
Abstract
CTX-M-type extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae have been previously reported in Venezuela. We assessed the frequency and diversity of CTX-M enzymes among 97 ESBL-producing Enterobacteriaceae isolates as well as to establish the genetic relationship among CTX-M producers collected from six hospitals in Caracas. Polymerase chain reaction (PCR) assays identified the blaCTX-M genes in 42 isolates (43.3%). The blaCTX-M-1 group was the most common in Escherichia coli (91 %) and the blaCTX-M-2 in Klebsiella pneumoniae (56.6%). Presence of blaCTX-M-1, blaCTX-M-2, blaCTX-M-15, and blaCTX-M-14 was revealed by sequencing analysis. The CTX-M producers were mainly isolated from urine samples (46%). Antimicrobial susceptibility tests showed that a high proportion of CTX-M-producing isolates was resistant to ciprofloxacin and trimethoprim-sulfamethoxazole. Analysis of enterobacterial repetitive intergenic consensus PCR and repetitive extragenic palindromic PCR profiles revealed several genetic clusters between isolates carrying the blaCTX-M-1 group, while complete genotypic diversity among isolates carrying the blaCTX-M-2 group was observed. This study documented that CTX-M has achieved a citywide distribution, with the CTX-M-1 group as the most frequent (66.7%). The CTX-M clusters detected suggest that patient–patient transmission may have played an important role in the widespread and high prevalence of the CTX-M-1 group. To our knowledge, this is the first report of the CTX-M-15 in Venezuela.
Introduction
These results were presented in part at the 49th Interscience Conference on Antimicrobial Agents and Chemotherapy, San Francisco, CA, 2009.
Materials and Methods
Clinical strains
We selected 97 ESBL-producing Enterobacteriaceae isolates (53 E. coli and 44 K. pneumoniae) recovered from clinical samples between March 2006 and March 2007 to assess the presence of CTX-M enzymes. Isolates were re-identified using 12 key biochemical differential tests to identify E. coli and K. pneumoniae species. 30 Only one ESBL-producing isolate from each patient admitted to the general medical ward or intensive care unit (defined as hospitalized patients) and outpatients (defined as nonhospitalized patients) was included. Demographic data, including age, gender, and types of clinical specimens, were collected for all patients who were infected with CTX-M producers. The samples were isolated in six hospitals (Hospital Dr. Domingo Luciani [n=13], Policlinica Metropolitana de Caracas [n=15], Centro Medico de Caracas [n=9], Hospital Universitario de Caracas [n=24], Hospital de Clinicas Caracas [n=20], and Centro Medico Docente La Trinidad [n=16]) from Caracas and sent to the Biology of Plasmids Laboratory of the Central University of Venezuela for inclusion into this study. The health centers were selected to give wide geographical coverage of Caracas (Fig. 1).
