
Abstract
Antimicrobial-resistant bacteria represent a major threat to human and animal health. We compared equine fecal samples (n=264) from 138 horses from hospital and nonhospital (livery stable and riding school) premises in North West England to determine the prevalence of Escherichia coli, Salmonella, and Campylobacter and rates of antimicrobial-resistant E. coli strains. Campylobacter jejuni was detected only in hospitalized horses (1.1%), and no Salmonella was identified. Data analysis of the horses' management and veterinary treatments (Tx) identified risk factors associated with shedding of antimicrobial-resistant E. coli. The hospital was the major source of resistant and multi-drug-resistant (MDR) E. coli. Moreover, shedding of antimicrobial-resistant E. coli was associated significantly with hospitalization for a gastrointestinal problem (odds ratio [OR]:±95% confidence intervals=8.50:1.79–40.32), receipt of oral antimicrobial Tx (OR=3.52:1.11–11.10), multiple antimicrobial Tx in hospital (OR/Tx=1.05:1.01–1.09), or geldings (OR=4.62:1.23–17.46). Interestingly, intravenous antimicrobial Tx was negatively associated with shedding of antimicrobial-resistant E. coli (OR=0.18:0.04–0.76). MDR E. coli was associated with hospitalization, antimicrobial Tx in hospital (OR/Tx=3.65:1.54–8.68), and increased age (OR/year=1.11:1.03–1.19). Thus, equine hospitals in this geographic location appear to be an important source of antimicrobial-resistant and MDR E. coli strains, but unlikely reservoirs of Salmonella or Campylobacter. Thus, it is important to moderate antimicrobial Tx given to hospitalized horses to lessen exposure and fecal shedding of resistant pathogens.
Introduction
The widespread use of antibiotics in agriculture and veterinary medicine has been implicated in the emergence of antibiotic-resistant Escherichia coli strains that potentially can be transmitted to humans through indirect or direct contact.11,38 Typically, E. coli are commensal inhabitants of the gastrointestinal tract, but some strains express genes associated with pathogenicity for certain diseases such as urinary tract infections and inflammatory bowel diseases. 19
Horses are recognized reservoirs of zoonotic bacteria (E. coli, Salmonella, and Campylobacter), although these pathogens comprise a small proportion of the horses' microbiome. 13 Most surveys of antibiotic-resistant bacteria in the nonhuman populations have focused on food-producing animals of industrialized nations (cattle, swine, and poultry). Relatively little information is available about companion animals, such as horses, as a potential source of zoonotic enteric bacteria or antibiotic-resistant bacteria. Interestingly, the genetic diversity of equine E. coli has been reported to be higher than in humans or cattle. 7 Thus, monitoring of antimicrobial-resistant bacteria, including pathogenic, zoonotic, and commensal, has been advised. 32
In addition to E. coli, Salmonella is another major contributor to acute and chronic enteric disease in horses53,55 and a major cause of nosocomial infections in hospitalized horses.50,18 Horses can harbor latent gastrointestinal infections of Salmonella without clinical symptoms. Another common gram-negative enteric pathogen, Campylobacter associated with zoonosis,36,59 has been implicated in equine enteritis (Campylobacter jejuni) and gastrointestinal lesions (Campylobacter coli).6,21
The emergence of bacteria possessing multiple antibiotic resistance genes has become a major concern in recent years, and multi-resistant E. coli has been reported as a serious health threat. 37 Multi-drug-resistant (MDR) bacteria spread via the acquisition of resistance genes through plasmids and transposons5,24 or through clonal selection of strains with mobile genetic elements (integrons), such as Salmonella typhimurium DT104 48 and E. coli. Mobile genetic elements and chromosomal systems, such as the mar locus, both contribute to the MDR phenomenon. 4
Currently, there is a paucity of information concerning antimicrobial-resistant bacteria in horses.20,25,44 Dunowska et al. 20 suggested that both hospitalization and antimicrobial administration contribute to the development of resistance among equine E. coli fecal. Similar human medicine studies have shown that hospitalization is associated significantly with an increase in antibiotic resistance pathogenic bacteria, although the correlation did not extend to the prevalence of antibiotic resistance in E. coli. 14
