
Abstract
Changes in the epidemiology of Streptococcus pneumoniae were reported worldwide after the introduction of the 7-valent pneumococcal vaccine, particularly an increase in multi-drug resistant (MDR) 19A strains. Subsequently, a 13-valent pneumococcal vaccine (PCV-13) has been introduced. This study assessed the incidence of S. pneumoniae serotypes in all age groups prior to the introduction of PCV-13 in Canada (2007–2009). Eight hundred S. pneumoniae isolates from respiratory specimens and blood cultures were collected as part of a Canadian surveillance study (CANWARD) from patients in 15 tertiary-care centers. Serotyping was performed by the Quellung method and antimicrobial susceptibility testing was performed by broth microdilution in accordance with the Clinical and Laboratory Standards Institute guidelines. The most common serotypes were 19A (8.6%), 3 (7.3%), 22F (6.0%), 4 (4.6%), 5 (4.4%), and 11A (4.4%); and the first serotype 6D isolate in Canada was identified. Serotypes 5, 7F, and 19A were significantly (p<0.001) more frequently isolated from bloodstream infections. Considerable serotype variability was noted for different age groups: 15B (p<0.01) and 19A (p<0.001) were more frequently isolated from children ≤2 years old. Overall, 46.4% of currently circulating S. pneumoniae serotypes in Canada are included in PCV-13. Notably, 87.5% of MDR-S. pneumoniae were covered by PCV-13. Accordingly, PCV-13 will provide coverage against a significant proportion of circulating S. pneumoniae strains in Canada, including the critical antimicrobial-resistant strains.
Introduction
The Canadian Immunization Monitoring Program, Active (IMPACT), which monitors the incidence of IPD in Canadian children 0 to 16 years of age, recently reported a significant decrease in the number of cases between 2000 and 2007 (48% overall and 56% in children<5 years of age). 2 Dramatic decreases in the incidence of IPD were also observed in the United States, with reports of a 75% reduction in children<5 years of age. 5 Likewise, the incidence rate of IPD for individuals 5 years of age and older decreased by 62% for vaccine serotypes and 29% overall, demonstrating considerable herd immunity. 5 Despite the success of PCV-7, the incidence of IPD caused by non-PCV-7 serotypes subsequently increased, particularly due to 19A strains.6,14
To enhance the protection provided by the pneumococcal conjugate vaccines, new formulations have been developed including the 10-valent vaccine (PHiD-CV), composed of the PCV-7 serotypes plus 1, 5, and 7F, and the 13-valent vaccine (PCV-13), composed of the PHiD-CV serotypes plus 3, 6A, and notably 19A. Due to the enhanced coverage of the predominant serotypes in North America, current NACI and ACIP guidelines recommend the routine use of PCV-13.6,14
The purpose of this study was to assess the circulating serotypes of S. pneumoniae from all age groups in Canada between 2007 and 2009, prior to the introduction of the PCV-13 vaccine.
Materials and Methods
Bacterial isolates
S. pneumoniae isolates were collected as part of the CANWARD study (an annual national surveillance study) from patients in 15 tertiary-care centers across Canada between 2007 and 2009, inclusive. 15 Eight hundred isolates (400 respiratory isolates and 400 blood culture isolates) were randomly selected for inclusion in this study.
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing was performed as previously described. 15 Briefly, the in vitro activities of penicillin, ceftriaxone, clarithromycin, levofloxacin, trimethoprim-sulfamethoxazole, and doxycycline were determined by the broth microdilution method using custom-designed 96-well microdilution panels, in accordance with the Clinical and Laboratory Standards Institute (CLSI) guidelines. 7 The minimum inhibitory concentrations (MICs) were interpreted based on CLSI breakpoints. 8
Serotype determination
The serotype of each isolate was determined by the Quellung reaction following standard methodology 1 using type specific antisera obtained from the Statens Seruminstitut (Copenhagen, Denmark). Infrequently observed serotypes were confirmed by the Centre for Disease Control and Prevention's polymerase chain reaction methodology (www.cdc.gov/ncidod/biotech/strep/pcr.htm) at the National Microbiology Laboratory–Public Health Agency of Canada.