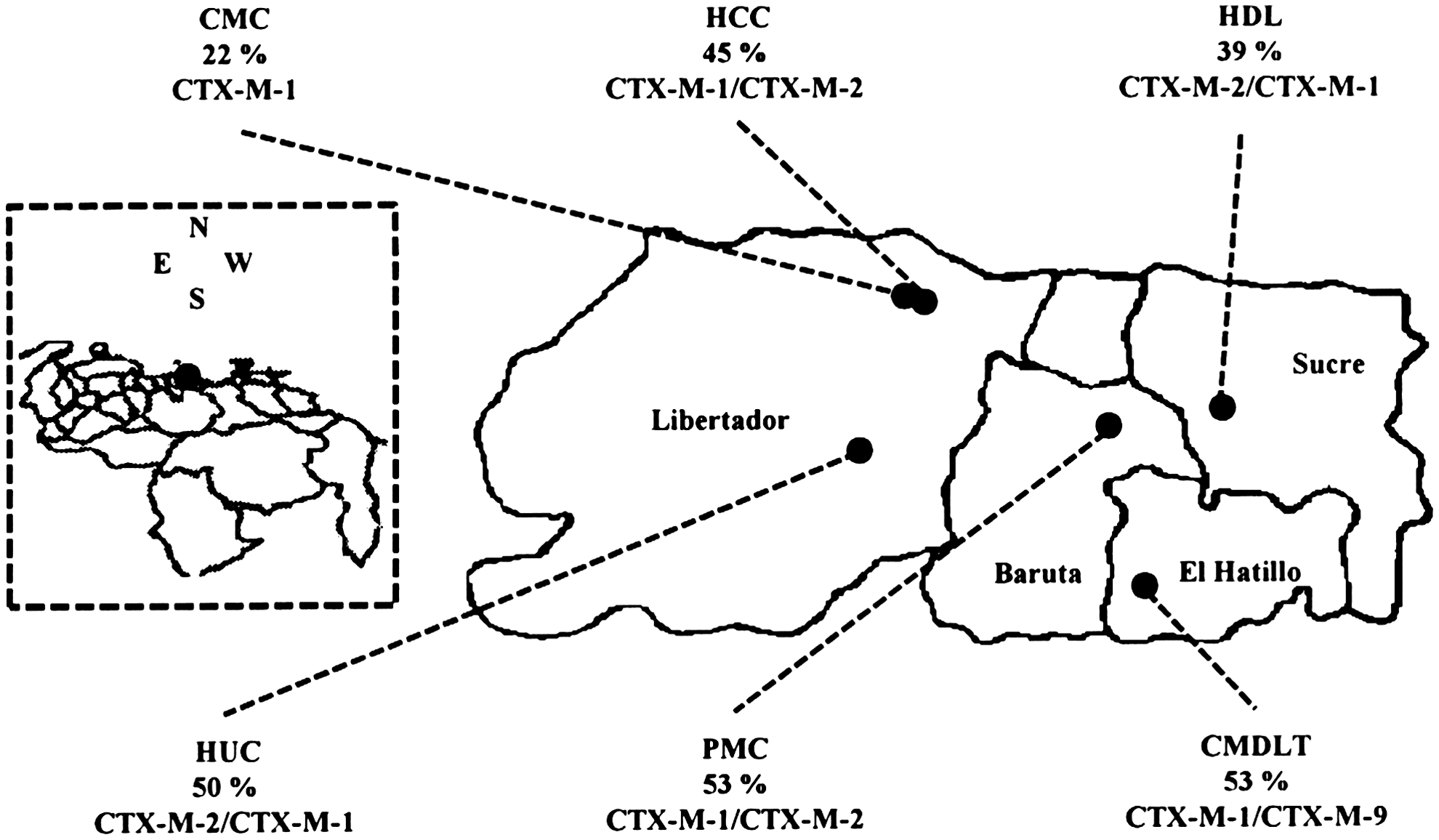
Map of the Caracas municipality showing the location of the health centers participating in this study. The prevalence of CTX-M producers observed among the extended spectrum beta-lactamase-positive Enterobacteriaceae and the CTX-M groups detected from each center are shown. The location of Caracas is marked as a dot on the left dashed box. HDL, Hospital Dr. Domingo Luciani; PMC, Policlinica Metropolitana de Caracas; CMC, Centro Medico de Caracas; HUC, Hospital Universitario de Caracas; HCC, Hospital de Clinicas Caracas; CMDLT, Centro Medico Docente La Trinidad.