In humans, overuse of antibiotics, particularly fluoroquinolones, has been shown to be a risk factor for shedding bacteria that are resistant to the administered antimicrobial compound. 39 Induced resistance, such as from quinolone therapy, and prior therapy with other antimicrobial agents have both been identified as risk factors for emergence of the antimicrobial-resistant phenotypes among E. coli isolates of human origin; importantly, the demographic variables of age, sex, and occurrence or duration of long-term care were not identified as risk factors. 28 Furthermore, resistance to fluoroquinolones has often coincided with the MDR phenotype and has yet to be reported as arising independently of resistance to at least one other agent. 49 Other studies have identified similar risk factors associated with antimicrobial and MDR E. coli and other classes of antibiotic drugs, such as penicillins (including ampicillin).23,33
Previously, we had collected equine fecal samples from an equine hospital and livery premises to investigate the distribution of enteric pathogens and anti-microbial-resistant strains. We published evidence of antimicrobial-resistant genes and events of horizontal gene transfer in E. coli indicating that these organisms shedding out in horse manure represent a potential zoonotic threat to public health. 3 Here, we extended our analysis of the original dataset to determine the prevalence and resistance phenotypes of E. coli, Salmonella, and Campylobacter in these samples. By performing comparative analysis of hospital-based samples with nonhospital samples, we identified the risk factors associated with equine gastrointestinal carriage and shedding of antimicrobial-resistant E. coli.
Materials and Methods
Study design
Equine fecal samples were collected for 6 months from hospitalized and nonhospitalized populations of horses residing in the North West region of England, as described. 3 In total, the sample pool consisted of 264 fecal samples collected from 138 horses. Specifically, 66 hospitalized horses that were in-patients at the Philip Leverhulme Equine Hospital (PLEH, University of Liverpool, a referral hospital specializing in gastrointestinal referred conditions) provided 109 samples. The nonhospitalized samples were sampled randomly from two different premises: 37 horses maintained at a riding school (Premises A) accounting for 112 samples; 35 horses maintained at a livery yard (Premises B) accounting for 43 samples.
Culture, isolation, and identification methods
Five grams of each fresh fecal sample was mixed with 5 ml of brain-heart infusion broth containing 5% glycerol; 1 ml aliquots were used to isolate bacteria, and remaining fecal suspensions were stored at −80°C. E. coli, Salmonella, and Campylobacter bacteria were isolated and identified as detailed below. All media used were purchased from Oxoid Ltd. (Hampshire, United Kingdom).
E. coli
One milliliter of the fecal suspension was added to 3 ml of brilliant green broth (BGB) and incubated aerobically for 24 hours at 37°C. The BGB volume was then streaked onto eosin methylene blue agar and incubated for an additional 24 hours at 37°C. Three metallic colonies typical of E. coli morphology were selected randomly and transferred onto nutrient agar plates. These plates were incubated for 24 hours under the same conditions for further confirmation using the Gram-negative enteric bacteria Api20E test strip (bioMerieux, Hazelwood, MT) as described. 3
Salmonella
One milliliter of the fecal suspension was added to 10 ml of buffered peptone water and incubated aerobically at 37°C for 24 hours. After incubation, 1 ml was transferred to Rappaport-Vassiliadis broth (10 ml) and incubated under aerobic conditions at 42°C for 24 hours. This culture was then used to inoculate xylose lysine decarboxylase agar and incubated for an additional 24 hours. Suspected typical colonies (i.e., red colonies with black centres) were transferred onto nutrient agar and further confirmed using agglutination testing and the API20 system.
