
Abstract
We sought to identify genotypic resistance classes by real-time PCR in 300 Streptococcus pneumoniae isolates from invasive pneumococcal diseases. Primers and molecular beacon probes were designed for the lytA gene, 3 pbp genes, and the mefA/ermB genes. Targeted sequences of pbp1a, pbp2x, and pbp2b genes in susceptible strain R6 corresponded to those of penicillin G-nonsusceptible strains, including sites within or adjacent to conserved amino acid motifs. If amplification did not occur, the corresponding penicillin-binding protein (PBP) was considered to possess amino acid substitution(s) affecting minimal inhibitory concentrations (MICs) of β-lactam antibiotics. Real-time PCR required 90 min or less. Strains were assigned to six genotypic classes: Genotypic penicillin-susceptible S. pneumoniae (gPSSP) with 3 normal genes (22.3%); genotypic penicillin-intermediate S. pneumoniae (gPISP) (pbp2x) with an abnormal pbp2x gene (25.3%); gPISP (pbp2b) with an abnormal pbp2b gene (7.3%); gPISP (pbp1a+2x) with abnormal pbp1a+2x genes (11.3%); gPISP (pbp2x+2b) with abnormal pbp2x+2b genes (4.7%); or genotypic penicillin-resistant S. pneumoniae (gPRSP) with 3 abnormal PBP genes (29.0%). Sensitivity and specificity of real-time PCR compared with those of conventional PCR were high, 73.7–100% and 97.7–100%, respectively. As for relationships between genotype and β-lactam MICs, 90% of MICs for every resistance class were distributed within three serial dilutions for almost all antibiotics. MICs of each β-lactam antibiotic were estimated with high probability from genotypic patterns. In conclusion, determination of genotypic classes of S. pneumoniae using rapid real-time PCR is useful in selecting effective therapeutic agents for patients with pneumococcal infection.
Introduction
In Japan, clinical isolates of PEN-resistant S. pneumoniae (PRSP) and PEN-intermediate S. pneumoniae (PISP) have increased rapidly since the late 1990s among school and preschool children as well as patients aged 65 years or older with either respiratory tract infections (RTI) or invasive pneumococcal diseases (IPD).28,30 The mortality rate reportedly is higher in elderly IPD patients than in pediatric patients. 8
Characteristically, PRSP and PISP strains show simultaneous resistance to cephalosporin antibiotics used in ambulatory practice. 30 The resistance mechanism for β-lactam antibiotics in PRSP and PISP is a decrease in affinities of three PEN-binding proteins (PBP) involved in peptidoglycan synthesis. These three enzymes, PBP1A, PBP2X, and PBP2B, are encoded by the pbp1a, pbp2x, and pbp2b genes, respectively. Among PEN-nonsusceptible strains (PRSP and PISP), abnormal genetic mosaic patterns of pbp1a, pbp2x, and/or pbp2b were found to differ from those of PEN-susceptible S. pneumoniae (PSSP).9,14 Although a variety of mosaic regions have been detected in each gene, the main contributors to β-lactam resistance are amino acid substitutions identified within or adjacent to conserved amino acid motifs such as Ser-Thr-Met-Lys (STMK), Ser-Ser-Asn (SSN), and Lys-Ser-Gly (KSG).2,3,13,23,24
Therefore, we established a conventional PCR method to determine whether or not a pneumococcal isolate is PEN-susceptible according to molecular evidence. 31 This PCR was completed within 2.5 hr from selection of a colony for testing by amplification and gel electrophoresis. The resistance pattern based on the results of conventional PCR was defined as genotypic (g) resistance and represented by designations such as gPRSP (pbp1a+pbp2x+pbp2b), gPISP(pbp1 a+pbp2x), gPISP(pbp2x), and gPSSP. Currently, the prevalence of gPRSP possessing three abnormal pbp genes exceeds 46% among pediatric patients and 17% among adults in Japan. 8
Given this situation, therapeutic choices for Japanese IPD patients have gradually eroded, with empirical first-line therapy shifting from penicillins or third-generation cephalosporins to carbapenem antibiotics. At the same time, numbers of adults and elderly persons with various underlying diseases posing high risk of IPD have increased rapidly.
