, S≥18), GM (10 μg) (R≤12, 13≤I≤14, S≥15), AM (10 μg) (R≤13, 14≤I≤16, S≥17) (only for the isolates from urine), norfloxacin (NOR; 10 μg) (R≤12, 13≤I≤16, S≥17) (as above), F/M (300 μg) (R≤14, 15≤I≤16, S≥17) (as above), FOX (30 μg) (R≤14, 15≤I≤17, S≥18), cefotaxim (CTX; 30 μg) (R≤14, 15≤I≤22, S≥23), ceftazidime (CAZ; 30 μg) (R≤14, 15≤I≤17, S≥18), aztreonam (ATM; 30 μg) (R≤15, 16≤I≤21, S≥22), IPM (10 μg) (R≤13, 14≤I≤15, S≥16), CIP (5 μg) (R≤15, 16≤I≤20, S≥21), netilmicin (NET; 30 μg) (R≤12, 13≤I≤14, S≥15), tobramycin (NN; 10 μg) (R≤12, 13≤I≤14, S≥15), C (30 μg) (R≤12, 13≤I≤17, S≥18), TE (30 μg) (R≤14, 15≤I≤18, S≥19), SXT (1.25 μg/23.75 μg) (R≤10, 11≤I≤15, S≥16) and of P. aeruginosa strains: mezlocillin (MZ; 75 μg) (R≤17, 18≤I≤20, S≥21), piperacillin (PIP; 100 μg) (R≤17, 18≤I≤20, S≥21), CAZ (30 μg) (R≤14, 15≤I≤17, S≥18), GM (10 μg) (R≤12, 13≤I≤14, S≥15), NN (10 μg) (R≤12, 13≤I≤14, S≥15), AMC (20 μg/10 μg) (R≤13, 14≤I≤17, S≥18), piperacillin/tazobactam (TZP; 100 μg/10 μg) (R≤17, 18≤I≤20, S≥21), CTX (30 μg) (R≤14, 15≤I≤22, S≥23), ATM (30 μg) (R≤15, 16≤I≤21, S≥22), IPM (10 μg) (R≤13, 14≤I≤15, S≥16), meropenem (MEM; 10 μg) (R≤13, 14≤I≤15, S≥16), NET (30 μg) (R≤12, 13≤I≤14, S≥15), CIP (5 μg) (R≤15, 16≤I≤20, S≥21), SXT (1.25 μg/23.75 μg) (R≤10, 11≤I≤15, S≥16), C (30 μg) (R≤12, 13≤I≤17, S≥18), and colistin (CL; 50 μg) (R<15, S>15). Susceptibility testing was carried out using the disk-diffusion method, on Mueller-Hinton II Agar. Cultures were incubated at 37°C for 16–18 hours, VA for 24 hours. The results were interpreted according to Clinical and Laboratory Standard Institute guidelines. 9
Results
Chemical composition of the tested oil
The composition of the essential oil derived from T. vulgaris was found to meet the requirements of the Polish Pharmacopoeia VIII and the European Pharmacopoeia.18,40 The content of thymol amounts to 38.1% and carvacrol to 2.3%, as well as other prevailing compounds such as p-cymene (29.1%), γ-terpinene (5.2%), and linalool (3.7%). The chemical composition of the tested oil is shown in Table 1.
Bold texts and values indicate the major constituents of thyme oil.
Susceptibility testing
The tested strains of S. aureus were resistant to 50% of β-lactams and macrolides recommended for susceptibility testing. Clinical strains of the Enterococcus genus showed resistance to macrolides in almost 70%, to β-lactams and aminoglycosides in 60%, and to carbapenems in 40%. The examined Es. coli strains were resistant to β-lactams in 40% and to aminoglycosides in 20%. The tested P. aeruginosa strains were resistant to β-lactams in more than 50%, to carbapenems in 30%, and to aminoglycosides and monobactams in 20%. The results are shown in Tables 2–5.