Antibiotic susceptibility testing
The ESBL phenotype was confirmed with both cefotaxime and ceftazidime alone and in combination with clavulanic acid according the Clinical and Laboratory Standards Institute (CLSI) disk diffusion test. 6 The MIC50 and MIC90 values of four antimicrobial agents (ceftazidime, cefotaxime, aztreonam, and cefepime) for CTX-M-producing isolates were determined by the E-test method (AB Biodisk, Solna, Sweden). CTX-M producers were tested against six non-beta-lactam agents (amikacin, chloramphenicol, ciprofloxacin, tetracycline, tigecycline, and trimethoprim-sulfamethoxazole) and four beta-lactam agents (imipenem, ertapenem, amoxicillin-clavulanic acid, and cefoxitin) by the standard disk diffusion method, and the results were interpreted based on the CLSI guidelines. 6 For tigecycline, interpretive criteria from previous study were applied. 12 E. coli ATCC 25922 and K. pneumoniae ATCC 700603 were used for quality control processes as recommended by the CLSI. 6
Polymerase chain reaction amplification for detection of the ESBL genes blaCTX-M and sequencing
The ESBL-producing isolates were initially screened for the presence of blaCTX-M by first amplifying with the CTX-M group primer pair. For detection and differentiation of the blaCTX-M groups, positive CTX-M group isolates were screened using three pairs of primers specific for alleles encoding CTX-M enzymes belonging to the CTX-M-1, CTX-M-2, and CTX-M-9 groups and the same pair for CTX-M-8 and CTX-M-257,8,19 (Table 1). Whole-cell DNA was prepared as previously described. 9 Polymerase chain reactions (PCRs) were run in a Mastercycler Personal Thermal Cycler (Eppendorf, Hamburg, Germany) using a cycling program: denaturation at 94°C for 1 min, followed by 30 cycles of denaturation at 94°C for 50 sec, and the primer-specific annealing temperature for 45 sec, with an extension at 72°C for 1 min. Cycling was followed by a final extension at 72°C for 1 min. PCR products of the blaCTX-M alleles were subject to bidirectional nucleotide sequencing with ABI 3130XL (Applied Biosystems, Foster city, CA).
PCR, polymerase chain reaction; REP, repetitive extragenic palindromic sequences; ERIC, enterobacterial repetitive intergenic consensus sequences.
Repetitive extragenic palindromic-PCR and enterobacterial repetitive intergenic consensus-PCR
The DNA templates were prepared using the same technique as described above. 9 PCR was used to amplify repetitive extragenic palindromic (REP) and enterobacterial repetitive intergenic consensus (ERIC) elements 28 (Table 1). Cycling conditions included an initial denaturation at 94°C for 5 min, followed by 30 cycles of 94°C for 1 min, the primer specific annealing temperature for 45 s, and an extension at 72°C for 7 min. Cycling was followed by a final extension at 72°C for 15 min. PCR products were separated on 1.5% agarose gels in 1×Tris-borate-EDTA buffer. PCR fingerprinting was analyzed with the BioNumerics software package using the Dice binary coefficient and unweighted pair group method with arithmetic average to create dendograms (Applied Maths, Inc., Austin, TX). The positions of bands on each gel were normalized by using the 1-kb DNA ladder as an external reference standard.
Results
Characterization of CTX-M-type beta-lactamases
All ESBL-producing isolates were characterized by PCR to detect blaCTX-M genes, including the blaCTX-M-1 group, blaCTX-M-2 group, blaCTX-M-9 group, and blaCTX-M-8. Among the 97 ESBL-producing Enterobacteriaceae analyzed, the blaCTX-M gene was detected in 24 E. coli and 18 K. pneumoniae isolates. Of the E. coli isolates that carried a blaCTX-M gene, 22 (91.7%) carried a blaCTX-M-1 group, and 2 (8.3%) carried a blaCTX-M-2 group. Among the 18 K. pneumoniae isolates, 10 (55.6%) carried a blaCTX-M-2 group; 6 (33.3%) carried a blaCTX-M-1 group; and 2 (11.1%) carried a blaCTX-M-9 group. The blaCTX-M-8 and blaCTX-M-25 genes were not detected in any isolates. PCR products of the ceftazidime blaCTX-M-1 group (isolates with ceftazidime MIC ≥32 μg/ml), blaCTX-M-2 group (five randomly selected isolates), and blaCTX-M-9 group (two isolates) were sequenced. Sequencing results showed that seven isolates carried a blaCTX-M-15 gene; four isolates carried a blaCTX-M-1 gene; five isolates carried a blaCTX-M-2 gene; and two isolates carried a blaCTX-M-14 gene.
