
Abstract
The purpose of this study was to determine the presence of integrons in Escherichia coli, which cause urinary tract infections, and to define the association between integrons and antimicrobial susceptibility. Susceptibility of 200 isolates from urine samples of patients suffering from urinary tract infections to 13 antibiotics was determined by the Kirby–Bauer disk diffusion method. The existence of class1 and 2 integrons in resistant isolates was assessed by polymerase chain reaction–restriction fragment length polymorphism and sequencing. Antibiotic resistance patterns were observed as follows: amoxicillin 78%, tetracycline 76.1%, co-trimoxazole 67.7%, cephalotin 60%, nalidixic acid 57.4%, chloramphenicol 49%, gentamicin 46.4%, ceftazidim 38.1%, ciprofloxacin 36.2%, nitrofurantoin 33.5%, amikacin 32.1%, norfloxacin 36.1%, and imipenem 27.1%. Of 200 isolates, 155 (77.5%) were multidrug resistant (MDR). The existence of integrons was confirmed in 50.3% of isolates. Three class 1 integron types, aadA2 being the most frequently found, and four class 2 integron types are described. Significant association between resistance to gentamicin, co-trimoxazole, cephalotin, ceftazidim, imipenem, chloramphenicol, and nalidixic acid with the existence of integrons was observed. Multidrug resistance suggests that the strategy for treatment of patients with E.coli infections needs to be revised. Furthermore, it was shown that integrons may be partly responsible for multidrug resistance. Imipenem and norfloxacin were the most effective antibiotics against isolates.
Introduction
An efficient route of acquisition and vertical and horizontal dissemination of resistance determinants is through mobile elements including plasmids, transposons, and gene cassettes in integrons. Several antibiotic resistance genes observed in Gram-negative microorganisms are part of a gene cassette inserted in an integron. The most common cassettes contain genes that confer resistance to a range of antimicrobial agents, including aminoglycosides, ß-lactams, chloramphenicol and trimethoprim, as well as genes that confer resistance to antiseptics and disinfectants. At the present time, about 60 different cassettes associated with resistance genes have been identified, and the same cassettes can be found in different classes of integrons. 5 Several classes of integrons related to antibiotic resistance have been identified that can be distinguished by the nucleotide sequence of their respective integrase.2,8,15 Four distinct classes of integrons encoding different integrases have been reported, and class 1 and 2 integrons are the most frequent in clinical strains, being found in many different organisms.7,10,14
Through incorporation into transposons and plasmids, integrons participate in the capture and dissemination of resistance genes among bacteria. The fact that genes yielding resistance to antibiotics commonly used in the treatment of human infections could be acquired by integron-harboring strains may potentiate the possibilities of selection by a variety of different antimicrobials. Therefore, integron acquisition is considered the major cause of multiple resistance in Gram-negative microorganisms, mainly in enteric bacteria. 1
Polymerase chain reaction (PCR) is now broadly applied for the molecular analysis of antibiotic resistance genes in bacteriology. 9 PCR-restriction fragment length polymorphism (RFLP) is a two-step version of PCR which could reveal minor differences within sequences of amplified PCR products by the generation of bands with different size in agarose gel. 18 Escherichia coli is frequently isolated from patients with urinary tract infections, therefore, in the present study, we assessed the presence of integrons in E.coli which cause urinary tract infections and the association between integrons and antimicrobial susceptibility.