FOX, cefoxitin; E, erythromycin; CC, clindamycin; F/M, nitrofurantoin; VA, vancomycin; TEC, teicoplanin; TE, tetracycline; C, chloramphenicol; CIP, ciprofloxacin; SXT, trimethoprim/sulfamethoxazole; FA, fusidic acid; LZD, linezolid; R, resistant; I, intermediate susceptible strain; S, susceptible strain; MIC, minimal inhibitory concentration.
AM, ampicillin; FOS, fosfomycin; GM, gentamicin; IPM, imipenem; LZD, linezolid; P, penicillin; S, streptomycin; SYN, synercid.
AMC, amoxicillin/clavulanic acid; CF, cefalotin; CZ, cefazolin; CXM, cefuroxime; NOR, norfloxacin; CTX, cefotaxim; CAZ, ceftazidime; ATM, aztreonam; NET, netilmicin; NN, tobramycin.
MZ, mezlocillin; PIP, piperacillin; TZP, piperacillin/tazobactam; MEM, meropenem.
The activity of thyme oil against tested bacterial strains
The MIC for S. aureus were between 0.25 and 1.0 μl/ml. MIC was 0.25 μl/ml for the standard strain of S. aureus ATCC 433000 and 6 strains from the clinical material. The results are shown in Figure 1.
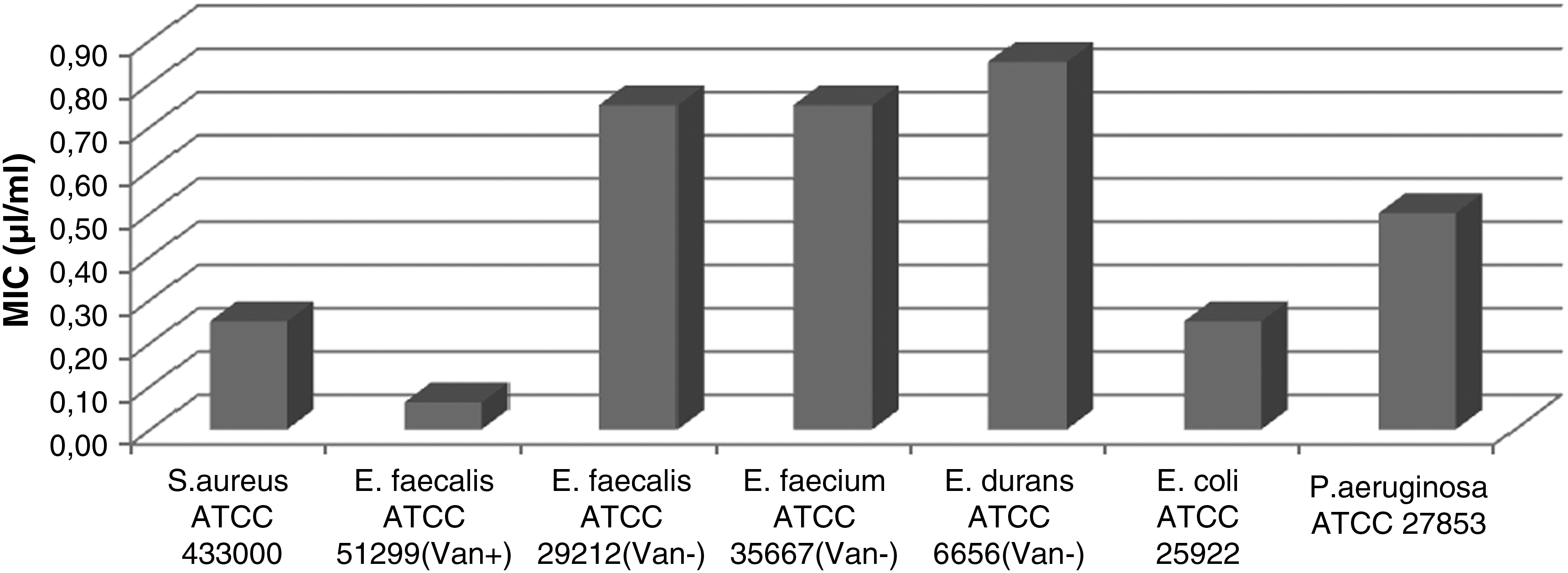
Standard strains susceptibility to thyme essential oil. MIC, minimal inhibitory concentration.