The CTX-M-1 group-producing isolates were the most widespread detected in the six health centers. The CTX-M-2 group-producing bacteria were isolated in four centers, and only two CTX-M-9 group-producing bacteria were isolated in the same center. The rate of ESBL isolates producing CTX-M-type enzymes was variable (range 22%–53%) (Fig. 1).
CTX-M producers were isolated from patients with a mean age of 54.8 years (range 7–84 years), and 21 patients were female. CTX-M-producing E. coli were mostly from urine (54.2%), followed by respiratory tract (8.3%), skin (8.3%), pus (8.3%), peritoneal fluid (8.3%), bile secretion (8.3%), and blood samples (4.2%). CTX-producing K. pneumoniae were recovered from urine (38.9%), respiratory tract (22.2%), skin (16.7%), pus (11.1%), peritoneal fluid (5.5%), and blood samples (4.2%).
Antimicrobial susceptibilities of CTX-M-producing isolates
The MIC50s (μg/ml) of ceftazidime, cefotaxime, cefepime, and aztreonam for CTX-M-producing E. coli were 12, >256, >32, and 16, respectively, and those for CTX-M-producing K. pneumoniae were 24, >256, >32, and 48, respectively. The isolates demonstrated consistently high MICs for cefotaxime and cefepime (except six isolates that showed FEP MIC ≤8), while MICs values of ceftazidime and aztreonam were variable among CTX-M producers. The ceftazidime MICs were higher than 32 μg/ml for 11 (7 were CTX-M-15-producing isolates) of 42 CTX-M-positive isolates.
The susceptibility data of the 42 CTX-M-producing isolates to noncephalosporin antibiotics are shown in Table 2. Susceptibility to amikacin was more common among CTX-M-producing E. coli (91.7%) than CTX-M-producing K. pneumoniae (38.9%). The isolates carrying the CTX-M-1 group showed lower rates of susceptibility against ciprofloxacin compared with the CTX-M-2 group. Up to 91.6% and 55.5% of CTX-M-producing E. coli and CTX-M-producing K. pneumoniae, respectively, were multiresistant to three or more antibiotic classes, and among these isolates was overall more frequent coresistance to ciprofloxacin, trimethoprim-sulfamethoxazole, and tetracycline (Table 2). Resistance to cefoxitin was noted in 25% and 33.3% of CTX-M-producing E.coli and K. pneumoniae, respectively.
Genotyping of the CTX-M-positive isolates
Genomic relatedness among the CTX-M-producing isolates was investigated by REP-PCR and ERIC-PCR profiling. Both profiles revealed the presence of multiple clusters among the CTX-M producers of either species; three of these clusters were within the same hospital from hospitalized patients (I, III, and VI clusters; Fig. 2). Isolates of the same cluster carried the same blaCTX-M variant, except for a cluster of K. pneumoniae (Fig. 2B). Among the 24 E. coli isolates, 14 (58.3%) clustered into four clonal groups of variable numbers of CTX-M-1-producing isolates. The major clonal group included seven isolates (II cluster; Fig. 2A) collected from four different hospitals isolated in hospitalized and nonhospitalized patients. Fifty-six percent of the K. pneumoniae isolates were not clonally related. The remaining isolates clustered into four small groups producing different CTX-M enzymes (Fig. 2B).
