
Abstract
The objective of this study is to develop an antibiogram (AB) method superior to a disc diffusion method (DDM) with respect to rapidity, reliability, and accuracy especially in view of an increasing threat from multidrug resistance (MDR) of infectious bacteria. A high-throughput liquid-phase fluorescent antibiogram method capable of providing results within 6–8 hours has been developed. The AB method has been optimally designed for ease of operation, growth, and dye stability. This new method was more reliable than DDM in differentiating AB sensitivity as susceptible, intermediate, and resistant within 6–8 hours and providing evidence for efflux mechanism in the MDR phenotype. The superiority of this method even over the standard liquid turbidity method was evidenced by more accurate determination of intermediary resistance in a set of 23 clinical Escherichia coli strains against five common antibiotics. In view of the demand for the right choice of an antibiotic in short time, the newly developed AB method is clinically applicable and useful in the rational use of antibiotic and minimizing of MDR emergence.
Introduction
In a recent case study conducted by us on MDR occurrence in protracted pediatric diarrhea, out of 73 Escherichia coli isolates, 80% were resistant to multiple antibiotics. 1 We also showed that even popular solid-state methods like the Kirby-Bauer disc diffusion method (DDM) are not quite reliable and accurate in determining antibiogram (AB), as these rely on the subjective interpretation of diameter of the zone of clearance around the antibiotic disc5,6 and affected by several physicochemical parameters of the antibiotics and the medium. 10
The more reliable and accurate turbidity assays, 11 however, suffer from detection limitation requiring cultures to attain a bacterial density of 108/ml and higher, essentially because of the poor sensitivity of light-scattering measurements measured using normal spectrophotometers or colorimeters. In this scenario, fluorescence-based viability-associated transport assays are expected to enhance the sensitivity by a few orders of magnitude3,16 and fluorescence measurement instruments are becoming more common. The bacterial viability or associated drug efflux has normally been studied by virtue of the ability of viable cells to take up nonfluorescent forms of certain dyes, metabolically convert them and efflux the fluorescent product.
Fluorescein derivatives, such as fluorescein diacetate (FDA), are commonly employed in biological research to study transport and viability of cells, predominantly in eukaryotic cells. To our knowledge, fluorescein dye-based AB methods have not been studied systematically to develop a clinical protocol or commercial product. Costlier dyes, such as Calcein, SYBR green, and SYTO blue 2 , for viability tests in eukaryotes and resazurin assay for the detection of multidrug-resistant Mycobacterium tuberculosis are a few reported applications. 14
To address the growing need of affordable AB methodologies for the peripheral laboratories in countries like India, we preferred to use the readily available and relatively cheaper fluorescein-based dyes. In our previous study, 1 FDA was used to demonstrate the correlation of efflux with MDR. In that experiment, since the ester, FDA, is labile and hydrolyzed by the medium, it was added to the sample wells after 7 hours of bacterial growth (i.e., toward the end) in the presence of antibiotics and incubated for half an hour. The released fluorescence was then measured. However, this required an additional step of adding the dye, which is not desirable in a commercially viable clinical method and the sensitivity too was poor, comparable to that of the turbidity measurements. In this report, we have systematically studied such methods, come up with solutions to certain critical practical problems, and developed a convenient and clinically useful AB method that is capable of generating reports within 6–8 hours to aid in the timely choice of the right antibiotic.
Materials and Methods
Bacterial strains and the antibiotics used
E. coli strains were isolated from stool samples of children, who were hospitalized for acute or persistent diarrhea at the Institute of Child Health and Hospital for Children (ICH and HC). E. coli strains were identified by conducting standard biochemical tests, such as Indole, Methyl Red, Voges-Proskauer, and Citrate 5 , and were confirmed by PCR. 8 Antibiotics used were procured from the following different suppliers: Amikacin (Aristo Pharma), Ampicillin (Ranbaxy Pharma), Amoxicillin (GlaxoSmithKline Pharma,), Cefotaxime (Lupin Labs), Ceftazidime (GlaxoSmithKline Pharma), Ciproflaxicin (Ranbaxy Pharma), Colistin (MP Biomedicals (India) Pvt. Ltd), Gentamicin (Fulford Pharma), Kanamycin (Macleods Pharma), and Nalidixic acid (Ranbaxy Pharma). The antibiotics concentration (for killing the bacteria) were calculated using the formula W=(1,000/P)×V×C, where W is the weight of antibiotic (mg) to be dissolved in V (ml), the volume required; P, potency of the antibiotic base given by the manufacturer (μg/mg); and C, final concentration in mg/L. 7 The antibiotics dose in the disc and concentration for liquid-phase methods used throughout the study is given in Table 1.