Most Staphylococcus strains were sensitive to oil at a concentration of 0.5 μl/ml. Growth inhibition was obtained in 17 out of the 30 clinical bacterial strains. Isolates were taken from the nose (n=5), ear (n=1), hand (n=2), wound (n=3), abdominal cavity (n=1), groin (n=1), ulcer swabs (n=3), and urine (n=1). The results are presented in Figure 2.

Clinical strains of Staphylococcus aureus, Enterococcus sp., Escherichia coli, and Pseudomonas aeruginosa susceptibility to thyme essential oil.
The tested clinical strains of S. aureus, resistant to many antibiotics, were sensitive to the thyme oil at low concentrations. S. aureus strain isolated from abscesses was resistant to 7 out of 11 tested antibiotics (sensitive to VA, TEC, C, and LZD); the MIC value for the thyme oil was 0.25 μl/ml. The MIC for highly multidrug resistant bacterial strains from the hand, wound, ear, foot ulceration, exudates from episiotomy wounds, stump ulcers, and urine ranged from 0.5 μl/ml to 0.75 μl/ml. Thyme oil at 0.5 μl/ml concentration inhibited the growth of more than 45% of the resistant strains. Table 2 shows the general characteristics of S. aureus isolates.
The VA resistant standard strain—En. faecalis Van B ATCC 51299 was the most sensitive strain to thyme essential oil (MIC–0.0625 μl/ml). The MIC was 0.75 μl/ml for VA sensitive strains of En. faecalis ATCC 29212 and En. faecium ATCC 35667 and MIC for the standard strain of En. durans ATCC 6656 was 0.85 μl/ml. The results are shown in Figure 1.
Thyme oil was also very active against clinical strains, the most active against En. faecium strain being isolated from the ulcer (MIC–0.25 μl/ml); it significantly inhibited 16 clinical strains at a concentration of 0.75 μl/ml and 11 clinical strains at 0.5 μl/ml. The results are shown in Figure 2.
An MIC value of−0.5 μl/ml was characteristic for all strains of En. faecalis and En. faecium isolated from urine, and En. faecalis strains derived from the hospital environment. The concentration of 0.75 μl/ml inhibited the growth of En. faecalis clinical strains from wounds and the throat, as well as of En. faecium strains from blood and from the hospital environment.
It was found that most clinical resistant strains of enterococci were sensitive to the tested oil. The En. faecium strain isolated from ulcers, resistant to 9 out of 14 antibiotics (sensitive to LNZ, SYN, TEC, and VA), was sensitive to thyme essential oil at the lowest concentration of 0.25 μl/ml. All En. faecium clinical strains isolated from urine, resistant to 8 antibiotics, were also sensitive to the oil of thyme; MIC was 0.5 μl/ml. In all, more than 45% of resistant strains were sensitive to thyme oil: MIC=(0.75 μl/ml). Table 3 shows the general characteristics of Enterococcus sp. isolates.
The oil showed bactericidal activity against Es. coli ATCC 25922 standard strain at 0.25 μl/ml (Fig. 1). Figure 2 shows that the same MIC value was determined for 13 strains from the clinical material. Thyme oil of this concentration was effective against clinical strains isolated from the throat and the majority of strains from the wound swabs. An MIC of−0.5 μl/ml was obtained for 17 tested clinical strains of colon bacilli, isolated from the anus, bedsore swabs, and urine. The clinical strains of Es. coli tested that were highly resistant to commonly used antibiotics showed sensitivity to thyme oil.
The multidrug resistant strain isolated from ulcers, resistant to 14 out of 16 antibiotics (sensitive to the ATM, IPM), was sensitive to thyme oil (MIC=(0.25 μl/ml)). The same MIC was obtained for two strains from wound and bedsore swabs, which were sensitive to only 5 out of the 16 tested antibiotics. The growth of nearly 60% of the resistant strains was inhibited by thyme oil at a concentration of 0.5 μl/ml. Table 4 shows the general features of Es. coli isolates.