Statistical analysis
Differences in serotype coverage by PCV-7 and PCV-13, serotype distribution in blood culture and respiratory isolates, and serotype distribution among children ≤2 years of age and individuals in all other age groups were evaluated for statistical significance by two-tailed Chi-squared analysis or Fisher's exact test, as appropriate. The diversity of the serotypes within each age group was evaluated by the Simpson's Index of Diversity (SID).
Results
Among the 800 S. pneumoniae isolates evaluated in this study, 48 serotypes were observed (Fig. 1). Figure 1 portrays the serotype distribution for blood culture (a) and respiratory isolates (b) of S. pneumoniae. Overall, the most common serotypes circulating in Canada between 2007 and 2009 were 19A (8.6%), 3 (7.3%), 22F (6.0%), 4 (4.6%), 5 (4.4%), and 11A (4.4%). Notably, an isolate of the newly described serotype 6D 3 was identified in this study. The organism was isolated from a respiratory sample from a 65 year-old-female. This is the first report of the 6D serotype in Canada.
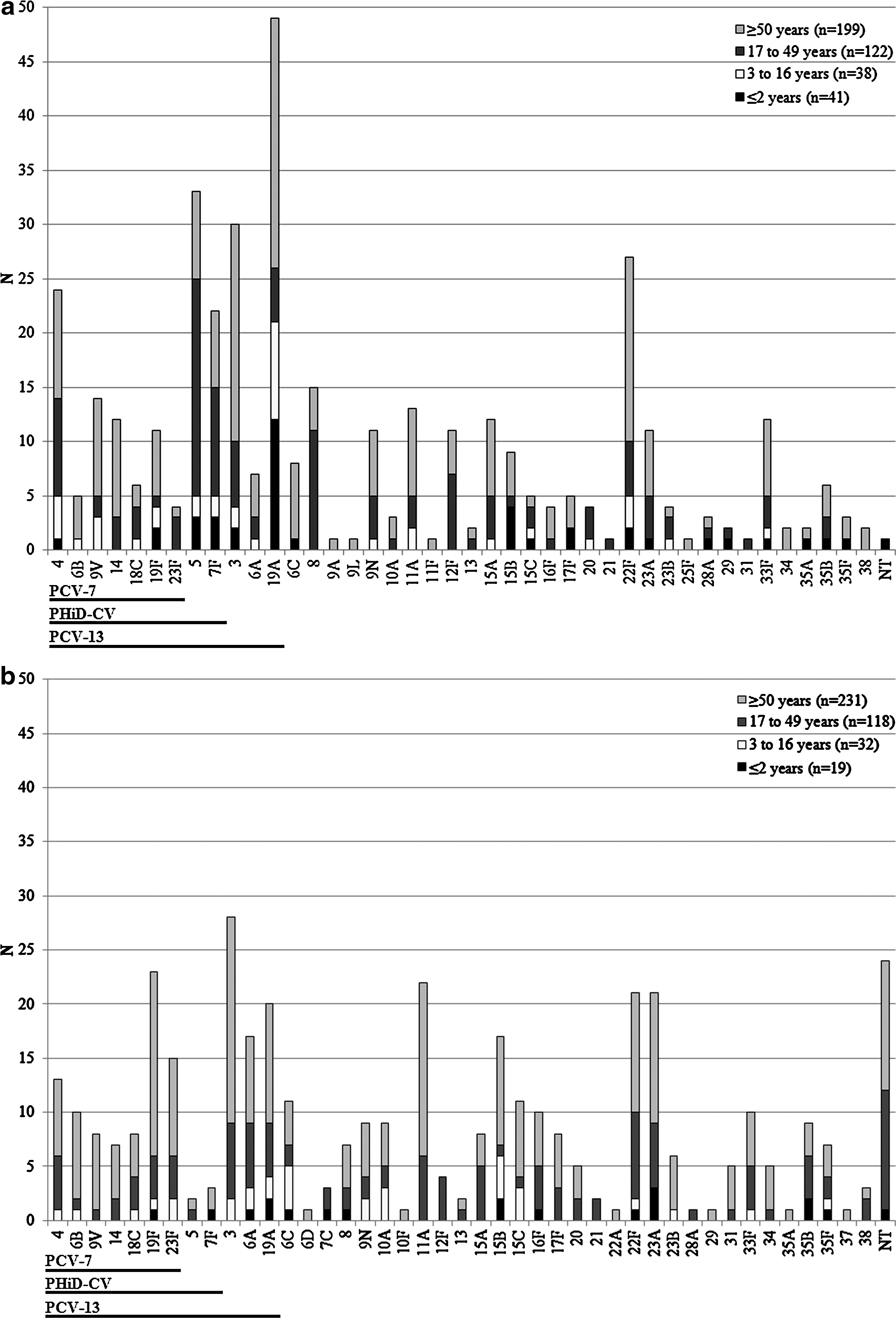
Serotype distribution of Streptococcus pneumoniae isolated from blood cultures
The S. pneumoniae serotype distribution was evaluated by specimen source and by age group (Fig. 1). Serotypes 5, 7F, and 19A were significantly more frequently isolated from bloodstream infections than respiratory specimens (8.3% versus 0.5%, 5.5% versus 0.8%, and 12.3% versus 5%, respectively, p<0.001). Conversely, serotypes 6A (4.3% versus 1.8%, p=0.04), 19F (5.8% versus 2.8%, p=0.04), 23F (3.8% versus 1%, p=0.02), and nontypeable isolates (6% versus 0.3%, p<0.001) were more commonly observed from respiratory specimens than from bloodstream infections. Among children 2 years of age and less (n=60), 23 serotypes were observed with serotype 19A accounting for 23.3% of the isolates. Other common serotypes