Antibiotics used in discs are as per the CLSI standards.
Antibiotic concentrations used in liquid assays were calculated using the formula.
DDM, disc diffusion method; LTM, liquid turbidity method; FAM, fluorescence antibiogram method; CLSI, Clinical and Laboratory Standards Institute.
Routine culture media tested for growth and dye stability
Tryptone yeast extract-based media
The Luria Bertani broth (LB medium—10 g of tryptone, 5 g of yeast extract, and 10 g of sodium chloride (NaCl) in 1 L of distilled water and the pH adjusted to 7.2 with 1 M sodium hydroxide). The Terrific broth (TB medium—12 g of tryptone, 24 g of yeast extract, 9.4 g of K2HPO4, 2.2 g of KH2PO4, and 4 ml of glycerol in 1 L of distilled water, the pH was adjusted to 7.0). The Hanahans broth (HB medium—20 g of tryptone, 5 g of yeast extract, 5 g of NaCl, 2.4 g of MgSO4, and 186 g of KCl in 1 L of distilled water and the pH was adjusted to 7.0). The Super broth (SB medium—35 g of tryptone, 20 g of yeast extract, 5 g of NaCl in 1 L of distilled water and the pH was adjusted to 7.0). All the media were autoclaved at 121°C and 15 lbs pressure for 20 minutes.
Casein acid hydrolysate-based media
The Casein acid hydrolysate (CA) medium with NaCl was prepared by dissolving 10 g of casein acid hydrolysate, 5 g of yeast extract, 4 g of potassium hydrogen phosphate, 5 g of NaCl in 1 L of distilled water and the pH was adjusted to 7.5 using sodium hydroxide and autoclaved. 12 Casein acid hydrolysate and the glucose medium (CAG) was prepared by dissolving 1 g and 5 g of CA separately dissolved in 1 L of distilled water and autoclaved. About 2% and 5% final concentration glucose (using 0.2-μm syringe filter) was added to each according to the volume required. CAG with the NaCl broth was prepared by dissolving 1 g of CA and 2 g of NaCl in 1 L of distilled water and autoclaved. To this, 0.5% of glucose (using 0.2-μm syringe filter) was added according to the volume required.
LB agar
It was prepared by dissolving 20 g agar–agar (Himedia) in the LB medium, sterilized, and cooled to ∼45°C. Twenty milliliters of the molten agar was poured into presterilized Petri plates. The plates were checked for sterility by incubating them at 37°C for 6–7 hours before experimentation.
Growth rate experiments
For selecting the best media in terms of growth rate, cost, and ease of preparation, different media were studied in a 96-well format with DH5α as the experimental model. In 5 hours at 37°C, complex media like LB, TB, HB, and SB supported comparable growth from a moderate inoculum size of 105 cells, but required a longer time from low inoculum doses.
Viability assay using FDA and 5-carboxy fluorescein diacetate, acetoxymethyl
FDA is a known marker to study bacterial viability.3,16 Two tubes of 3 ml overnight culture (DH5α) were taken and one tube was autoclaved to kill the cells. One milliliter of culture from each test tube was taken and pelleted in 1.5-ml centrifuge tubes and resuspended with 200 μL of phosphate-buffered saline pH 7.4 having 25 μM FDA. The tubes were incubated in the dark for 30 minutes. Visible fluorescence was observed in the tube containing viable bacterium, but not in the tube with dead cells. The fluorescence was read at Ex/Em=485/510 nm using a commercial fluorimeter (Fluroscan; Thermo Lab systems).