Strains of P. aeruginosa were the most resistant to the thyme oil. The standard strain—P. aeruginosa ATCC 27853—was inhibited with 0.5 μl/ml. The results are shown in Figure 1. The number of the clinical strains that were sensitive to the thyme oil at 1.5, 2.0, and 2.5 μl/ml was similar, and it is presented in Figure 2. Concentrations of 1.5 and 2.0 μl/ml inhibited the growth of strains mainly isolated from wounds and bedsores. MIC values of−2.0 and 2.5 μl/ml were obtained for blue pus bacilli isolated from ulcers. The highest concentration of thyme oil, 2.5 μl/ml, was effective against the bacteria from bronchial secretions and from the anus swabs. It was found that the most resistant micro-organisms were isolated from bronchial secretions. Two of them were found to be resistant to all 16 antibiotics, and the third was sensitive to only 6 of them. The MIC obtained for thyme oil against these strains ranged from 2.0 to 2.5 μl/ml.
Higher oil activity (MIC-1.5 μl/ml) was obtained against the P. aeruginosa strain isolated from the flank, which showed resistance to 12 antibiotics (sensitive to AMC, TZP, IPM, and NET). At the same time, these strains were sensitive in 40% of thyme oil used at a concentration of 1.5 μl/ml.
Table 5 shows the general characteristics of P. aeruginosa isolates.
Control media containing alcohol (at concentrations used in the dilutions) did not inhibit the growth of bacterial strains.
Discussion
A number of chemotypes were identified in red thyme, T. vulgaris; the most important are the thymol (65% thymol, 5%–10% carvacrol) and carvacrol chemotypes (85% carvacrol, 1%–5% thymol). 42 According to the requirements of the Polish Pharmacopeia VIII and European Pharmacopeia, the oil should contain thymol (36%–55%) and carvacrol (1%–4%).18,40
In our study, the oil showed antimicrobial activity against standard and clinical strains of S. aureus, En. faecalis, En. faecium, En. durans, Es. coli, and P. aeruginosa. The obtained results are in accordance with the literature, and show that thyme oil has strong antimicrobial properties against all tested strains. The activity is due to the high content of phenolic compounds with antibacterial properties, such as thymol and carvacrol, which constitute more than 40% of the ingredients of the oil. 33
In our tests, most of the clinical strains of S. aureus were sensitive to thyme oil at a concentration of 0.5 μl/ml (17 strains), therefore relatively low compared with the high concentrations of antibiotics usually required. These strains came from diverse materials and hospital wards (e.g., swabs from wounds, swabs from nose, and urine). As far as susceptibility to antibiotics was concerned, many isolates were resistant to TE (n=25, 83.3%), CC (n=20, 66.6%), FOX (n=14, 46.6%), E (n=13, 43.3%), and CIP (n=12, 40%). However, all the strains were susceptible to VA, and TEC and only two (from wound and urine) were resistant to LZD. Strains with MIC at 1 μl/ml were isolated from swabs (groin and wound), wards (nephrology and ICU), and remained sensitive to several antibiotics (VA, TEC, C, SXT, and LNZ). There were five isolates for which the MIC was 0.75 μl/ml, isolated from diverse materials, and with different susceptibility to tested drugs.
The increasing prevalence of methicillin resistance among S. aureus strains is an increasing problem, one that has renewed interest in treating S. aureus infections with CC. However, widespread use of MLSB antibiotics has led to an increase of resistance to them. 15 Although Prabhu et al. reports that 28.42% of S. aureus strains are resistant to TE, our results showed much greater resistance to TE as well as CC. 41 Resistant strains were a significant problem in our study−66.6% of the strains were resistant at the same time to at least three antibiotics. However, they were sensitive to glycopeptides and generally to LZD and chloramfenicol. Only 10% of the strains that were susceptible/had intermediate susceptibility to all drugs.