Materials and Methods
Antimicrobial susceptibility testing
Between April and November 2010, 200 E.coli isolates from patients (99 men, 101 women) suffering from their first episode of Urinary Tract Infection (UTI) and free of recent antibiotic exposure, who have attended three hospitals affiliated with Shahid Beheshti University of Medical Sciences, were obtained. The mean age of studied patients was 27±2 years, 25±1 in females and 26±3 in males. Urine samples were collected 4 hours after previous urination. All urine samples were obtained from a midstream into standardized, sterile containers and delivered to the laboratory at the Department of Medical Microbiology, Medical University of Shahid Beheshti within 2 hours after being collected. In the first stage quantitive urine culture was performed where all urine samples were plated onto blood and MacConkey agar plates. Urine cultures that contained less or equal than 10,0000 (≤105) CFU/ml of bacteria were insignificant bacteriuria. Urine growth with two or more uropathogens was interpreted as contamination and was not further worked up. Patients in such cases were asked to provide another urine sample for correct assessment. In cases where the number of growing colonies of bacteria exceeded 105 CFU/ml (significant bacteriuria), the samples were further worked up. Isolates which were identified as E.coli based on standard biochemical tests, were further worked up. 16 The isolates were screened for antimicrobial susceptibility using Kirby-Bauer disk diffusion methodology. 12 The group of antimicrobials tested were Gentamycin (10 μg), Tetracycline (30 μg), Ceftazidime (10 μg), Co-trimoxazole (25 μg), Imipenem (10 μg), Ciprofloxacin (5 μg), Norfloxacin (10 μg), Cephalotin (30 μg), Amikacin (30 μg), Chloramphenicol (30 μg), Nalidixic Acid (30 μg), Amoxicillin (10 μg) and Nitrofurantoin (32 μg).
Detection of class 1 and class 2 integrons
The presence of class 1 integron was tested by PCR (Fig. 1), using the primers 5′CS–3′CS 10 and the specific primer for the int1 gene in all the sulfamethoxazole-resistant isolates. To characterize the conserved segment 3′CS, a PCR, using specific primers, was performed to determine the presence of sul1 and qacEΔ1 genes in all those isolates. Class 2 integron were detected by PCR (Fig. 1) with specific primers for the int2 gene, 10 and subsequently the cassette regions were amplified using primers hep74 and hep51 for the attI2-orfX region. PCR amplification was carried out in 50 μl reaction mixtures containing 5 μl DNA, 50 pm of each oligonucleotide primer, 50 mM KCL, 10 mM Tris-HCL, pH 9.0, 0.01% (v/v) Triton X-100, 1.5 mm MgCl2, 0.2 mM dNTPs (dATP, dCTP,dGPT,dTTP) and 2.5 U Taq polymerase. PCR assay was performed as described by Japoni et al. 6