The FDA dye was replaced with 5-carboxy fluorescein diacetate (5-CFDA) as it exhibits more charges when hydrolyzed to its acid form, which helps the fluorescent product to hold better inside the cells. The new dye was tested for its uptake, stability as done for FDA and found to be more stable. However, changing the dye did not address the issue of the medium spontaneously hydrolyzing the dye. So the medium was optimized for a better stability of the dye. The FDA and 5-CFDA dyes were procured from Molecular Probes, Invitrogen.
Optimized growth and stability for AB determination
Many complex media routinely used in the laboratory were found to spontaneously hydrolyze the dye within a short time of 1–2 hours. Therefore, the composition of the popular bacteriological medium, LB, was modified for best growth as well as the stability of the dye in the medium during AB determination. Tryptone and yeast extract, which caused the spontaneous hydrolysis of the ester dye, were reduced to 1 g per liter each instead of 10 and 5 g/L, respectively. The concentration of NaCl was left unchanged at 5 g/L, but 1 g/L of CA (It did not hydrolyze the dye, but provided buffering to maintain the pH 6.5 and supported the growth in the lean LB) was added as a supplement and this medium was named as the AB medium. To prepare the medium, the ingredients were simply dissolved in 1 L of distilled water; pH was normally 6.5. An Indian patent had been filed for the medium composition and the methodology developed. 15
Standardized procedure for AB determination
The AB method was performed in a 96-well plate (eight rows and 12 columns with lid), wherein six strains (in duplicates in columns) were screened against five antibiotics (rows) at a time. One hundred eighty microliters of the AB medium was taken in the wells and 10 μL of 500 μM 5-CFDA dye in 100% dimethylsulfoxide was added to each well to give a final dye concentration of 25 μM. Antibiotics to be tested were added row-wise, each row for one antibiotic. Finally, 104 cells of the test strains were inoculated column-wise, one strain per column. The medium with dye served as blank and the medium with dye and cells, but without the antibiotic served as control for growth. The plate was incubated at 37°C with constant shaking at 170 rpm for 6 hours. Fluorescence was measured every hour using a fluorimeter (Thermo) and the optical density of bacterial cultures was measured using Multiscan (Labsystems, Thermo).
Results
Viability-dependent fluorescence measurement is a useful tool for AB determination
A major demand of the clinicians in tackling infectious diseases is the timely detection of appropriate antibiotics for treatment. As we had reported recently, the existing DDM, though popular, is not quite satisfactory from the point of accuracy, rapidity, throughput, and cost. The turbidity assay, which is routinely employed in laboratories, has poor sensitivity, though accurate. Therefore, our attempt to develop a superior, but a more affordable AB method relied on improvising a popular viability assay using fluorescein derivates.
The working principle of the method was first demonstrated using FDA. Figure 1 shows that whereas the vial containing dead cells did not fluoresce there was intense fluorescence due to live cells. As can be seen in the composite picture in the figure, the serial dilution of the viable cells showed that 106 live cells/ml could be visualized even by the naked eye; the limit of detection using the laboratory fluorimeter was found to be 105 cells/ml. However, at this level of sensitivity, it still necessitates a certain amount of growth of the bacterium before detecting the antibiotic susceptibility, especially while testing samples from early infectious or samples containing lower numbers of bacteria. As the ester forms of fluorescein dye are known to be labile in aqueous solutions, the problem of dye stability for hours in the growth medium had to be addressed by modifying the exisiting media without adversely affecting the bacterial growth rate.