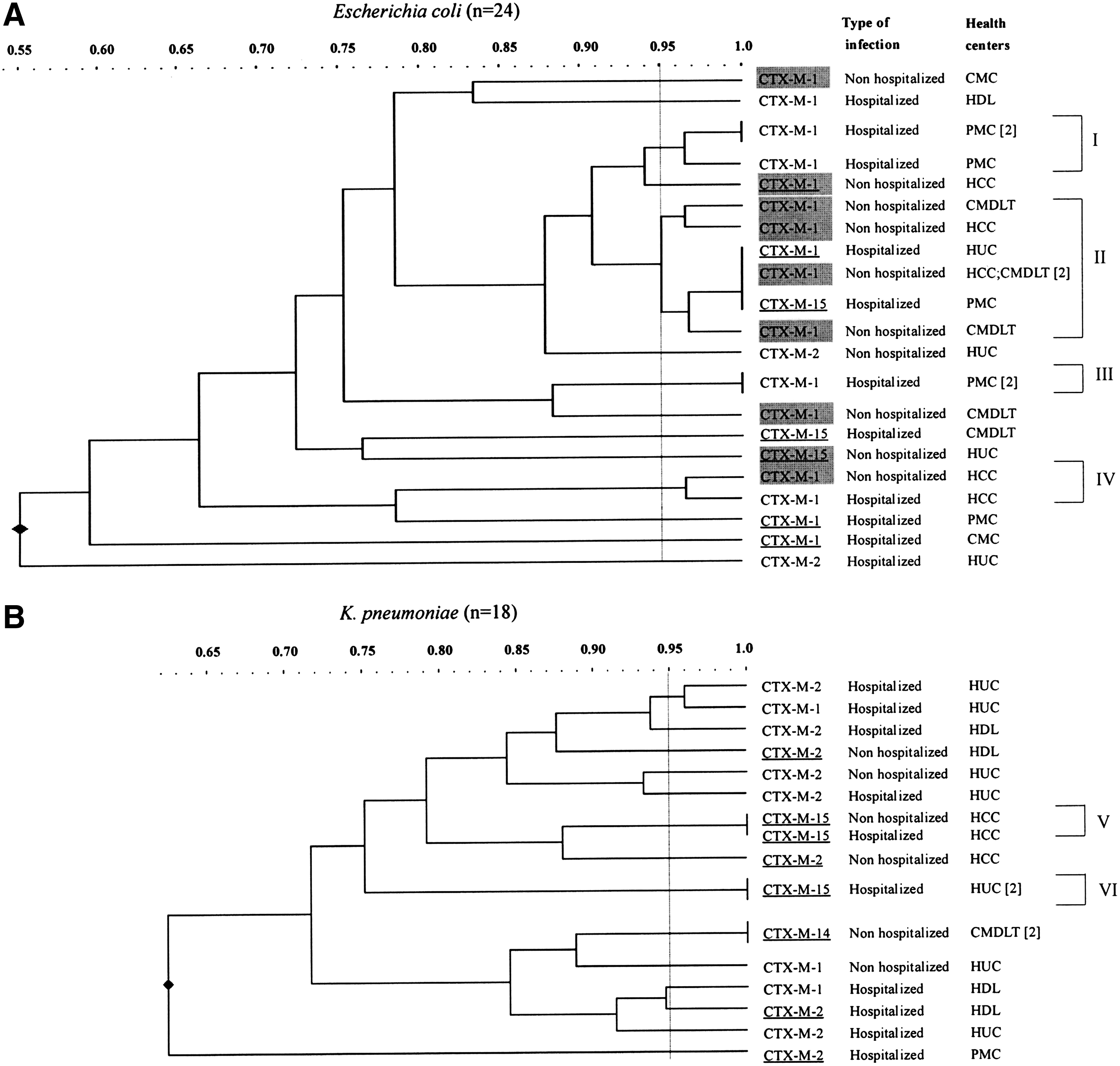
Dendograms based on repetitive extragenic palindromic-polymerase chain reaction typing showing genetic relatedness among CTX-M-producing Escherichia coli
Of interest, the total genotypic diversity was detected among isolates carrying the blaCTX-M-2 group (12 isolates distributed in 12 clusters; cluster/isolate ratio=1) unlike that observed among the isolates carrying the blaCTX-M-1 group (28 isolates distributed in 16 clusters; cluster/isolate ratio=0.57).