Most of the resistant isolates occurred in the ICU, and the major sites of isolation were swabs (wounds, nose, or ulceration), which is in accord with the literature.41,57 Fortunately, despite the fact that there were many multidrug resistant strains, all of them showed susceptibility to “last line” antibiotics.
In accordance with the literature, T. vulgaris L. oil was shown to inhibit the growth of S. aureus strains isolated from respiratory infections. The tested strains of S. aureus, sensitive to 0.0125 μl/ml of oil, were resistant to oxacylin, GM, and NN, and many of them, to NOR. 19 Oil obtained from Thymus fontanesii Boiss. Et Reut. containing carvacrol at a concentration of 0.3 μl/ml inhibited the growth of the standard and clinical strains of S. aureus isolated from clinical materials. 4 The oil was derived from the carvacrol chemotype of Thymus ciliatus (Desf.) Benth. ssp. eu-ciliatus Maire. Thyme oil was also found to inhibit the growth of pristinamicin-sensitive S. aureus strains isolated from respiratory diseases with MIC 0.8 μl/ml; our results were similar. 7 Research on the antimicrobial properties of thyme oils obtained from different chemotypes of Thymus spinulosus Ten. confirms the relationship between inhibitory activity and the thymol and carvacrol content. These oils contained myrecene, limonene, and γ-terpinene as the dominant components and low concentration of phenolic compounds. Their antimicrobial activity was less effective, with MIC values ranging from 2.25 to 9.0 μl/ml against the standard strain of S. aureus ATCC 25923 and also against En. faecalis ATCC 29212. 14
Many clinical strains of Enterococcus spp. were sensitive to thyme oil at concentrations of 0.5 (n=11) and 0.75 μl/ml (n=16), but En. faecalis isolate was inhibited at 1.25 μl/ml. These strains came from diverse materials and hospital wards. The En. faecium strains were, in general, more resistant to antibiotics than En. faecalis strains. Fortunately, no isolates were resistant to last-line drugs: glycopeptides, SYN, and LZD. However, resistance to TE (n=25, 83.3%), E (n=19, 63.3%), CIP (n=20, 66.6%), GM, and S (n=17, 56.6%) was common. Strains inhibited by 1.25 or 0.75 μl/ml of the essential oil were isolated from different hospital wards and presented diverse susceptibility to antibiotics.
In the last two decades, the importance of En. faecium as a nosocomial pathogen has increased throughout the world due to the greater ability of this species to acquire resistance to drugs than En. faecalis. Very often, resistance among enterococci results from the presence of a putative pathogenicity island. What is interesting is that an increase in AM-resistant En. faecium usually precedes increasing rates of VA-resistant strains.10,54 In our study, there were no isolates showing resistance to VA, but 10 of 11 En. faecium strains were resistant to AM. Regarding TE, although the enterococci resistance rate decreased over time, it remains high in some centers (57%). 10 In our study, the resistance to TE was even higher (83.3%), especially among En. faecalis strains. In addition, erythromycin may be ineffective in therapy. Resistance worldwide is very high, which is in accord with our results.6,46 Overall, rates of high-level resistance to aminoglycosides were higher than those observed recently in Brazil and in the United States.23,45
Due to the high content of active phenols and p-cymene, the oil of T. vulgaris L. showed a very strong activity against standard strains of Enterococcus genus, with MIC values ranging from 0.0625 to 0.85 μl/ml in our studies. MIC values obtained for the clinical strains cultured in the presence of the oil were also significantly lower (0.25–1.25 μl/ml). Mention is made within the literature of the inhibiting properties of thymol from Thymus sp. species on the adhesion of S. aureus and Es. coli clinical strains to epithelial cells of genitourinary system, which may be an alternative to synthetic drugs in the prevention of urinary tract infections. 12
We have shown that clinical strains of Es. coli were sensitive to thyme oil at concentrations of 0.25 μl/ml (13 strains) and 0.5 μl/ml (17 strains). They were more sensitive to oils than P. aeruginosa, S. aureus, and Enterococcus spp. strains. As far as susceptibility to antibiotics was concerned, many isolates were resistant to AMP and TE (n=21, 70%), CF (n=19, 63.3%), SXT (n=15, 50%), and CZ (n=12, 40%). However, all the isolates were sensitive to IPM, and most of them were susceptible to ATM, CAZ, and NET. Strains inhibited by 0.5 μl/ml of essential oil were isolated from diverse materials, in different hospital wards, and, generally, were more resistant to antibiotics than strains inhibited by 0.25 μl/ml.