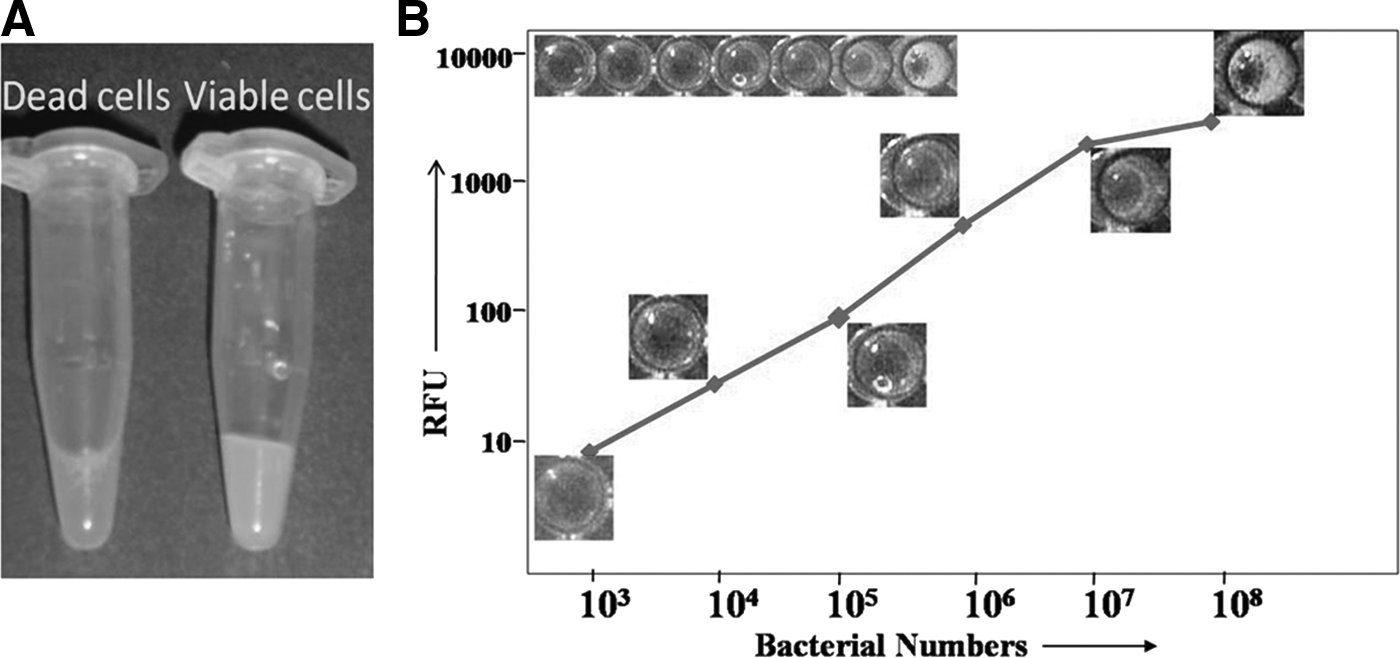
The fluorescent viability assay and its utility in AB determination.
LB medium was modified for optimal dye stability and bacterial growth for AB determination
Generally, complex organic media (like LB) provide better growth rates compared to simple inorganic (M9) or organic media (casein hydrolysate). Among the former, LB was found to be the best choice from the point of view of cost, ready availability, familiarity, and preparation. Other tryptone and yeast extract-based media (costlier variants of LB) to enhance the growth rates did not offer significant advantage for growth within 5–6 hours. Inclusion of vitamins, minerals, and trace elements also did not improve the growth rates significantly.
FDA, being a labile ester, got hydrolyzed in the LB medium within the growth period to yield high backgrounds. Within 3 hours, most of the FDA was hydrolyzed in media control. This hydrolytic activity was obviously due to the organic components of the complex medium, yeast extract, and tryptone, but not due to the inorganic component, NaCl. Since many bacteria grow well in minimal media supplemented with 10–20% of LB, it was decided to reduce the organic components to 1 g each, instead of 5 g, and this drastically reduced the hydrolysis rate and resulted in a lower background. However, this modification resulted in a reduction of growth rate, to almost 50% of the rate in normal LB. We had earlier observed that casein hydrolysate did not hydrolyze the dye significantly, but supported moderate growth in the presence of glucose. Thus, we formulated a new medium called the AB-medium with 5 and 10 times lower amount of yeast extract and tryptone, respectively, but containing the same amount of NaCl and supplemented with 1 g/L of casein hydrolysate; glucose as carbon source was not necessary under these conditions.