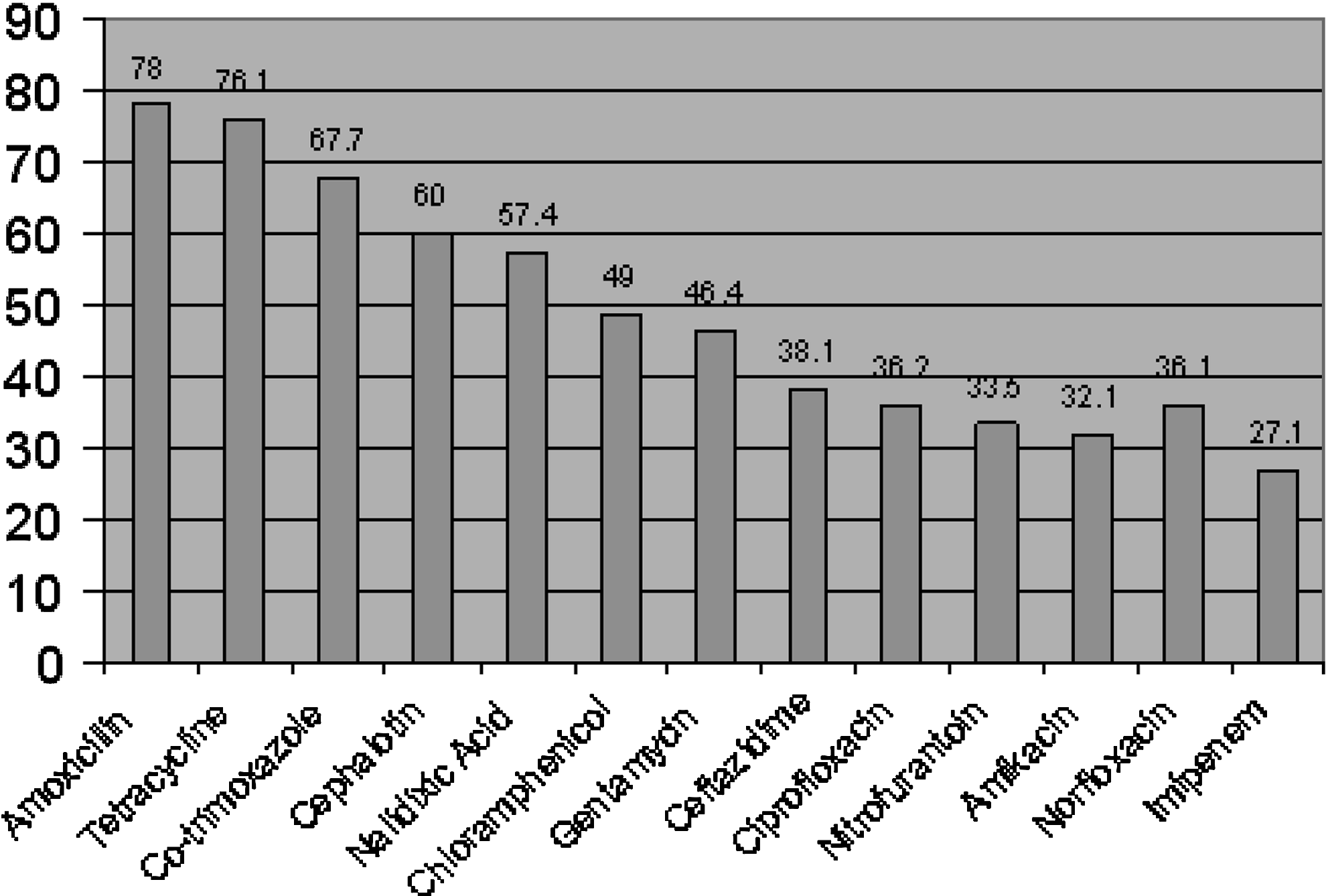
Antibiotic resistance pattern of Escherichia coli isolated from urine samples.
DNA purification and PCR-RFLP analysis
PCR products generated in the first PCR step (direct amplification samples as well as agarose gel fragments) were purified with the GFX PCR DNA and gel band kit (Amersham Pharmacia Biotech, Barcelona, Spain).
The RFLP analysis of the different amplicons was carried out using several endonucleases: TaqI (T↓CGA) (Roche Diagnostics, Barcelona, Spain) and BglII (A↓GATCT), PvuI (CGAT↓CG), and HincII (GT [T/C]↓[A/G]AC) (Amersham Pharmacia Biotech). For this, aliquots of the amplicons obtained in the first PCR step were directly purified and digested separately with 5 U of each endonuclease, according to the manufacturer's recommendations. The restriction products were analyzed by electrophoresis on 1.5% agarose gels. An amplified DNA fragment corresponding to the variable regions of each distinct class 1 or class 2 RFLP-type integron was sequenced using an ABI Prism 377 automated sequencer (Applied Biosystems, Perkin-Elmer, Foster City, CA). Nucleotide sequences were compared with sequences in the GenBank and EMBL databases using the BLASTN local alignment search tool (http://blast.ncbi.nlm.nih.gov/Blast.cgi).
Results
Resistance to Amoxicillin was observed in 78% of isolates Tetracycline in 76.1%; Co-trimoxazole in 67.7%, Cephalothin in 60%, Nalidixic Acid in 57.4%, Chloramphenicol in 49%, Gentamycin in 46.4%, Ceftazidim in 38.1%, Ciprofloxacin in 36.2%, Nitrofurantoin in 33.5%, Amikacin in 32.1%, Norfloxacin in 36.1% and Imipenem in 27.1% (Fig. 1). Of 200 isolates 155 (77.5%) were multidrug resistant. The existence of integrons was confirmed in 50.3% of the isolates by PCR-RFLP. Class 1 and 2 integrons were detected in 56 (36.1%) and 20 (12.9%) isolates, respectively. Co-existence of class 1 and 2 integrons was detected in 2 isolates (1.3%). Seventy seven isolates (49.7%) did not harbor integrons (Table 1). The size, type and number of generated fragments are shown in Table 2.
PCR, polymerase chain reaction.
Associations of drug resistance to Gentamycin, Co-trimoxazole, Cephalotin, Ceftazidim, Imipenem, Chloramphenicol and Nalidixic Acid with the presence of integrons which was calculated by chi-square and Fisher exact tests, respectively, were statistically significant (Table 3).