There was an increase observed in antimicrobial resistance in Es. coli between 2002 and 2009. It was suggested that the observed trends regarding resistance to third-generation cephalosporins, a more than fivefold overall growth in resistance (from 0.6% to 3.4%), may be the result of the addition of resistance traits to strains that were already resistant. 22 It may be explained by the spread of multidrug-resistant plasmids that also contain genes for the production of extended-spectrum beta-lactamase (ESBL).2,35 Resistant strains were a significant problem in our study. The most resistant strains came from wounds (n=13) and were resistant at the same time to even 11 or 14 of the tested drugs. Contrary, there were two isolates (n=6.6%) entirely susceptible to antibiotics and seven that were resistant to one or two of them (n=23.3%).
Studies on the antimicrobial properties of the essential oil obtained from T. fontanesii Boiss. Et Reut. containing carvacrol explain its very strong activity against clinical strains of Es. coli, with an MIC value of−0.35 μl/ml. 4 Similar MIC values were obtained for the carvacrol chemotype of T. ciliatus (Desf.) Benth. ssp. eu-ciliatus Maire eu. against clinical strains of colon bacilli isolated from the respiratory system. 7 In our tests, clinical strains of Es. coli were sensitive to thyme oil at concentrations of 0.25 and 0.5 μl/ml.
P. aeruginosa strains were sensitive to thyme oil at concentrations of 1.0–2.5 μl/ml. Many strains required 2.0–2.5 μl/ml of the essential oil to be inhibited; therefore, they were the most resistant when compared with other tested bacterial species. At the same time, some isolates obtained from bronchial secretions were resistant to all tested antibiotics (n=2). Besides, the great majority of strains were resistant to C (n=28, 93.3%), STX (n=27, 90%), AMC (n=25, 83.3%), PIP and MZ (n=21, 70%), and CTX (n=20, 66.6%). Fortunately, most isolates were susceptible to CAZ (n=4), GM (n=5), IPM, and NET (n=5). Eight strains with an MIC of 2.5 μl/ml were isolated from diverse materials, and their resistance to antibiotics was similar to isolates more susceptible to the essential oil.
A lot of published studies on antibiotic use and resistance have reported increasing resistance among P. aeruginosa strains, 21 some show a decrease in CIP and CAZ resistance among P. aeruginosa isolates as a result of decreased use of those antibiotics. 37 There is also a global problem with MBLs P. aeruginosa strains, which are very often resistant to other important groups of antibiotics tested, including third-generation cephalosporins, aminoglycosides, and quinolones.8,13 In our study, there were some isolates resistant not only to IPM but also to all the other antibiotics tested, which could cause problems with therapy. In this situation, the only therapeutic option may be polymyxins, which should not be used as monotherapy. 53
The most resistant to the tested oil were clinical strains of P. aeruginosa, where inhibition of growth fell in the range of 1.5–2.5 μl/ml. Similar MIC values were obtained using the disk-diffusion method for oil obtained from Thymus persicus L. (thymol−10%, carvacrol−25%) and Thymus eriocalyx (Ronniger) Jalas (thymol−66%). 24 The action of T. spinulosus Ten. essential oil, which has a much lower content of active phenolic compounds (thymol) than that of the oil derived from T. vulgaris L., was much weaker against blue pus bacilli. The obtained MIC values were within the limits of 4.5–9.0 μl/ml, which was in accord with the literature. 44 Other species of thyme such as Thymus zygis L., T. serpyllum L., T. kotschyanus Boiss. & HoH., T. persisus L., and T. longicaulis C. Presl also demonstrate antibacterial activity due to the active phenol content.7,14
The literature reports not only the antimicrobial properties of thyme and oregano essential oils, but also their antioxidant properties as demonstrated by chemotypes from Thymus munybyanus De Noe, T. pallescens De Noe, T. numidicus Poiret, T. guyonii De Noe and oregano: Origanum glandulosum Desf., and O. floribundum Munby. 29 Studies on the biological properties of savory oil (Satureja hortensis L.), containing phenols as predominant compounds, showed antioxidant and antimicrobial properties against standard strains of Gram-positive and Gram-negative bacteria. 27