Though these modifications brought down the dye hydrolysis drastically, the background noise was high enough to interfere with the interpretation of results of intermediary resistant types and possibly of slow growing bacteria. Therefore, a more stable derivative of FDA, 5-CFDA was employed to reduce the background noise. The data in Fig. 2A shows that CFDA was more stable in both LB and AB medium compared to FDA to reduce the background. Figure 2B shows the stability of the CFDA dye is excellent in AB compared to LB and the Muller Hinton broth (MHB). The relative fluorescence unit (RFU) due to 2½ hours of hydrolysis of FDA by LB was equivalent to 8 hours of hydrolysis in the AB medium, CFDA in the AB medium showed much lower hydrolysis rates; even after 8 hours, the RFU was basal comparable to 30 minutes of hydrolysis of FDA in LB. So, the AB medium, as formulated, was found to be suitable for AB determination within 6–8 hours, as designed for the test.

The AB method was tested on a panel of clinical E. coli isolates and other enterobacteria against commonly prescribed antibiotics
Once the AB medium was standardized for dye stability and growth, the assay was designed for a 96-well microtiter plate. We tested two panels, one consisting of six strains of E. coli and the other consisting of six different enterobacterial species (other than E. coli), in duplicate, against seven commonly prescribed antibiotics. Initially, the DDM as per the Clinical and Laboratory Standards Institute (CLSI) recommendations was taken as the reference for fixing the S, I, and R forms. However, as reported earlier, the liquid turbidity method (LTM) and the fluorescence antibiogram method (FAM) indicated more susceptible forms for aminoglycosides compared to DDM, which showed them to be resistant. However, we could eliminate this mismatch by doubling the antibiotic dose in the discs used in DDM. Since the superiority of the FAM over DDM could be proven, S, I, and R were fixed according to the former.
However, considering the variability due to measurement as RFU, time duration, status of the medium hydrolysis, the cutoff values are determined after the experiment based on internal controls. The image of the fluorescence intensities (Fig. 3) and the RFU values (Table 2) for the E. coli panel and the panel of other bacteria, respectively, indicated the expected performance of the assay. The intensities generally correlated with the corresponding