in this age group included 15B (10.0%), 7F (6.7%), 23A (6.7%), 5 (5.0%), 19F (5.0%), 22F (5.0%), and 35B (5.0%). Serotypes 15B (p<0.01) and 19A (p<0.001) were significantly more frequently isolated from children 2 years of age and less than from individuals of all other age groups. Among children 3 to 16 years (n=70), adults 17 to 49 years (n=240), and individuals 50 years of age and older (n=430), the number of serotypes observed was 23, 39, and 46, respectively. The most common serotypes among children 3 to 16 years of age were 19A (15.7%), 4 (7.1%), 3 (5.7%), 6C (5.7%), 15B (5.7%), 15C (5.7%), and 22F (5.7%). Among adults aged 17 to 49 years, the predominant serotypes were 5 (8.8%), 4 (5.8%), 3 (5.4%), 8 (5.4%), and 22F (5.4%). The most commonly observed serotypes among individuals aged 50 years and older were 3 (9.1%), 19A (7.9%), 22F (6.5%), 11A (5.6%), and19F (5.3%). Although the number of serotypes varied between the age groups, all of the groups demonstrated high levels of serotype diversity (SIDs>0.9).
The coverage provided by PCV-7, PHiD-CV, and PCV-13 against the currently circulating S. pneumoniae serotypes is displayed in Fig.1 and detailed by specimen source and age group in Table 1. Serotypes were defined as vaccine serotypes when the serotype was included in the vaccine formulation, as vaccine-related serotypes when the serotype belonged to a serogroup with at least one other serotype included in the vaccine, and as nonvaccine serotypes when the serogroup was not represented in the vaccine. Overall, 46.4%, 27.5%, and 20% of the circulating S. pneumoniae serotypes in Canada were included in PCV-13, PHiD-CV, and PCV-7, respectively. The enhanced coverage provided by PCV-13 was most notable for blood culture isolates (PCV-13: 54.3% versus PCV-7: 19%, p<0.001), especially among children ≤2 years of age (PCV-13: 56.1% versus PCV-7: 7.3%, p<0.001).