Due to the bactericidal and fungicidal properties of essential oils, their use in pharmaceuticals and food are more and more widespread as alternatives to synthetic chemical products. Essential oils or some of their components are used in perfume products, in sanitary products, in dentistry, in agriculture, as food preservers and additives, and as natural remedies.28,39 Essential oils are effective in anticancer therapy, cardiovascular, and nervous system disorders; they lower cholesterol levels, decrease and regulate glucose level, and have antioxidative properties. 17 Now, investigations on the mechanism of action of essential oils and their components are carried out both in vitro and in vivo on animals.5,38,47,48 Analytical monographs have been published (National Pharmacopeia, European Pharmacopoeia, ISO, WHO, Council of Europe) to ensure the necessary information about essential oils: their source, concentration of active components, and therapeutic doses. The cytotoxic capacity of essential oils based on their pro-oxidant activity can make them excellent antiseptic and antimicrobial agents. A big advantage of essential oils is the fact that they are usually devoid of long-term genotoxic risks. Moreover, some of them show a very clear antimutagenic activity that could well be linked to an anticarcinogenic activity. Recent studies have demonstrated that the pro-oxidant activity of essential oils or some of their constituents, as also that of some polyphenols, is very efficient in reducing local tumor volume or tumor cell proliferation by apoptotic and necrotic effects.32,36,50,51,56
However, essentials oils may be toxic not only against bacteria, fungi, or viruses but also can have an adverse effect on the human body when overdosed. In eukaryotic cells, essential oils can provoke depolarization of the mitochondrial membranes by decreasing the membrane potential, affect ionic Ca2+ cycling and other ionic channels, and reduce the pH gradient. 52 Some essential oils contain photoactive molecules such as furocoumarins. The essential oils possessing phototoxic activity are obtained from some plant families, such as Apiaceae Rutaceae, Polygonaceae, and Hypericaeae. This may cause damage to cellular macromolecules and, in some cases, the formation of covalent adducts to DNA, proteins, and cellular membrane. 16 Some essential oils or rather some of their constituents may be considered secondary carcinogens after metabolic activation. 26 For example, psoralen, a photosensitizing molecule found in some essential oils, for instance from Citrus bergamia, can induce skin cancer after formation of covalent DNA adducts under ultraviolet A or solar light. 3 In addition, pulegone, a component of essential oils from many mint species, can induce carcinogenesis through metabolism generating the glutathione depletory p-cresol. 58
The application of essential oils in the treatment of many human diseases, particularly infectious diseases caused by multidrug resistant bacterial strains, may be an interesting alternative for synthetic drugs that also show side effects. Essential oils used in combination with antibiotics might prevent antibiotic-resistant strain formation. Due to the therapeutic problems associated with particularly resistant strains, essentials oils can be useful in fighting diseases caused by nosocomial pathogens.
Conclusions
Thyme oil obtained from T. vulgaris L.:
1. Shows very strong activity against standard and clinical strains belonging to: Staphylococcus sp., Enterococcus sp., Escherichia sp., and Pseudomonas sp. genus. 2. It shows lower efficacy against clinical strains of P. aeruginosa. 3. It is active against clinical strains resistant to most tested antibiotics.
Footnotes
Acknowledgments
The authors wish to thank Danuta Kalemba for thyme oil analysis. The research reported in this article was supported by grant no 503/5015-02/503-01 and has not been submitted elsewhere.
Disclosure Statement
No competing financial interests exist.