Campylobacter
Approximately 0.2 ml of fecal suspension was added to 3 ml of Campylobacter enrichment broth (containing 5% lysed horse blood and cefoperazone 20 mg/L, vancomycin 20 mg/L, trimethoprim 20 mg/L, and cycloheximide 50 mg/L). Broths were incubated under microaerophilic conditions (N2 74%, O2 11%, H2 3%, and CO2 12%) at 37°C for 24 hours and then plated onto modified Campylobacter selective agar (mCCDA; containing cefoperazone 32 mg/L and amphotericin 10 mg/L) and incubated at 37°C for 2–3 days. Suspected colonies were transferred to Columbia agar (with 5% defibrinated horse blood) for incubation under the same conditions listed above. After 48 hours of incubation, colonies were subjected to routine Gram stain, catalase and oxygenase testing, growth in oxygenated conditions, and PCR.
Genetic testing was used only for those strains identified provisionally as Campylobacter. Genus-specific PCR 35 was carried out, followed by a species-specific PCR protocol to detect C. jejuni and C. coli. 27
Positive controls were in-house characterized E. coli strains, S. typhimurium DWC 2578, and a C. jejuni strain (11168 NCTC).
Antibiotic susceptibility tests
The disc diffusion and agar dilution method were carried out, respectively, as described by the British Society for Antimicrobial Chemotherapy (BSAC) guidelines (www.bsac.org.uk).9,8 The MICs of antimicrobial-resistant E. coli isolates by disk diffusion testing were determined using the agar dilution method 8 for each of the following antibiotics: ampicillin, chloramphenicol, ciprofloxacin, tetracycline, and trimethoprim. In this study, multiple drug resistance (MDR) was defined as resistant to at least four classes of antimicrobial agents as determined by the BSAC-disk diffusion method. 3 To determine florfenicol resistance in chloramphenicol-resistant isolates, we adopted the criterion of R≤18 mm. 3
Statistical data analysis
All data were assessed initially by descriptive statistics and univariate analysis using SAS statistical software (version 9.2; SAS Institute, Cary, NC). The Wilcoxon rank sum test was used to comparatively analyze the frequency counts of antimicrobial-resistant and MDR E. coli isolates between groups and variables (e.g., premises and sampling time). Logistic regression analysis was performed to determine associations between antimicrobial-resistant E. coli and risk factors related to the horse and environment. Separate models were evaluated for the dependent outcomes of antimicrobial-resistant E. coli and MDR E. coli, respectively. For each dependent variable, two overall analyses were carried out involving (1) hospitalized horses and (2) horses residing at the two different outside premises (A and B). Each dependent variable was represented as a bacterial-level proportion index (number of positive resistant colonies/number of colonies examined). A William's scale was used to correct for overdispersion of the data. Furthermore, the SAS-Glimmix macro was used to evaluate multi-level logistic regression models for each dependent outcome, in which the premises of origin were included as random effects.
The independent variables were horse related (age, sex, breed, and origin), treatment related (disease, diagnosis, drug type, drug amount, days hospitalized, route of drug administration, and treatment days), and bacteria characteristics (antimicrobial resistance pattern and number of isolates). Initially, all continuous independent variables were screened for possible inclusion in models by using a univariate analysis, as both linear and quadratic terms, against all outcome variables. Inclusion in preliminary models was determined based on the size of the parameter estimate±standard error.
Afterward, forward and backward selection procedures were used to identify variables with a p-value<0.05 for inclusion in final models. All continuous independent variables were centered against the mean value before inclusion in final models to reduce multi-collinearity. Final model selection was based on model deviance, parameter estimates, p-values, and examination of model residuals. The deviances between models were compared using a χ2-distribution, either directly or by taking into account the difference in degrees of freedom.
Results
The prevalence of enteric bacteria
The fecal samples had been previously tested for the presence of E. coli and multiple isolates had been found in all. 3 E. coli was isolated from all fecal samples. All samples were tested further from the hospital and nonhospital premises for other enteric pathogens (e.g., Salmonella and Campylobacter spp). Salmonella was not detected in any of the samples. By contrast, Campylobacter was isolated from 2.7% of the hospital samples (derived from three horses), but was not detected in any of the samples from the livery yard or riding stables. PCR analysis confirmed the Campylobacter isolates as C. jejuni, both of which exhibited resistance to trimethoprim and sensitivity to all other antibiotics tested.