A large number of isolates were included in the vaccine-related serotypes category for PHiD-CV (22.5%) and PCV-7 (22.1%), primarily due to the predominance of 19A. For PCV-13, 10.9% of isolates had vaccine-related serotypes of which 23A/B, 6C, and 9N were the most common.
The most common serotypes that were not covered by PCV-13 or related to serotypes covered by PCV-13 were 22F, 11A, 15B, nontypeable isolates, 8, 33F, and 15A. Among children 2 years of age or less, the most common serotypes that were not directly or possibly indirectly covered by PCV-13 were 15B, 22F, and 35B.
Table 2 displays the antimicrobial susceptibility of S. pneumoniae isolated in Canada between 2007 and 2009. The antimicrobial susceptibility patterns are presented by specimen source (respiratory or blood) and based on the coverage provided by PCV-13. The differences in susceptibility rates between blood culture and respiratory isolates ranged from 1% for ceftriaxone (nonmeningitis CLSI interpretative breakpoints) to 13.4% for clarithromycin. The differences in susceptibility rates between PCV-13 serotypes and non-PCV-13 serotypes were <5% (range 0%–2.5%) for penicillin (non-meningitis CLSI interpretative breakpoints), ceftriaxone, clarithromycin, levofloxacin, and doxycycline. Conversely, differences in susceptibility rates between PCV-13 serotypes and non-PCV-13 serotypes were greater than 5% (range 11.7%–12.1%) for penicillin (meningitis CLSI interpretative breakpoints) and trimethoprim-sulfamethoxazole.
Doxycycline interpreted with tetracycline breakpoints [10]
CLSI, Clinical and Laboratory Standards Institute.
Of the 800 S. pneumoniae, 24 (3%) isolates were considered multi-drug resistant, which was defined as organisms with a penicillin MIC ≥2 μg/ml and resistance to at least one more of the tested antimicrobials from a different antimicrobial class. In addition to having a penicillin MIC ≥2 μg/ml, 2 isolates were resistant to clarithromycin, 8 were resistant to trimethoprim-sulfamethoxazole, 1 was resistant to doxycycline, 11 were resistant to clarithromycin and trimethoprim-sulfamethoxazole, and 2 were resistant to clarithromycin and doxycycline. The majority of the multi-drug resistant S. pneumoniae (16/24, 66.7%) were isolated from respiratory specimens. By serotype, the multi-drug resistant isolates observed were as follows: 8 of serotype 9V, 2 of serotype 14, 1 of serotype 15A, 6 of serotype 19A, 3 of serotype 19F, 1 of serotype 22F, 2 of serotype 23F, and 1 non-typeable strain.
Discussion
Prior to the introduction of PCV-13 in Canada in 2010, a broad range of serotypes were identified among S. pneumoniae causing respiratory and bloodstream infections. The most commonly circulating serotypes in Canada included 19A, 3, 22F, 4, 5, and 11A. As part of this study, we report the first isolation of serotype 6D in Canada. Variability in serotype distribution was observed among the different specimen sources and age groups. Serotypes 5, 7F, and 19A were significantly more frequently isolated from bloodstream infections than respiratory specimens. A recent study conducted in France reported similar differences in serotype distribution by specimen source, with serotypes 1, 19A, and 7F being most common in IPD specimens. 10 The invasiveness of specific serotypes may be dependent on a variety of factors, including the ability to resist phagocytosis and the persistence of colonization.10,11
Similarly, the observation of significant differences in the serotype distribution by age group is consistent with the current literature.10,11 Non-PCV-7 serotypes, such as 19A and 15B, were predominant among children<2 years of age in this study. Recently reported data from the IMPACT study also demonstrated that non-PCV-7 serotypes, 19A, 3, 22F, 7F, 5, and 15C, were the most commonly observed serotypes. 2 In the IMPACT study, only serotype 19A was found to have significantly increased subsequent to the introduction of the PCV-7 immunization program. 2 The current predominance of 19A in young children is well described in various regions of the world.2,9,10 Among children 3 to 16 years in this study, serotypes 19A, 15B/C, and 4 were the most common. A similar serotype distribution was observed among children 0 to 14 years in the United States in 2003/2004 with serotypes 19A, 6A, 3, 15, and 35B predominating. 9 Interestingly, serotype 19A was the most common serotype in children<16 years and in individuals aged 50 years and older but it was not identified as one of the top 5 serotypes causing infections in adults between the ages of 17 and 49 years. The high proportion of 19A strains among young children and older adults was also recently observed in France. 10