In the present study, we aimed to construct a novel assay using real-time PCR that eliminates the need for gel electrophoresis, allowing completion of all procedures within 90 min. We describe sensitivity and specificity of our real-time PCR compared with conventional PCR and efforts to estimate MICs of therapeutic agents against various strains belonging to different PBP genotypic classes.
Materials and Methods
Strains and serotyping
Clinical isolates of S. pneumoniae obtained from IPD patients were collected from 186 clinical laboratories at medical institutions participating in our program of active nationwide surveillance for emerging and re-emerging of infectious diseases. We randomly selected 300 strains as follows: Blood (n=218), cerebrospinal fluid (n=56), pleural fluid (n=14), joint fluid (n=6), and others (n=6). These strains were sent to our laboratory from August, 2006, to July, 2007, accompanied by application form with a similar format as the Active Bacterial Core Surveillance (ABCs) case report.
The serotypes of all strains were determined in real time by the Quellung reaction using antiserum purchased from the Statens Serum Institute (Copenhagen, Denmark). The serotypes of these strains were mainly 6B (n=47), 12F (n=28), 14 (n=27), 3 (n=26), 4 (n=22), 9 (n=20), 19F (n=19), 23F (n=18), 6A/6C (n=16), 19A (n=14), 15 (n=12), and others (n=51).
Real-time PCR primers and molecular beacon probes
Sequences of six sets of primers and molecular beacon (MB) probes and amplicon sizes (bp) applied for our real-time PCR are shown in Table 1. Target genes and the DNA amplification positions were the lytA gene encoding the autolysin enzyme specific to S. pneumoniae 12 ; the pbp1a gene detected in susceptible strains, 18 located in the region including a conserved amino acid motif, STMK, corresponding to that of resistant strains; the pbp2x gene detected in susceptible strains, 16 located in the region surrounding the STMK motif corresponding to divergent sequences of resistant strains; the pbp2b gene detected in susceptible strain, 10 located in the region adjacent the SSN motif; the mefA gene encoding the efflux protein for 14-membered macrolide (ML) antibiotics 25 ; and the ermB gene encoding adenine methylase for 14- and 16-membered ML antibiotics. 27
Primers and MB probes corresponding to pbp1a, pbp2x, and pbp2b genes were designed to amplify the DNA only in susceptible strains. All MB probes were labeled with a fluorescent reporter of 6-carboxyfluorescein (FAM) at the 5′ end and also with a black hole quencher 1 (BHQ-1) at the 3′ end. Reporters and quenchers were connected to stem oligonucleotides.
Real-time PCR conditions
The real-time PCR reaction mixture consisted of 15 μl of 2× real-time PCR Master Mix (Toyobo, Tokyo, Japan), each primer at 0.2 μM, and each MB probe at 0.3 μM. The final volume of the mixture was adjusted to 30 μl by addition of DNase- and RNase-free H2O. After each reaction mixture was pipetted into a 96-well plate, plates were stored at −30°C until use.
One colony grown on a sheep blood agar plate was picked up and suspended in 30 μl of lysis solution. 29 The tube then was placed in a thermal cycler (Gene Amp PCR System 9600R; Perkin-Elmer Cetus, Norwalk, CT) and heat-treated for 5 min at 60°C and for 5 min at 94°C to obtain template DNA. Next, after wells of the frozen real-time PCR reagent were thawed on ice, 2 μl of each template DNA was added to each well. Real-time PCR was performed immediately with a Stratagene Mx3000P (Stratagene, La Jolla, CA). The PCR conditions included an initial DNA denaturation step of 95°C for 30 sec, followed by 40 cycles of 95°C for 15 sec, 50°C for 20 sec, and 75°C for 15 sec. The time required from the lyses reaction to completion of real-time PCR was 90 min.