Susceptibility to antimicrobials
The E. coli isolates defined as resistant to at least one antibiotic (n=296, 3) were used to generate antibiotic resistance and distribution profiles. As much as 82% of the hospital samples (89/109) harbored resistant isolates, whereas only 15% and 49% of the nonhospital samples (Premises A:17/112 and B:21/43, respectively) had E. coli isolates that were resistant to at least one antibiotic (Fig. 1). The differences between the hospital and nonhospital premises and Premises A and B were statistically significant (both, p≤0.0001). In addition, the hospital was significantly the major source of MDR E. coli (p≤0.0001; Fig. 1), and also significantly more MDR E. coli isolates were obtained from Premises B than from A (p≤0.01).
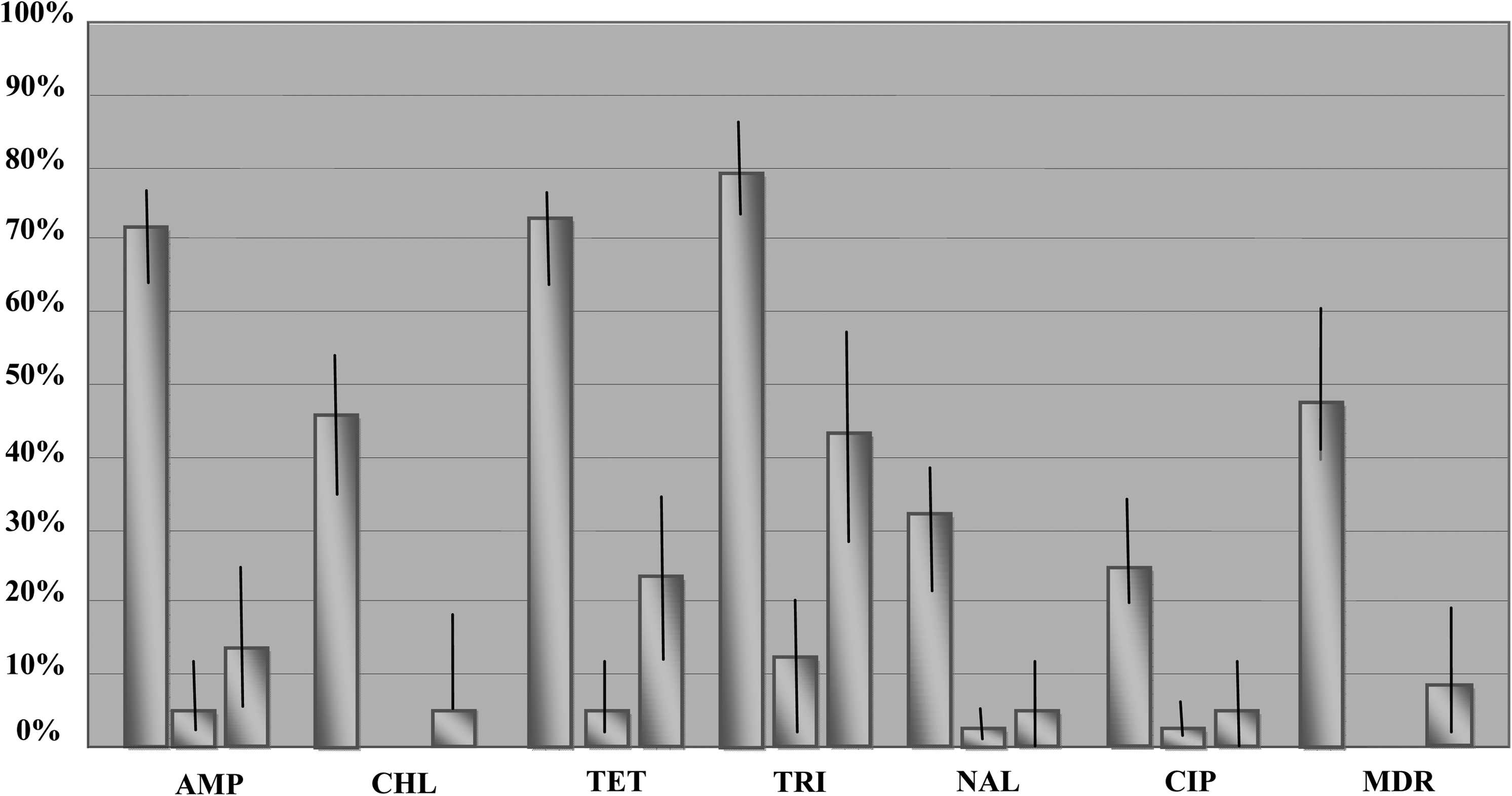
Prevalence of antibiotic-resistant Escherichia coli isolates in equine fecal samples. Bars represent the proportion of samples containing at least one antibiotic-resistant E. coli isolate with 95% confidence intervals. For each antibiotic tested, and for MDR isolates (isolates resistant to at least four classes of antimicrobial agents as determined) by the British Society for Antimicrobial Chemotherapy-disk diffusion method, data from the three sources—hospital*, riding school*, and livery yard*—are shown, respectively, from left to right. *Bars for hospital samples represent previously published data (Ahmed et al.) and are presented here for comparison purposes. AMP, ampicillin; CHL, chloramphenicol; TET, tetracycline; TRI, trimethoprim; NAL, nalidixic acid; CIP, ciprofloxacin; MDR, Multi-drug resistance.
Statistical analysis
Initially, a univariate analysis was performed to explore the potential factors associated with the presence of antimicrobial-resistant E. coli and multi-resistant E. coli (Tables 1 and 2). From this univariate analysis, multivariate logistic regression models were generated. By using only the premises (hospital and nonhospital; Premises A and