
Abstract
The nature and frequency of mutations in the rpoB gene of rifampicin (RIF) resistant Mycobacterium tuberculosis clinical isolates varies considerably between different geographical regions. The objective of the present study was the identification of rpoB gene mutations responsible for RIF resistance in M. tuberculosis isolates in Sri Lanka. Three regions of the rpoB gene of M. tuberculosis, one corresponding to a 437-bp region, including the rifampicin resistance-determining region (RRDR) and two other regions (1395 bp and 872 bp) spanning the RRDR, were polymerase chain reaction amplified, and were subjected to DNA sequencing. The two mutations found within the RRDR in the 31 RIF resistant strains isolated in this study were at codon 526 (n=15, 48.4%) CAC (His)→TAC (Tyr) and codon 531 (n=3, 9.7%) TCG (Ser)→TTG (Leu). A significant proportion (n=15, 48.3%) showed mutations spanning the RRDR, including two novel mutations at codon 626 (n=13, 41.9%) GAC (Asp)→GAG (Glu) and 184 (n=2, 6.4%) GAC (Asp)→GAT (Asp), a silent mutation. Two isolates revealed double mutations (codons 626+526 and 626+184). The presence of a high frequency of new mutations, and the different frequencies of the universally prevailing mutations, as reported here, emphasizes the need for expanding the geographical database of mutations for effective application of an rpoB-based diagnosis of multidrug resistant tuberculosis.
Introduction
Multidrug resistant tuberculosis (MDR-TB) is defined as resistance to at least rifampicin (RIF) and isoniazid (INH). The WHO has recognized MDR-TB and XDR-TB, or extensively drug resistant tuberculosis (MDR-TB plus resistance to any fluoroquinolone, and resistance to at least 1 of the 3 injectable drugs: capreomycin, kanamycin, and amikacin) as being a major challenge for controlling TB. Around 440,000 MDR-TB cases are estimated to emerge each year, and 150,000 people die annually from MDR-TB. 32 The four countries that have the largest number of estimated cases of MDR-TB are China, India, the Russian Federation, and South Africa. 34 The WHO progress report of 2011 states that 69 countries had reported at least one case of XDR-TB by the end of 2010, and it is estimated that 25,000 cases of XDR-TB will emerge each year. In an outbreak in South Africa, 52 out of 53 XDR-TB patients died within an average of 3 weeks of being diagnosed. 32
Although Sri Lanka is not a high-burden country, TB remains a significant public health problem. The estimated incidence rates of all forms of tuberculosis in 2009 were 66 per 100,000 population, 35 and 9643 new TB cases were notified. 15 The overall treatment success rate among smear-positive cases was 85% among the new smear-positive cases and 70% among retreatment patients in the year 2008. 35 A study conducted by the National Reference Laboratory-Sri Lanka during the period 2005–2007 revealed that 3.4% of MTB strains were resistant to RIF and 4.5% were resistant to INH, while 2.5% were multidrug resistant. 6
RIF is the most important drug in the short-course treatment regimen due to its efficient antimicrobial action. 20 RIF interferes with initiation of DNA transcription. It is stated that approximately 90% of the world's RIF resistant isolates are also resistant to INH, making RIF resistance a useful marker of MDR-TB.25,27 Most of RIF resistant MTB strains from different countries appear to harbor specific point mutations in the rifampicin resistance-determining region (RRDR) of the rpoB gene, which comprises an 81-bp region containing codons 507–533.11,12,16,30 In addition, studies have also revealed a significant contribution to RIF resistance through mutations in the region outer to RRDR of the rpoB gene, suggesting that, the nature and frequency of mutations in the rpoB gene of RIF resistant M. tuberculosis clinical isolates vary considerably, between different geographical regions.10,11,17–19 Further, it has been reported that there is discordance between results of phenotypic methods and genotypic methods that are based on RRDR mutations used for the detection of drug resistant TB. 10
The WHO recommends performing drug susceptibility testing (DST) for at least RIF and INH in resource limited settings, especially in previously treated patients and HIV coinfected patients. An early diagnosis of drug resistant TB and the management of MDR TB patients are challenging obstacles faced by tuberculosis control programmes. 31 Presently numerous molecular-based identification methods such as INNO-LiPA Rif.TB (INNOGENETICS) and GenoType MTBDRplus (HainLifescience) have been commercialized for identification of RIF resistance. However, these methods are based on the detection of commonly found mutations at codon 531, 526, and 516. 34
In Sri Lanka, RIF resistance is identified by the proportion method that requires more than 28 days for detection of drug resistance. Rapid molecular methods have yet to be established for identification of drug resistant tuberculosis. Before establishing molecular-based methods for detection of drug resistance, it is important to characterize the mutations in the rpoB gene in MTB isolates in a particular geographical setting. Therefore, the present study was focused on evaluating the nature and the frequency of mutations in the rpoB gene that are associated with resistance to RIF in M. tuberculosis strains isolated from Sri Lanka. The results of the present study will also contribute to expand the knowledge on the profile of mutations in the rpoB gene.