turbidity measured in a parallel experiment indicating that the fluorescence was a function of growth. Resistant forms showed good growth, and hence resulted in intense fluorescence; intermediary ones showed a lesser growth, and therefore moderate fluorescence; the nonfluorescent wells indicated susceptibility, all matching the known antibiotic sensitivity of the strains taken. This successful demonstration of feasibility of the method led us to validate an imaging-based instrumentation method to categorize strains according to fluorescence intensity as susceptible, intermediate, and resistant.
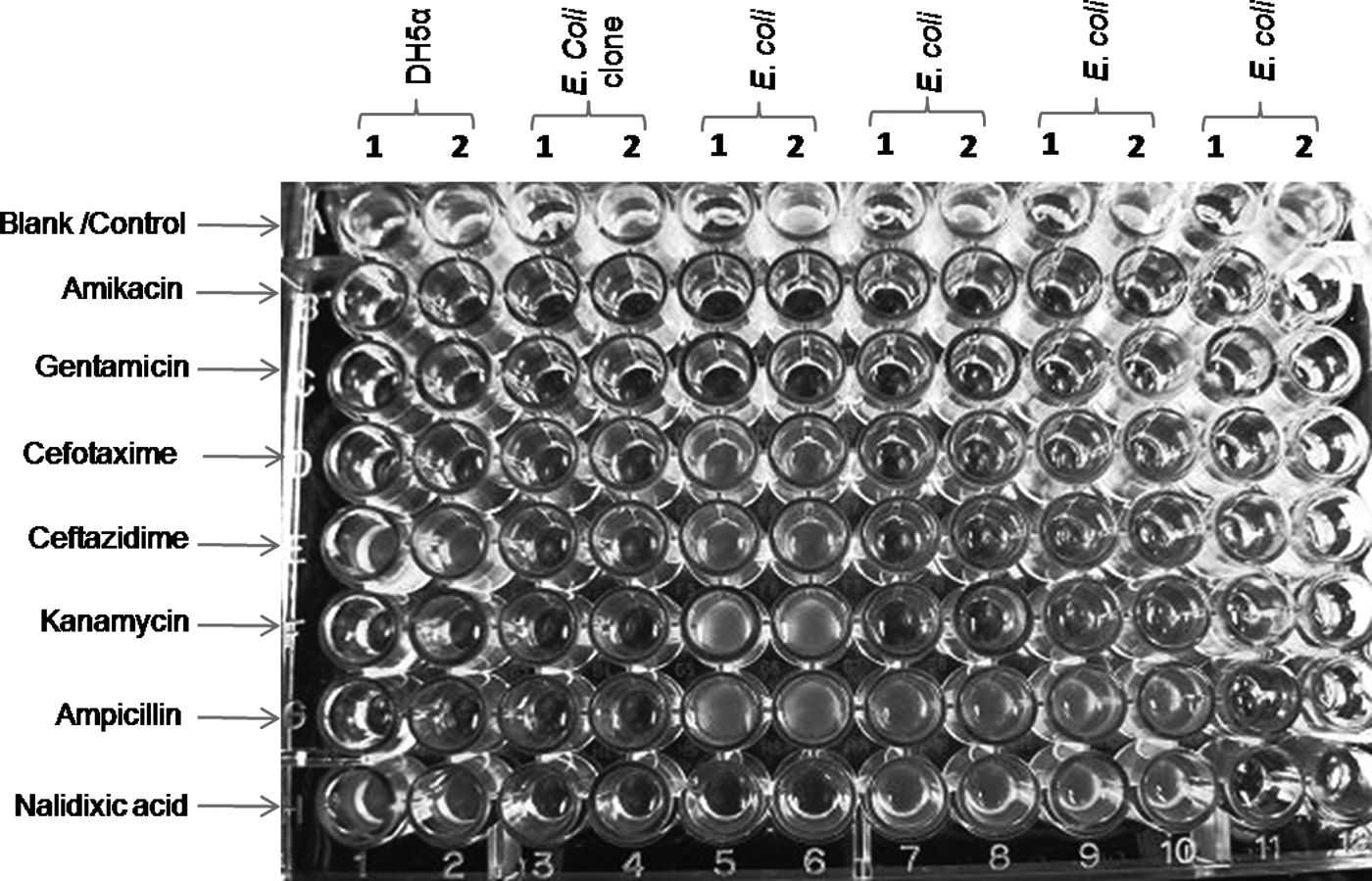
Image of the 96-well microplate format of fluorescent AB method with Escherichia coli strains. The figure shows the visual profile of fluorescence as captured using a camera in a gel documentation system with long UV (365 nm) excitation. The fluorescence intensities, high, moderate, and low can be used to infer resistant, intermediate, and susceptible forms, respectively. The AB profile of six different E. coli strains (named in the top row) in duplicates against seven routinely used antibiotics with corresponding blanks and controls (labeled vertically). The match of such a deduction with the actual AB determined with standard methods was excellent.
The values represent the RFU.
The cutoffs were established based on the results in comparison with the DDM.
S, susceptible (RFU ≤10); I, intermediate (RFU 11–25); R, resistant (RFU >25); MIC, minimal inhibitory concentration; RFU, relative fluorescence unit.
The newly developed FAM validated with clinical strains
When a panel of 12 laboratory E. coli isolates was tested for its AB using the FAM in comparison with the DDM, LTM (OD read at 600 nm), and MHB turbidity method (OD read at 600 nm), we found a good match, as revealed in the Table 3. LTM and MHB had 95.8% exact match. The remaining were resistant, R in the case of MHB and intermediary I in the case of LTM. Clinically, I and R are treated as R, so we can consider the match to be as high as 99%. However, one strain (E. coli 8) against Ciproflaxicin was R by MHB, S by LTM, but I by FAM. This implied better accuracy of FAM over LTM.
The antibiogram using DDM was scored by the zone of clearance; MHB and LTM by OD 600 nm; FAM by RFU.
Gray shaded indicates difference in antibiogram results between MHB and LTM.
S, susceptible; I, intermediate; R, resistant; MHB, Muller Hinton broth.