Conventional PCR
Conventional PCR was performed as a control assay for the real-time PCR in the same strains, using a commercially available kit (Wakunaga Pharmaceuticals, Hiroshima, Japan). The right of commercial production for this kit had been transferred to the company from Ubukata et al.19,30
Sequencing of pbp genes with discrepancies between the two PCR methods
Both the pbp1a and pbp2x genes in S. pneumoniae strains for which a discrepancy in the PCR data was recognized between the conventional and real-time methods were sequenced to identify the amino acid substitution. PCR primers used for analysis were a sense primer for pbp1a, 5′-TGGGATGGATGTTTACACAAATG-3′; a reverse primer for pbp1a, 5′-TGTGCTGGTTGAGGATTCTG-3′; a sense primer for pbp2x, 5′-TATGAAAAGGATCGTCTGGG-3′; and a reverse primer for pbp2x, 5′-AGAGAGTCTTTCATAGCTGAAGC-3′, as described previously.2,3
Amplified DNA fragments were purified using a QIAquick PCR purification kit (Qiagen, Tokyo, Japan) and used as templates. Sequencing reactions were carried out using a BigDye® Terminator Cycle Sequencing kit, version 3.1 (Applied Biosystems, Foster City, CA). DNA sequencing was performed with an ABI 3130/3130xl genetic analyzer (Applied Biosystems).
Susceptibility testing
MICs of the five β-lactam antibiotics PEN, ampicillin (AMP), cefotaxime (CTX), meropenem (MEM), and panipenem (PAM) were determined by an agar dilution method using Mueller–Hinton II agar (MH, Becton Dickinson, Franklin Lakes, NJ) supplemented with 5% defibrinized sheep blood. Bacterial inoculum size and culture conditions were in accordance with a previously described method. 28
S. pneumoniae ATCC49619 and R6 reference strains were used as quality controls.
Multilocus sequence typing and eBURST analysis
Multilocus sequence typing (MLST) performed for S. pneumoniae strains recognized discrepancy in the data of the two PCR methods. MLST and eBURST analysis was performed according to the MLST site (http://spneumoniae.mlst.net/).
Results
Resistant genotypes determined by real-time PCR
Figure 1 shows four patterns from a computer display connected to the real-time PCR instrument shown just after the PCR reaction was completed. Each tested strain was identified as follows: A, as gPSSP by DNA amplification corresponding to lytA (a), pbp1a (b), pbp2x (c), and pbp2b (d) genes; B, as gPISP (pbp2x), with only the pbp2x gene not amplified; C, as gPISP (pbp1a+pbp2x), with pbp1a and pbp2x genes not amplified; and D, as gPRSP (pbp1a, pbp2x, and pbp2b), with all 3 pbp genes not amplified. With regard to ML resistance, a strain showing DNA amplification for mefA and/or ermB genes was identified as ML resistant.