Based on the current serotype distribution, PCV-13 provided significantly greater coverage than PCV-7 overall. The enhanced coverage provided by PCV-13 was most notable for children ≤2 years of age with invasive S. pneumoniae infections. This observation is similar to the serotype distribution at the time PCV-7 was introduced in the United States; there was a greater proportion of PCV-7 serotypes in blood cultures compared with respiratory specimens and in children 2 years of age and less compared with children between the ages of 3 and 14 years. 9 Good coverage of invasive strains in young children is key for new vaccine formulations as this is the critical patient age group with the highest incidence of invasive disease and for which routine immunization is recommended. The reduced level of coverage provided by PCV-7 concurs with recent reports, which demonstrate that only 27% of serotypes in the United States in 2003/2004 and 20.7% of serotypes in France in 2009 were covered by PCV-7.9,10 Due to the inclusion of key serotypes like 19A in PCV-13, the coverage provided by PCV-13 is significantly greater than PCV-7.
With the increased prevalence of serotype 19A, which is frequently antimicrobial-resistant, an assessment of the antimicrobial susceptibility pattern of S. pneumoniae is important. The antimicrobial susceptibility of 800 S. pneumoniae isolated from blood cultures and respiratory specimens in Canada were evaluated as part of this study. S. pneumoniae isolated from blood cultures demonstrated greater susceptibility than strains from respiratory specimens. Other studies have also noted higher resistance rates for S. pneumoniae isolated from the respiratory tract, including acute otitis media specimens.9,10,11 Overall, greater susceptibility to penicillin (meningitis CLSI interpretative breakpoints) and trimethoprim-sulfamethoxazole was noted among the non-PCV-13 serotypes; susceptibility to ceftriaxone, clarithromycin, levofloxacin, and doxycycline was similar for PCV-13 and non-PCV-13 serotypes. Eighty-eight percent of the multi-drug resistant S. pneumoniae were serotypes covered by PCV-13. The coverage of multi-drug resistant strains by PCV-13 was considerably greater than the coverage provided by PCV-7 (87.5% versus 62.5%). The increased coverage of antimicrobial-resistant strains by PCV-13 is critical as the overall rate of penicillin resistance in S. pneumoniae remained stable after the introduction of PCV-7 despite the fact that almost 90% of penicillin non-susceptible isolates were PCV-7 serotypes prior to the introduction of the vaccine. 2 Although a decrease in penicillin resistance among PCV-7 serotypes was observed subsequent to the introduction of PCV-7, a concomitant increase in penicillin resistance occurred in non-PCV-7 serotypes. 2 The emergence of antimicrobial-resistant 19A strains largely accounts for the consistent overall rate of penicillin resistance following the introduction of PCV-7. 2
In conclusion, PCV-13 provides coverage of a large percentage of circulating S. pneumoniae strains in Canada and importantly, it provides protection against the critical antimicrobial-resistant strains. Ongoing surveillance of the epidemiology of S. pneumoniae in Canada is essential to assess the impact of the introduction of PCV-13 and guide the development of future vaccines.
Footnotes
Acknowledgments
The authors acknowledge the technical expertise of Nancy Laing at the University of Manitoba and Irene Martin, Walter Demczuk, and Averil Griffith at the National Microbiology Laboratory–Public Health Agency of Canada in Winnipeg, Manitoba, Canada.
Funding for this study was provided in part by the University of Manitoba Health Sciences Centre in Winnipeg, Manitoba, Canada and Pfizer Canada.
Disclosure Statement
GGZ received a study grant for this study from Pfizer Canada.
All other authors have no conflicts of interest to declare.