B) then no useful models could be developed for the resistant or multi-resistant E. coli data. However, valid models were developed for antimicrobial-resistant and multi-resistant E. coli within the hospital setting (Table 3). Logistic regression analysis found that horses were significantly more likely to shed antimicrobial-resistant E. coli if they had presented with a gastrointestinal problem (p-value=0.007; odds ratio [OR]:±95% confidence intervals=8.50:1.79–40.32) or received a number of antimicrobial treatments (Tx) in hospital (p-value=0.017; OR/Tx=1.05:1.01–1.09) (Table 3). In addition, geldings were more likely than stallions to shed antimicrobial-resistant E. coli (p-value=0.024; OR=4.62:1.23–17.46). Interestingly, intravenous administration of antimicrobials appeared to be protective against shedding of antimicrobial-resistant E. coli (p-value=0.019; OR=0.18:0.04–0.76) (Table 3).
Results are expressed as either mean±standard error (SE) or frequency of positive horses for each type of E. coli.
ABs, antibiotics; GI, gastrointestinal; NSAID, nonsteroidal anti-inflammatory drug; IV, intravenous; IM, intramuscular; PO, per os (oral); MDR, Multi-drug resistance.
Results are expressed as either mean±SE or frequency of positive horses for each type of E. coli.
OR, odds ratio; CI, confidence interval; N/A, not applicable.
Logistic regression modeling revealed that within the hospital setting, horses were significantly more likely to shed MDR E. coli with increasing age (p-value=0.006; OR=1.11:1.03–1.19 per year) or after having received a number of antimicrobial treatments in hospital (p-value=0.003; OR/Tx=3.65:1.54–8.68). Furthermore, the time between the last antimicrobial treatment and fecal sample collection was associated significantly with fecal MDR shedding; for example, increasing numbers of days between the last antimicrobial administration and fecal sampling were significantly less likely to shed MDR E. coli (p-value=0.004; OR=0.28:0.12–0.66) (Table 3).