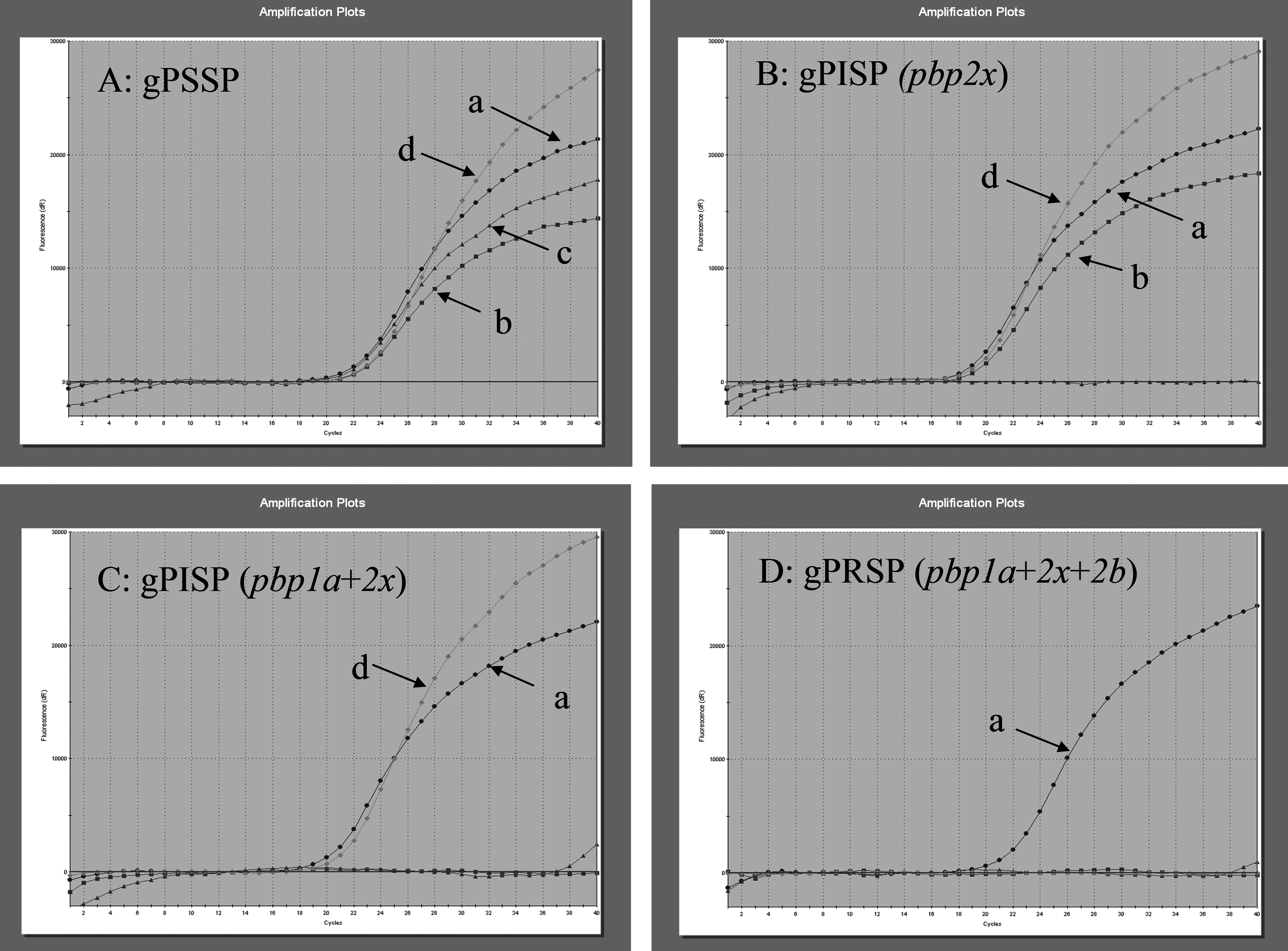
Four genotypic resistance patterns from a computer display connected to the real-time PCR instrument, seen just after the PCR reaction was completed. (
Genotypic classification of β-lactam and macrolide resistance
All strains tested were classified into six genotypic categories by real-time PCR for 3 pbp genes: gPSSP with three normal genes (n=67, 22.3%); gPISP (pbp2x) with an abnormal pbp2x gene (n=76, 25.3%); gPISP (pbp2b) with an abnormal pbp2b gene (n=22, 7.3%); gPISP (pbp1a+2x) with abnormal pbp1a+2x genes (n=34, 11.3%); gPISP (pbp2x+2b) with abnormal pbp2x+2b genes (n=14, 4.7%); and gPRSP with three abnormal PBP genes (n=87, 29.0%). Strains examined included 106 from pediatric patients (35.3%) and 194 from adult patients (64.7%). Percentages of the strains representing gPRSP accounted for 50.5% of isolates from children and 17.5% of those from adults.