Materials and Methods
Collection of sputum samples
The sample collecting period was from March 2008 to September 2010, and only pulmonary TB cases were considered. The study population represented primary TB patients (patients that had never received treatment for TB or who had received anti-TB treatment for <1 month) as well as secondary TB patients (i.e., relapse, retreatment, treatment failure, and defaulters) (defaulter: A patient who returns to treatment, positive bacteriologically, following interruption of treatment for 2 months or more). Sputum samples were collected from secondary TB patients admitted to the Chest Hospital Welisara (the only chest hospital in Sri Lanka) for supervised treatment and from primary and secondary TB patients presenting to the Central Chest Clinic, Colombo (the location to which secondary TB patients are referred for re-evaluation and treatment from peripheral clinics). In addition, sputum from all TB suspects (cough >3 weeks) were collected from the Prison Hospital Colombo as prisoners are at a high risk of harboring drug resistant TB strains.
Isolation of M. tuberculosis strains
The sputum specimens were processed using the modified Petroff's method. Sodium hydroxide (4%) (Sigma)-treated sputum was centrifuged at 3000 g under refrigerated conditions (at 4°C). The centrifuged deposit was diluted in 1ml of sterile distilled water for preparing the bacterial suspension for inoculation. Two slopes of the Lowenstein–Jensen (L-J) medium (Difco), one containing paranitrobenzoic acid (PNB, Sigma), were inoculated with 100 μl of the bacterial suspension. A small portion of the bacterial suspension was examined microscopically, using the Ziehl-Neelsen (ZN) stain, to determine the presence of acid fast bacilli. The inoculated media were incubated at 37°C in a 5% CO2 incubator up to 8 weeks until growth was observed. Cultures were confirmed as MTB if they were slow growing, nonpigment producing, reduced nitrate, and did not grow in the presence of PNB. The isolates were further confirmed as MTB by detection of the insertion element IS6110 by polymerase chain reaction (PCR) as published previously. 14 One Isolate from each patient was used for the study. The H37Rv strain and a known RIF resistant MTB isolate confirmed by the National Tuberculosis Institute, Bangalore, India were used as quality control strains.
DST for M. tuberculosis strains
DST was carried out using the agar proportion method, 7 the nitrate reductase assay (NRA), 2 and the manual Mycobacteria Growth Indicator Tube (MGIT). 1 Rifampicin (Sigma) stock solution (10 mg/ml) was prepared using dimethyl sulphoxide (DMSO) (Sigma), and filter sterilized aliquots were stored at −70°C. A working solution (1 mg/ml) was prepared by diluting the stock solution with sterile distilled water. The final concentration of RIF in each drug containing the culture medium used for the DST was 1 μg/ml 7 (Data not shown).
DNA extraction
Genomic DNA was extracted from identified RIF resistant isolates using the phenol chloroform extraction method. 29 Harvested heat-killed bacteria from the L-J slopes were incubated overnight with proteinase K (Sigma). Genomic DNA was extracted using phenol–chloroform (Sigma) and precipitated with absolute ethanol (Sigma) followed by washing with 70% ethanol. The precipitated DNA was resuspended in the TE buffer (pH 8.0). The quality and concentration of the extracted DNA was tested using an agarose gel (1.5%) electrophoresis, and the DNA was stored at −20°C.
PCR amplification and DNA sequencing
Extracted DNA was used for amplification of three different segments (437 bp, 872 bp, and 1395 bp) of the rpoB gene (Fig. 1). The amplified segments covered around 60% of the total length of the rpoB gene. Specific primers were designed using available literature21,28 and primer-3 software. For amplification of the 437-bp region, including RRDR, rpoBF primer and rpoBR primer were used. The TR9 and RRBN primer pair was used to amplify the 872-bp region downstream of the RRDR region. The 1395-bp fragment upstream of RRDR was amplified using the FRBN and TR8 primer pair (Table 1) (all primers were purchased from Promega).

Position of primers used for amplification of the three regions of the rpoB gene in rifampicin resistant Mycobacterium tuberculosis isolates.