Discussion
This work provides insight into the molecular epidemiology of the CTX-M-producing E. coli and K. pneumoniae responsible of infections in Caracas. These isolates were detected in all participating centers distributed from east to west in hospitalized as well as nonhospitalized patients, demonstrating that CTX-M-type ESBLs have achieved a citywide distribution (Figs. 1 and 2). In a recent study, the prevalence of CTX-M among ESBLs-producing Enterobacteriaceae from hospitals in Caracas was ∼31%. 16 Data from the present study, showing a CTX-M prevalence of 43.3% among ESBL-producing E. coli and K. pneumoniae, could reflect a higher prevalence, and suggest that E. coli as well as K. pneumoniae have been important sources of CTX-M enzymes in Caracas. Continuing surveillance is mandatory to monitor the spread and evolution of this important ESBL-type in these pathogens.
The CTX-M-1 group was found in both species (mainly E. coli) and was the most frequent CTX-M-type (66.7%) among the ESBL-producing E. coli and K. pneumoniae isolated in Caracas. Likewise, in a neighboring country, Colombia, the CTX-M-1 group genes were detected in a high frequency among CTX-M-producing Enterobacteriaceae. 27 However, in Argentina, 22 Paraguay, 13 and Bolivia, 4 the CTX-M-2 group has been reported as the most frequent genotype, indicating that CTX-M-1 and CTX-M-2 groups are associated genotypes within this region of South America. In addition, CTX-M-14 and CTX-M-15 (first report in Venezuela) enzymes were detected in a low frequency in our study. These CTX -M variants have been reported as the dominant genotypes in European and Asian countries, and CTX-M-14 and -15 producers are recognized as important pathogens of nosocomial and community-acquired infections.3,10,11,15,20 Previously, in the South American continent, CTX-M-15 and CTX-M-14 have been only reported in Brazil, 5 Colombia, 25 Peru, and Bolivia. 17
In this study, more than one-third of CTX-M-producing isolates were from nonhospitalized patients (18 isolates), and 10 of them were the CTX-M-1 group-producing E. coli (10 isolates) from patients with urinary tract infections (Fig. 2A). Different authors have highlighted that these urinary isolates are capable of causing bloodstream-associated infections and could represent a reservoir for dissemination of infection within a healthcare institution.18,20,23
Carbapenems and tigecycline showed the most consistent activity against the CTX-M-producing isolates. Carbapenems have been considered the preferred therapy and tigecycline as an alternative for treatment of infections for these pathogens.11,18 In addition, E. coli isolates, mainly CTX-M-1 group producers (Table 2), retained susceptibility to amikacin, as previously reported.14,18 High rates of resistance were observed especially for ciprofloxacin and trimethoprim-sulfamethoxazole among CTX-M-producing isolates, which is consistent with other studies.14,18 The fraction of CTX-M-15-nonproducing isolates, which demonstrated high ceftazidime MICs, is likely to produce other ESBLs reported in Caracas, such as TEM or SHV. 26 Resistant to cefoxitin exhibited for CTX-M producers inferred the presence of AmpC beta-lactamases among these isolates. Recently, molecular detection of these cefalosporinases was reported in Caracas city. 16
Genotyping profiles may reveal differences in the spread of the blaCTX-M groups. In particular, genotypic diversity among isolates producing the CTX-M-2 group suggests that genetic support dissemination played a major role in the dissemination of the blaCTX-M-2 genes. In contrast, clusters I–VI-associated CTX-M-1 producer (Fig. 2) suggests that the dissemination of blaCTX-M-1 genes was dependent on clonal spread. These different behaviors may reflect the nature of the genetic elements carrying the two CTX-M group determinants. Further work is required to characterize the genomic location and which genetic mobile elements are implicated in the mobilization of these antibiotic resistance genes. Moreover, the cluster detected suggests that patient–patient transmission may have been a key factor in the wide dissemination and high prevalence of the CTX-M-1 group in Caracas.
Footnotes
Acknowledgments
This work was supported by a Grant from Consejo de Desarrollo Cientifico y Humanistico (CDCH) to G.A., PG-03-7327-2008. The authors thank Martin Llewellyn (Department of Pathogen Molecular Biology, London School of Hygiene & Tropical Medicine, London, United Kingdom) for writing assistance.
Disclosure Statement
No competing financial interests exist.