Although detailed data are not shown, ML resistance in these strains was classified into four genotypic categories based on presence or absence of resistance genes: ML-susceptible strains (n=58, 19.3%); 14-membered ML-resistant strains possessing an mefA gene (n=79, 26.3%); 14- and 16-membered ML-resistant strains possessing an ermB gene (n=150, 50.0%); or an ML-resistant strain possessing mefA and ermB genes (n=13, 4.3%). Proportions of strains showing ML resistance were 85.9% of isolates from children and 77.9% of the isolates from adults.
Sensitivity and specificity of real-time PCR
As shown in Table 2, sensitivity and specificity for all strains were compared between conventional and real-time PCR. The sensitivity and specificity for the mefA gene and the ermB gene were calculated to be 100%.
Sensitivity.
Specificity.
Table 3 shows detailed information for the nine strains (3.0%) showing a discrepancy between real-time PCR and conventional PCR. In these strains, DNA amplification for the pbp1a or pbp2x gene corresponding to the susceptible strain occurred weakly in conventional PCR but not at all in real-time PCR. According to susceptibility testing for AMP, and CTX, results of real-time PCR proved more accurate than those of conventional PCR. Overall, our new real-time PCR method showed to have excellent sensitivities and specificities compared with those of conventional PCR.
When DNA amplification occurred, the corresponding pbp gene showed the same sequences as the susceptible strain; for example, a strain showing amplification of pbp1a and pbp2b genes was designation gPISP(pbp2x).
ST6939 is not present in any group of clonal complexes.
MIC, minimum inhibitory concentration; PEN, penicillin; AMP, ampicillin; CTX, cefetaxime; MEM, meropenem; PAM, panipenem; ST, sequence type; CC, clonal complex; gPSSP, genotypic penicillin-susceptible Streptococcus pneumoniae; gPISP, genotypic penicillin-intermediate S. pneumoniae; gPRSP, genotypic penicillin-resistant S. pneumoniae.
Relationships between PBP gene alterations and MIC of β-lactam agents
Figure 2 shows relationships between MICs of five β-lactam agents and results of real-time PCR for pbp1a, pbp2x, and pbp2b genes in the tested strains. MICs of PEN, MEM, and PAM were affected by pbp2b alterations rather than those in pbp2x. On the other hand, the MIC of CTX was 4–8 times lower than that of PEN due to pbp2x alterations. Notably, 90% of MICs in each genotype resistance class were distributed essentially within three serial dilution concentrations (for instance, gPRSP in PEN, from 0.5 to 2 mg/L) for almost all antibiotics. However, eight gPSSP strains with a CTX MIC ranging from 0.125 to 0.25 mg/L possessed substitutions of Thr550Ala adjacent to a KSG motif in PBP2X that could not be detect with the real-time PCR constructed in this study.