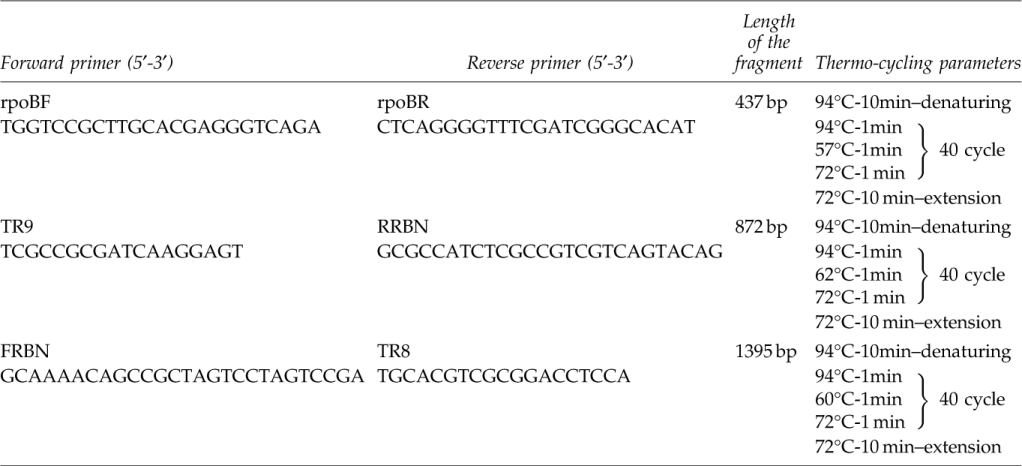
A 50 μl PCR mixture containing 50 mM KCl, 10 mM Tris (pH 8.0),1.5 mM MgCl2, 200 μM of deoxynucleotides triphosphates (dNTPs) (Promega), 1 U Taq polymerase (GenScript), 20 pmol of each primer (Promega), and 2.5 μl of genomic DNA (10 ng) was used for each PCR reaction. The thermo-cycling parameters used for amplification of the three segments of the rpoB gene are shown in Table 1. The amplified PCR products were electrophoresed on ethidium bromide stained agarose gels (1.5%) and visualized under a UV illuminator.
Each resistant strain was PCR amplified in duplicate and both amplified products were custom DNA sequenced (Macrogen DNA sequencing service in Korea). A DNA sequence analysis was done using NCBI and Sea View software (version 4.2.12). All resistant isolates were also subjected to IS6110 restriction fragment length polymorphism typing using the PvuII restriction enzyme. 29
Results
Three hundred and seventy-three (373) MTB strains were isolated from sputum samples during the period March 2008 to September 2010. The majority of patients were from the Western Province (Colombo, Gampaha, and Kalutara districts) of Sri Lanka, which has a high prevalence of TB. 15 Thirty one RIF resistant isolates were identified among the 373 MTB strains by one or more phenotypic method (APM, NRA, and manual MGIT). Thirteen RIF resistant isolates were from primary cases of TB and the remaining 18 isolates from patients with secondary TB.
DNA sequencing of amplified fragments of the rpoB gene revealed that mutations in the RRDR region accounted for resistance in 18 (54%) isolates and were confined to two codons, 526 (n=15, 48.4%) and 531 (n=3, 9.7%). The remaining mutations were detected in the regions outer to RRDR and occurred at codons 626 (n=13, 41.9%) and 184 (n=2, 6.4%). Twenty nine isolates showed single-point mutations at codon 526 (n=14, 45.2%), 626 (n=11, 35.5%), 531 (n=3, 9.7%), and 184 (n=1, 3.2%). Dual mutations (at codon 526+626 and at codon 184+626) were detected in 2 strains (Table 2).
The mutated codons with corresponding amino acids are indicated.
Codons within RRDR.
Codons outer to RRDR.
novel mutations.
RRDR, rifampicin resistance-determining region; TB, tuberculosis.
The mutation observed at codon 526 (CAC→TAC) and codon 531 (TCG→TTG) was a C-to-T transition mutation, while the novel mutation at codon 626 (GAC→GAG) was a C-to-G transversion mutation and at codon 184 (GAC→GAT), a transition mutation. All point mutations in this study revealed only a single mutation pattern, and there were no multiple patterns of base changes at a single codon.
NCBI Accession numbers for DNA sequences: HQ377336-HQ377338, HQ377340- HQ377345, HQ377351, and JQ314433-JQ314444.
Discussion
It is widely reported that MTB expresses a high degree of geographic diversity in mutations to the rpoB gene.9,13,22,26,36,37 Mutations of codon 531, 526, and 516 have been reported as the most frequent mutations in the mutation hotspot region of the rpoB gene of MTB worldwide.3,23,36 In the present study, the majority of mutations occurred at codon 526, and the mutation frequency (48.4%) observed was slightly higher than frequencies reported by China (40%), 36 Japan (35%), 16 and Korea (38%). 9 However, the frequency of occurrence of the mutation at codon 526 in India, the closest neighbor to Sri Lanka, is much higher (93%) as reported by Sharma et al. (2003).