Discussion
Enteric bacteria are shed continuously in equine fecal matter, yet the proportions of different species (E. coli, Salmonella, and Campylobacter spp.) are variable and represented by antibiotic-sensitive strains. 13 This microbial profile can change when a horse is ill, undergoing antibiotic treatment, or living in settings that promote emergence of antimicrobial-resistant strains (such as hospitals). To explore the potential of horses as a source of antimicrobial-resistant bacteria and determine the risk factors associated with such resilient pathogens, we examined fecal samples from horses housed in hospital and nonhospital premises.
It was unexpected that no Salmonella were detectable in any of our samples. Salmonellosis is a well-documented nosocomial problem in hospitalized horses, 18 and associated with therapy after hospitalization. 34 In addition, it has been shown that exposure to antimicrobial drugs before hospitalization and abdominal surgery are associated with Salmonella shedding in adult horses. 22 However, the UK equine hospital used in this study has a very low occurrence rate of nosocomial clinical salmonellosis (personal communication with Prof. Peter Clegg) and this fact is consistent with our inability to detect Salmonella spp.
Other studies have also reported an apparent absence or very low levels of Salmonella in equine fecal and diarrheal samples.56,60 Nevertheless, our finding was unexpected since the PLEH specializes in colic (>300 cases/annum) and salmonellosis has been found to be more prevalent in horses with colic.16,34 It is possible that the low (no) isolation rate may be a feature of the particular geographic region, or simply a reflection of the need for better microbiological isolation methods for Salmonella. For example, targeted PCR amplification methods can be approximately threefold more sensitive than conventional culture. Yet, Salmonella was detected by targeted amplification in only 0.6% of broth-enriched samples 47 and findings of PCR have been discordant with those from culture.17,57
We used isolation and identification protocols that have been optimized for a wide range of fecal Campylobacter spp. 10 Nonetheless, only three samples were positive for C. jejuni and those came from hospitalized cases. Recently, Campylobacter fetus subsp. fetus was reported to be significantly associated with chronic diarrhea in horses. 29 That finding contradicted an earlier case–control study in which foal diarrhea was associated with bacterial infection, particularly Clostridium spp., and Campylobacter was found to not be significantly correlated. 41 Yet another study utilizing in-patient hospitalized horses found that Campylobacter fetus subsp. fetus was only able to be isolated from jugular venous blood after hospital admission, 31 and concluded that hospitalization did indeed play a role in Campylobacter shedding. Thus, the hospital setting is likely to be a risk factor of equine Campylobacter infection, although the exact mechanisms (such as stress-related events and specific treatments or drugs) causing increased susceptibility to infection and excretion remain undefined.
The prevalence of Campylobacter in horse fecal matter is relatively low as compared with the amounts present in the normal feces of other large, intensively farmed herbivores. 42 Other studies have found evidence suggesting that latent Campylobacter infections may be common in a variety of domestic and wild animals.2,30 Co-infections or septicaemic events have been postulated to induce shedding of latent bacteria; as such, these animals would represent effective reservoirs of Campylobacter for human infection. Moreover, a recent report from the United Kingdom found a significant correlation between that the presence of horses and increased incidence of Campylobacter spp. in cattle. 21 Although the rates of infection documented in horses in the United Kingdom have been low, 13 horses in Iran suffer from a particularly high infection rate. Indeed, the horse population in this country has been identified as the major carrier of Campylobacter spp. second only to poultry. 12 Taken together, these observations justify careful and continued surveillance of bacterial shedding in animal feces in order to facilitate responses to potential outbreaks and gain further insight into the zoonotic mechanisms through empirical studies.
In line with this idea, we also identified a higher prevalence of E. coli isolates having antibiotic-resistant and MDR phenotypes from hospitalized horses. All of the hospitalized horses in our sample population were referral cases for pre-existing gastrointestinal conditions, and it is likely that many would have undergone treatment, including antibiotics, before their arrival at. Thus, the higher prevalence of resistant E. coli in our hospitalized horses might reflect a prior positive selection event, rather than the immediate hospital environment. Transportation and other stress-inducing events have been associated statistically with increased shedding of antibiotic-resistant enteric bacteria 40 and also may have influenced the prevalence of shedding in horses within the PLEH.