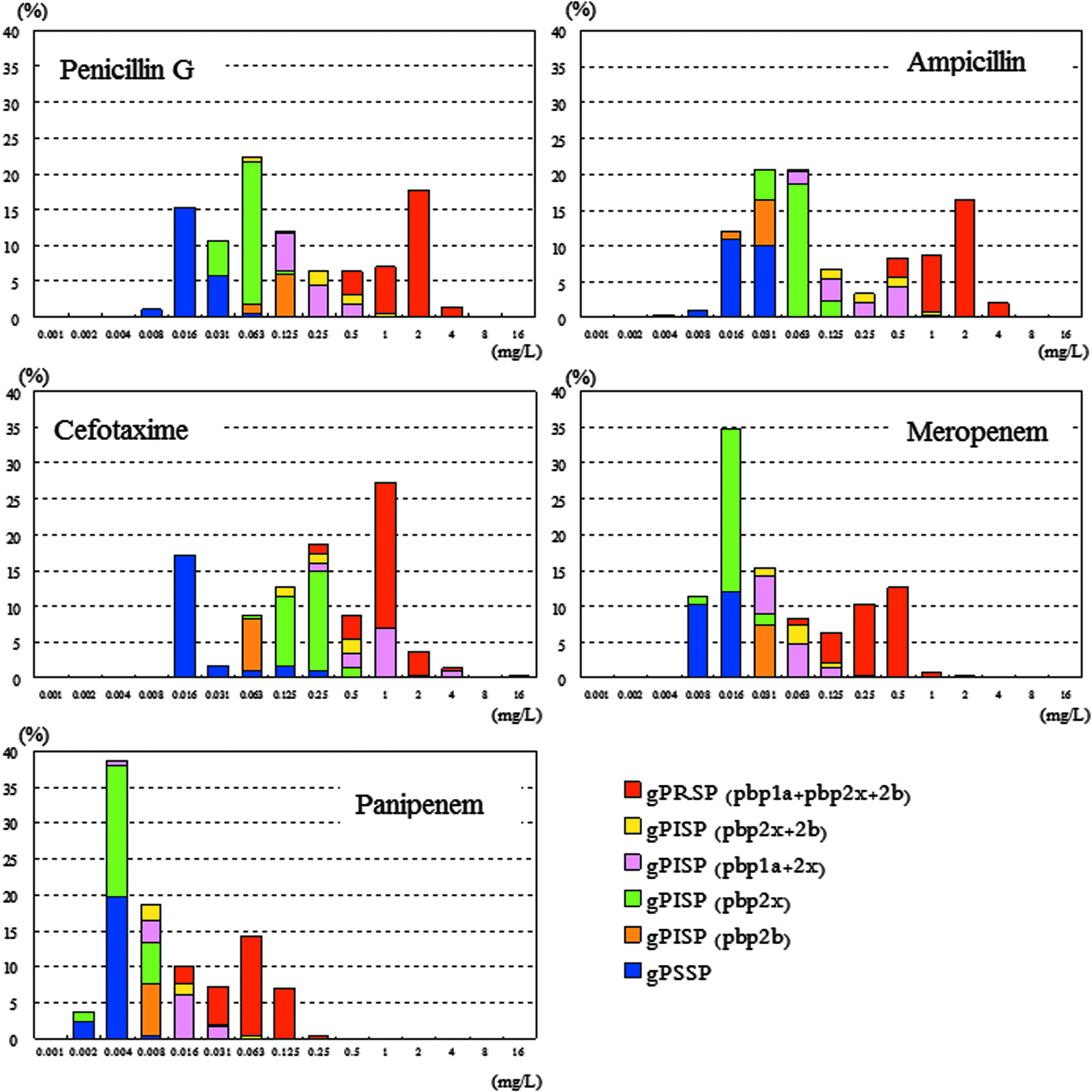
Correlation between minimal inhibitory concentrations (MICs) of five β-lactam antibiotics and penicillin-binding protein (PBP) gene alterations for 300 Streptococcus pneumoniae isolates from invasive infections.
Estimated MIC50 values and corresponding ranges for 90% of β-lactam antibiotics among six PBP genotypic categories are listed in Table 4. On the basis of these data, MIC estimation for parenteral β-lactam antibiotics associated with clinical efficacy could be made with high probability.
MIC, minimum inhibitory concentration; PEN, penicillin; AMP, ampicillin; CTX, cefetaxime; MEM, meropenem; PAM, panipenem; gPSSP, genotypic penicillin-susceptible Streptococcus pneumoniae; gPISP, genotypic penicillin-intermediate S. pneumoniae; gPRSP, genotypic penicillin-resistant S. pneumoniae.