Integron class 1 positive in PCR-RFLP assay.
Integron class 2 positive in PCR-RFLP assay.
Statistically significant values are in bold.
PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism.
Discussion
Antibiotic resistance and, in particular, multidrug resistance are major problems for the empirical treatment of patients. 6 The existence of integrons was confirmed in 78 (50.3%) of our multi-drug resistant isolates, indicating the prevalence values is in the high range.
As previously noted, integrons of class 1 and 2 were more prevalent than those of class 3,4,11 thus in our study, the association of integrons of class 1 and 2 with antibiotic resistance was investigated. In a research by Fluit and Schmitz, it was shown that the prevalence of class 1 Integron and also the increase in its prevalence in the genome of resistant E-coli, klebsiella oxytoca, Enterobacter aerogenes and Enterobacter cloacae, were higher compared with the other classes of integrons, during 1993, 1996 and 1999. 4 In our study, it was demonstrated that class 1 integron is significantly associated with antimicrobial resistance which is consistent with previous studies.
In 2006, Paauw et al. demonstrated that Multidrug resistance among Enterobacteriaceae is strongly associated with the presence of integrons and is independent of species or isolate origin. This study investigated the extent to which multidrug resistance (MDR) among Enterobacteriaceae is related to DNA elements called “integrons,” whether the relationship is species dependent or origin dependent, and which resistance patterns are associated with integrons. Analysis of 867 nonrepeated isolates comprising 8 species, originating from the community and 23 European hospitals showed a significant relation between multidrug resistance (MDR) and integrons, independent of species or origin. Although resistance to each tested antimicrobial agent was significantly associated with integrons, only resistance to sulfamethoxazole, cotrimoxazole, gentamicin, tobramycin, ampicillin, piperacillin, and cefuroxime predicted the presence of integrons. Combined resistance to both ampicillin and sulfamethoxazole-trimethoprim was the starting point for the development of resistance to additional β-lactams, aminoglycosides, cephalosporins, and ciprofloxacin, a development paralleled by an increasing prevalence of integrons. It was shown that the acquisition of resistance genes is not random, and the transfer of integron-carrying elements plays a dominant role in the development of MDR by Enterobacteriaceae. 13
Isolates in this study were highly sensitive (189; 94.5%) to imipenem.Extreme sensitivity of E.coli isolates to imipenem has earlier been reported by Tariq et al. 17 and Japoni et al. 6
However, nowadays in our clinics, quinolones (nalidixic acid, ciprofloxacin and norfloxacin) are often prescribed to treat gastrointestinal and UTIs. A consistent stepwise increase in E.coli resistance to ciprofloxacin was obsereved from 1995 (0.7%) to 2001 (2.5%) by Bolon et al. 3 Ciprofloxacin resistance in our isolates was 36.2% which is on high side compared with Japoni et al. who obsereved that 21% of 200 E.coli isolates were resistant to ciprofloxacin.
Evidently there is a positive correlation between antibiotic resistance and class 1 and 2 integrons. However, a significant association between resistant isolates to nearly half of the antibiotics including amoxicillin and tetracycline and the presence of integrons was not found statistically (Table 3). Imipenem and Norfloxacin were the most effective antibiotics against isolates in vitro. Nevertheless, the clinical efficacy of these antibiotics remains to be assessed.
The aim of this study was to define the role of Integrons as one of the most important genetic elements responsible for antibiotic resistance among the E.coli strains isolated from urine samples of patients suffering from UTI.
Muti drug resistant E.coli, that is, isolates resistant to three or more unrelated antibiotics, were quite common in our study. One hundred fifty-five (77.5%) showed MDR. This implies that certain changes in treatment strategy of patients with E.coli infections is necessary.
Footnotes
Acknowledgments
This study was supported by the Paediatric Infections Research Centre (PIRC) of Mofid Children's Hospital in Tehran affiliated with Shahid Beheshti University of Medical Sciences. We are grateful to the Iran National Science Foundation (INSF) for their financial support.
Disclosure Statement
No competing financial interests exist.