Although the majority of published reports have shown CAC to GAC (transversion mutation) as the most prevalent base change at codon 526 (29.7% among Italian isolates 18 and 12% in Greece isolates 12 ), our study revealed that the base change was CAC to TAC (transition mutation) in all isolates, similar to reports from India. 24
The frequency of mutation at codon 531 (9.7%) was comparatively low in MTB isolates from Sri Lanka in relation to mutation frequencies reported by other countries, including India (47%), 10 Australia (52%), 37 Vietnam (31%), 4 and Poland (41%). 23 However, the base change observed at codon 531 was a TCG to TTG (transition mutation) as commonly reported by several Asian countries (Japan, 16 China, 36 Korea, 9 and India 11 ) and other countries such as Greece 12 and Italy. 18 Previous studies have reported that a mutation at codon 531 is frequently associated with the codon 526 mutation in certain regions of the world. 22 However, this phenomenon was not observed in our study.
The mutation at codon 626 (n=13, 41.9%) GAC (Asp)→GAG (Glu) was the second major mutation found in the present study. Codon 626 is located downstream of RRDR and mutation in this codon has not been previously reported. This novel mutation was present in 13 isolates, and these strains showed different DNA fingerprinting patterns with 1–15 copies of the IS6110. The absence of identical banding patterns demonstrates the presence of epidemiologically nonrelated strains. Thus, it is plausible that M. tuberculosis strains with mutation at codon 626 represent epidemiologically different strains.
Two isolates showed a silent mutation at codon 184 GAC (Asp)→GAT (Asp) that is located upstream of RRDR. In one isolate, the mutation at codon 184 was associated with a mutation at codon 626. Several mutations in the upstream region of RRDR also have been reported from India. 10
Mutations at codon 516 have been reported as prominent in several geographical areas such as India, 13% 10 and Iran, 10% 5 and therefore, commercially available RIF resistance diagnosis kits have been optimized to detect mutation at codon 516 among other mutation in the RRDR. However, no mutations were observed at codon 516 in the present study.
Several publications have stated that ∼4% of phenotypically resistant isolates did not show any mutations within the RRDR.4,8 Yue et al. (2003) have reported that 10% of phenotypically resistant MTB strains did not show any mutations at RRDR. According to Lingala et al. (2010), 21% of phenotypically RIF resistant isolates did not show any mutations when a 255-bp region of RRDR and 350-bp region of non-RRDR of the rpoB gene were sequenced. This may be due to mutations occurring in the region outer to RRDR, as was observed in 41.9% of RIF resistant isolates of MTB in the present study. A single discordant result was observed between phenotypic and genotypic results in the present study (phenotypically resistant, but no mutation), although the isolate showed a silent mutation at codon 184. This isolate was confirmed as resistant to RIF by APM and MGIT. It is possible that an additional point mutation is present in this isolate at a codon in the rpoB gene not investigated in the present study.
Current molecular diagnostic methods such as INNO-LiPARif are designed to detect common rpoB mutations at codon 531, 526, and 516. Therefore, they may not be applicable universally across various settings, considering the geographical diversity of the mutations.10,24
Although the mutations in our strains are limited to a few types, the occurrence of a high percentage of mutations outside the RRDR presents important implications for the use of currently available rapid molecular methods, which target mutations in the RRDR region. Molecular tests used for rapid detection of drug resistance need to be customized to enable detection of novel mutations in different geographical areas. Therefore, identification of drug resistant mutations and their relevant frequencies is an important first step before introducing molecular DST in different geographical settings.
In conclusion, two novel point mutations outer to the RRDR and two universally prevailing mutations in the RRDR of the rpoB gene were observed in Sri Lankan RIF resistant MTB isolates. The new mutations and different frequencies of universally prevailing mutations that are reported here emphasize the need for expanding the geographical database of the mutations for effective application of the rpoB-based diagnosis of MDR-TB in public health settings. It may be necessary to customize the rpoB-based molecular diagnostic methods so as to make them suitable to detect locally prevalent mutations.
Footnotes
Acknowledgments
The authors thank Dr. Inoka Corea, Sirithilak Gamage, Srirani Hendalage, S.M.P Senevirathne, and Gihani Perera and the laboratory assistant staff (Department of Microbiology, Faculty of Medicine, the University of Colombo) for providing assistance. Funding: The study was supported by the National Science Foundation of Sri Lanka.
Ethical Approval
The Ethics Review Committee of the Faculty of Medicine, the University of Colombo, Sri Lanka, approved the study (ERC number is EC/06/062).
Disclosure Statement
All authors report no conflicts of interest relevant to this article.