Chloramphenicol and florfenicol are not prescribed currently in the United Kingdom for use in horses, yet resistance to chloramphenicol was found in almost half of our hospital samples. The majority of the chloramphenicol-resistant isolates and all florfenicol-resistant isolates were MDR, suggesting that co-selection may occur through the use of other antibiotics, especially if resistance to several antibiotics is encoded on a single plasmid or other mobile genetic elements. 15 Certainly, the lack of direct selection for chloramphenicol resistance does not appear to have eliminated E. coli isolates of this phenotype from being present in horses. 52 In our study, resistance to the fluoroquinolones (i.e., ciprofloxacin) was associated strongly with MDR and vice versa. Fluoroquinolone resistance in Enterobacteriaceae is usually the result of chromosomal mutations, although plasmid-mediated quinolone resistance, attributable to the qnr gene, has been reported in E. coli. 45
Logistic regression models indicated that horses with pre-existing gastrointestinal diseases were more likely to shed antimicrobial-resistant E. coli. This finding may have implications for hospital management, including implementation of patient isolation procedures to control the circulation of antimicrobial-resistant bacteria within the hospital and waste control measures to guard against spread of the isolates beyond the location boundaries. The differences observed between the prevalence of resistant E. coli in samples from Premises A (a riding stable) and Premises B (a livery yard) were marked. This feature could reflect a seasonal influence as the samples from Premises B were collected between spring and summer when the horses were experiencing changes in management routines. The type of work and, therefore, nutrition and stresses placed on the horses also differed between the two sites, and may have influenced the shedding rates.
Although resistant isolates were found in samples from all sites, the prevalence of resistance to individual antibiotics did vary between sites. Resistance to trimethoprim, tetracycline, and ampicillin were those most frequently encountered. Studies have predicted that resistance to fluoroquinolones in enteric bacteria is most likely to emerge from the usage of fluoroquinolone drugs. 58 This may also explain the higher rates of resistance in hospital isolates and presence of MDR isolates found in this study. It has been suggested that therapeutic and nontherapeutic uses of certain antibiotic drugs can also be associated with resistance (to these same antibiotics) in commensal bacteria, thereby increasing the reservoir of resistance genes.38,43 In our study, there was a poor association between antimicrobial drug types (e.g., quinolones) or doses administered to horses and the presence of antimicrobial-resistant E. coli. However, the relatively small scale of this study (in terms of the number of horses sampled) may explain the lack of association. A larger scale study would be needed to further investigate associations of equine gastrointestinal antimicrobial-resistant bacteria and drug usage.
In conclusion, this study indicated that horse fecal matter in this geographic location is likely not a significant source of Campylobacter, nor is Campylobacter shedding associated with gastrointestinal disease in horses. The absence of Salmonella in this population, even in hospitalized horses, suggests that salmonellosis is associated largely with infection of individual animals, who may then introduce it to larger horse populations, as opposed to it being an endemic disease. The hospital was also identified as a significant source of antibiotic-resistant bacteria and MDR E. coli isolates. Risk factors for increased shedding of antibiotic-resistant E. coli included hospitalization, antimicrobial treatment, and the presence of gastrointestinal dysfunction.
Footnotes
Acknowledgments
We would like to thank the staff at the School of Veterinary Sciences, University of Liverpool, who aided in sample collection. This work is dedicated to Professor Tony Hart of the Department of Medical Microbiology and Liverpool University, who dedicated his life's work to understanding the mechanisms of infectious disease in human and animal populations and whose brilliant insight and collaborative spirit will be greatly missed.
Author Disclosure Statement
The authors declare no relationship (commercial or otherwise) that may constitute a dual or conflicting interest.