A panel of 23 clinical diarrheagenic E. coli isolates was tested for its AB using FAM, LTM, and DDM. The comparative results are given in Table 4. Out of 23 strains tested against five antibiotics routinely used to treat diarrhea, 80% match was found in the AB between the two methods. The remaining 20% predominantly belonged to the ampicillin group. These were intermediate by FAM, but susceptible by LTM. This contradictory finding implicating poorly growing, but antibiotic tolerant E. coli prompted us to test these cultures on agar plates for viability. The results are shown in Fig. 4. Those that were read as susceptible by both the methods, (strains 407238, 426749, and 408619 against amikacin, gentamycin, and cefotaxime respectively), there was no growth seen on the agar plates. Against ampicillin, all the strains of the controversial group (except 407238) that was intermediate by the new FAM, but susceptible by the classical LTM showed lawns instead of nil or a few colonies. The strain, 407238, showed a few colonies. The strain 407459 against amikacin, though read as susceptible by both the methods, still showed around 25–30 colonies on the agar plate. This observation clearly showed that the more sensitive fluorescence method is able to provide a more reliable AB.

Plates showing viability of bacteria from samples that scored either intermediate (I) or resistant (R) by the fluorescence method (FAM), but susceptible (S) by the classical LTM. Those samples against the antibiotics (from Table 4) indicated at the bottom of the plates that scored either intermediate (I) or resistant (R) by the fluorescence method (FAM), but sensitive (S) by the classical LTM were further experimented. To verify the presence of viable bacteria, the samples were plated onto antibiotic-free plates and examined for colonies. No colonies in the plates, 407238/amikacin, 426749/gentamicin, 408619/cefotaxime, and 407459/amikacin showed that these bacteria were susceptible by both the methods, and hence good correlation. The presence of colonies in other plates confirmed the I or R results of FAM. LTM, liquid turbidity method; FAM, fluorescence antibiogram method.
The organisms examined are diarrheagenic E. coli strains.
The CLSI–MIC concentration and the employed concentration of the antibiotics are given in the parenthesis.
S, susceptible; I, intermediate; R, resistant.
Discussion
Fluorescence-based viability assay offers a more rapid and reliable method for AB determination, preferably within a working day or before the second dose
MDR is emerging as a major problem in the treatment of infectious diseases and currently, clinicians are more interested to know the right drug for beginning the treatment, avoiding trial and error during the critical period. Administering a wider spectrum antibiotic based on just the symptoms is generally the treatment pattern for a variety of bacterial infections for determination of the AB or MDR phenotype is time-consuming and expensive. The currently popular disc diffusion technique takes at least 2 days or the duration required for 3–4 doses of antibiotics. We had recently reported the deficiencies in DDM, especially false positivity, and recommended the use of liquid-based assays. In continuation, in this study, we have developed a new fluorescence-based liquid assay method for AB determination. Owing to the superiority of FAM over DDM, S, I, and R will be fixed according to the former.
In this method, we have exploited the viability tests normally conducted using colored or fluorescence dyes and adapted it for bacterial AB taking clinical E. coli as a test group. For saving the critical time by enhanced sensitivity of detection, we have chosen fluorescein dyes as the viability indicators in the presence of antibiotics. 9 This property was exploited in our report on the comparison of DDM and the liquid assay and demonstration of efflux as a good indicator of the MDR phenotype. In this, the dye was added toward the end keeping in mind the well-known lability of ester in an aqueous solution. 1
The newly developed LB as AB medium provides a convenient method for determination of AB within 8 hours
Originally, FDA, a well-documented and established dye, was used for testing bacterial viability because of its intense fluorescence in the visible range (green) when excited in the visible (blue) light. This property of the dye is helping in the development of inexpensive fluorimeters based on LED sources and photodiodes. The detection sensitivity of 106 viable cells/ml visually and an order more (105/ml) using simple laboratory fluorimeters prompted us to develop a quicker and sensitive AB method. The problem of dye lability was overcome by reducing drastically the organic components of LB, but supplementing with casein hydrolysate and employing more stable dye form, CFDA. Together, the AB medium (Indian patent applied) containing the dye, provided a convenient means of growing bacterial samples and measuring the fluorescence within 6–8 hours and determine the AB. Even visual differentiation and imaging are possible. It was also possible to categorize the strains into resistant, intermediate, and susceptible types; a very useful result for the clinician and this solves the problem faced by DDM (requires manual interpretation and the inaccuracies associated with solid-phase assay). Since clinically, I is also considered as R, only S or R really matters in the field. Hence, the cutoff values will be fixed after subtracting the blank value from the reference wells containing antibiotic-susceptible bacterial control.