Discussion
The ultimate global public health goal in the 21st century is to develop and disseminate vaccination to prevent infectious diseases caused by various viruses and bacteria more effectively. For immunity against pneumococcal infections, development of 23-valent pneumococcal polysaccharide vaccine (PPV23) 5 began in the early 1980s in the United States, and this vaccine was introduced in Japan in 1988. In Japan, 7-valent pneumococcal conjugate vaccine (PCV7) has just been approved on a voluntary basis to prevent IPD among children with immunologic immaturity.
In countries where PCV7 has been introduced into the vaccine schedule, incidence of pediatric IPD caused by vaccine-type strains has decreased significantly,4,6,22 while a related decrease of IPD among adults also has been reported. 17 However, prevalence of IPD caused by serotypes 19A and 6A (nonvaccine types) has increased, accompanied by a shift from PEN-susceptible to PEN-resistant strains.7,11,21 Some investigators also have reported that overall incidence of IPD is little changed. 26
In Japan, great clinical attention has been paid to the increase of PRSP and PISP among S. pneumoniae isolates from IPD, 8 which strongly reflects the difference in use of oral antibiotics between pediatricians and internists. Specifically, in pediatric practice, oral cephalosporins are favored over penicillins for outpatients, although a recent shift back toward amoxicillin and AMP has been noted. On the other hand, in internal medicine, ML and fluoroquinolone agents rather than β-lactam antibiotics are preferred. This might contribute significantly to rates of gPRSP isolated from pediatric patients and gPISP isolated from adult patients.
These situations concerning antibiotic resistance, in addition to the present state of pneumococcal vaccination, show that a need for rapid and accurate determination of resistance in clinical isolates is necessary for appropriate selection of chemotherapeutic agents in pneumococcal infections.
We initially identified species and antibiotic resistance using colony samples likely to be S. pneumoniae from blood agar plate using a conventional PCR method completed within 2.5 hr using gel electrophoresis. 30 Intrinsically, three primer sets designed on pbp1a, pbp2x, and pbp2b genes detect the most important amino acid substitutions affecting β-lactam susceptibilities, all positioned within or adjacent to conserved amino acid motifs in each PBP—substitutions from STMK to SAMK or SSMK in PBP1A, substitutions from STMK to SAMK or SAFK and from (L)KSG to (V)KSG in PBP2X, and substitution from SSN(T) to SSN(A) or SSN(S) in PBP2B. The genotypic resistance pattern based on the pbp gene analysis was divided into six categories: gPSSP, gPISP(pbp2x), gPISP(pbp2b), gPISP(pbp1a+pbp2x), gPISP(pbp2x+pbp2b), and gPRSP (pbp1a+pbp2x+pbp2b).
This was not shown in the results, but each class of resistance genes was not of a single clone. For example, gPRSP was divided into 11 serotypes with various clonal complexes (CCs). The major serotypes and CCs were serotype 6B with CC156 and CC490, serotype 19F with CC320, serotype 23F with CC156, CC242 and CC1437, serotype 6A with CC3115, CC3787 and CC81, and serotype 14 with CC320 and CC554.
As stated in the Results section, real-time PCR yielded satisfactory sensitivity and specificity compared with conventional PCR. Accurate estimation of MICs of each β-lactam antibiotic on the basis of genotypic patterns is highly important. Our novel real-time PCR assay also can be completed within 90 min after selection of colony samples, with elimination of gel electrophoresis, saving both time and labor.
Another merit of this assay is possible direct testing of usually sterile specimens (such as cerebrospinal fluid, joint fluid, and pleural fluid) from IPD patients, because primers and MB probes for amplification of the lytA gene are included in the real-time PCR. In the future, simultaneous performance of speciation and identification of resistance gene(s) by real-time PCR should optimize cost and benefit in clinical settings.
Footnotes
Acknowledgments
Our study was funded in part by a grant under the category ‘‘Research on Emerging and Re-emerging Infectious Diseases'’ (number H22-013) from the Japanese Ministry of Health, Labour and Welfare (to Dr. K. Ubukata).