None of the antibiotics tested had any effect on the hydrolysis of the dye or affected the stability of the AB-medium and vice versa. The dry powder of the medium could be stable for months, when kept under refrigeration. It is desirable that, the medium with the antibiotics could be dried on the plate so that it could be rehydrated when the AB has to be determined. Such tests have not been performed yet, but need to be performed for product development.
The new AB method has the potential to be adapted for clinical use
Since E. coli is fast emerging as a dangerous pathogen (enteropathogenic E. coli, enterohemorrhagic E. coli, enterotoxigenic E. coli, enteroinvasive E. coli, and uropathogenic E. coli) affecting children and adults, and it is a very common bacterium, initially we wanted to test the usefulness of the method on a set of E. coli strains that were isolated from clinical diarrheal samples of hospitalized children below 5 years of age. The fact that the new AB-medium was working satisfactorily was evident from the determination of AB of a representative panel of E. coli and other enterobacterial strains as well as a larger panel of 23 E. coli strains against five antibiotics. Owing to the enhanced sensitivity, the FAM scored even better than the LTM in identifying intermediary types, as revealed by the plating method. This is critical to antibiotic treatment. Identifying the intermediates as susceptibles is risky, as the false negative results will lead to a choice of wrong antibiotics, one of the causes for MDR complications. This method has also been verified on the clinical isolates of a few other gram-negative bacteria like Uropathogenic Escherichia coli (UPEC), Shigella, and Salmonella in our laboratory (unpublished results). Considering the seriousness of the clinical situation due to MDR bacteria and the disadvantages of the popular DDM due to the subjectivities associated with solid-phase assays, the new FAM is a better choice for obtaining AB results within 6–8 hours or within the second dose of the antibiotics. 1
This method has definitive advantages over the DDM (gold standard). The faster determination (6–8 hours vs. 24–48 hours) of AB without the physicochemical limitations and manual errors in result interpretation associated with DDM saves precious treatment time and provides more accurate results. It would match the speed and sensitivity of methods like the Biomérieux's Vitek® system, which determines the AB in 5–8 hours, but at a much lower cost and operational ease suitable to limited skills and funds available in peripheral laboratories.
Conclusion
A medium called AB medium was improvised from the popular LB medium for developing a new AB method. This new method based on the fluorescence viability/efflux assays in routine laboratory use was optimized to provide AB results within 6–8 hours with a reliability superior to disc diffusion or even LTM. The new AB method validated on a set of clinical isolates of diarrhogenic E. coli and a few other enteropathogens holds promise to be adapted as a clinical method to administer the right antibiotic within a day or by the second dose.
Footnotes
Acknowledgments
This work was supported by the Department of Science and Technology, India, under their Technology Development Programme, Technology Systems Group. We acknowledge. Dr. Jayanthi, Dr. Saradha Suresh, Dr. Md. Meeran, Dr. Umadevi of Institute of Child Health and Hospital for Children (ICH and HC), Chennai, India for their support in sample collection and discussions on clinical practices. We thank Dr. Rolf Reissbordt, Robert Koch Institute, Germany, for the reference EPEC strains. We acknowledge the useful interactions and help by Dr. Pavan Kumar.
Disclosure Statement
There is no conflict of interests for the authors for submitting this article. This work was supported by the Department of Science and Technology, India, under their Technology Development Programme, Technology Systems Group. They have no involvements in the study design, in the collection, analysis, and interpretation of data; in the writing of the article; and in the decision to submit the article for publication.