
Abstract
The ST8 methicillin-resistant Staphylococcus aureus (MRSA) with Staphylococcal cassette chromosome mec (SCCmec) type IVa, known as USA300, is a prevalent community-acquired MRSA (CA-MRSA) clone in the United States and has been spreading worldwide. The USA300 characteristically harbors Panton-Valentine Leukocidin (PVL) genes and the arginine catabolic mobile element (ACME, type I). Prevalence and molecular characteristics of PVL+ and/or ACME+ S. aureus were investigated in a university hospital located in northern Japan, for 1,366 S. aureus isolates, including 601 MRSA strains derived from clinical specimens collected from 2008 to 2010. The PVL gene was identified in three MRSA strains with SCCmec IV, which belonged to ST8, spa type t008, coagulase type III, and agr type I. Two PVL-positive MRSA strains had also type I ACME, and were isolated from skin abscess of outpatients who have not travelled abroad recently. One of these PVL+/ACME+ strains carried tet(K), msrA, and aph(3′)-IIIa, showing resistance to kanamycin, tetracycline, erythromycin, and ciprofloxacin, suggesting acquisition of more resistance than ST8 CA-MRSA reported in Japan previously. In contrast, another PVL+/ACME+ strain and a PVL+/ACME− strain were susceptible to more antimicrobials and had less virulence factors than PVL−/ACME+ MRSA strains. Besides the two PVL+ MRSA strains, ACME (type-ΔII) was identified into seven MRSA strains with SCCmec II belonging to ST5, one of the three spa types (t002, t067, and t071), coagulase type II, and agr type II. These PVL−/ACME+ MRSA strains showed multiple drug resistance and harbored various toxin genes as observed for ST5 PVL−/ACME− MRSA-II. The present study suggested the spread of ST8-MRSA-IV in northern Japan, and a potential significance of ACME-positive ST5-MRSA-II as an emerging MRSA clone in a hospital.
Introduction
Staphylococcal cassette chromosome mec (SCCmec), a genetic element containing mecA that is critical to methicillin resistance in MRSA, is diverse in their structural organization and genetic content, and has been classified into several types and subtypes. 20 Three types of SCCmec elements (type I, II, and III) are carried mostly by hospital-acquired MRSA (HA-MRSA) strains. 36 By contrast, the majority of CA-MRSA strains differ from HA-MRSA strains in that they usually contain SCCmec type IV or V,19,36 although several HA-MRSA clones (e.g., EMRSA-15) also carries SCCmec IV. Most of the CA-MRSA strains that have emerged in recent years produce PVL, associated with occurrence of severe symptoms in wide spectrum of infections. 2
Globally, MRSA clones with different genetic traits predominate in different geographical locations. ST8-MRSA-IVa, known as CA-MRSA clone USA300, has become predominant CA-MRSA clone in the Unites States,18,33 and has spread to Europe, South America, Australia, and Japan, although its prevalence outside the U.S. is still generally low.28,32 The USA300 clone characteristically harbors arginine catabolic mobile element (ACME) linked to SCCmec type IVa in its chromosome, 7 which is associated with enhanced ability of growth and survival, and considered as a key factor in the persistence of USA300 in the community.8,36 Coagulase-negative staphylococci, such as S. epidermidis, is considered to act as a reservoir of ACME for S. aureus.24,30 ACME is integrated into the orfX, the attachment site for the SCCmec element, and it was demonstrated that ACME integration and excision is catalyzed by the SCCmec recombinase.8,10
In Japan, most of the MRSA from inpatients and outpatients have been reported to be the New York/Japan clone belonging to ST5, and the predominant CA-MRSA clones were PVL-negative ST5 strains.15,36 From sporadic cases, ST8-USA300 clone has been reported in only three cases since 2007: (1) a 3-month-old Indian girl who was born in United States of America, (2) a 25-year-old American woman, and (3) a 11-month-old Japanese girl.11,13,28 Among these, CA-MRSA infection in the case (3) is considered as the first report suggesting transmission of USA300 clone in Japan, from her family members who visited Hawaii.13,35 These cases occurred in areas near Tokyo. In addition, there have been two reports on outbreak of skin infections due to USA300 clone in hospitals in Kyoto, in western Japan, 26 and Okinawa, a southernmost main island of Japan. 23 However, information of ST8 MRSA clones in Japan, that is, their prevalence and genetic characteristics, is still limited, and no information is available about the epidemiology of USA300 clone in northern Japan. In the present study, prevalence and genetic traits of PVL and/or ACME-positive S. aureus were analyzed for recent clinical isolates from a large teaching hospital in Hokkaido, a northern main island.
Materials and Methods
Bacterial isolates and susceptibility testing
A total of 1,366 S. aureus isolates were analyzed. These bacterial strains were derived from clinical specimens associated with a single patient who developed symptom of infection, in Sapporo Medical University Hospital located in Sapporo, in Hokkaido, Japan, between February 2008 and December 2010. All the isolates analyzed in the present study were regarded as hospital-associated pathogens. Antimicrobial susceptibility testing was performed for representative 24 strains that included all the 11 PVL+ and/or ACME+ strains, and 13 PVL−/ACME− MRSA strains belonging to different SCCmec types (SCCmec IIa, three strains; SCCmec IV, seven strains; SCCmec V, three strains). Minimum inhibitory concentrations of representative 12 antimicrobial agents (oxacillin, ampicillin, cefoxitin, vancomycin, gentamycin, kanamycin, fosfomycin, tetracycline, minocycline, ciprofloxacin, clindamycin, and erythromycin) were measured by broth microdilution test and interpreted as sensitive or resistant based on the National Clinical and Laboratory Standards Institute guidelines. 5
Multiplex PCR assays for MRSA, genotyping
For all the S. aureus isolates, the presence of staphylococcal 16s rRNA gene, nuc, mecA, PVL gene (lukS-PV/lukF-PV), and ACME gene (arginine deminase gene: arcA) was investigated by multiplex PCR assay as described by Zhang et al. 37 Coagulase genotypes, including subtypes of IV and V, and accessory gene regulator (agr) typing were determined by multiplex PCR assay as described previously.14,15 SCCmec type and SCCmec subtype of MRSA were determined by PCR as described previously.20,22 For the selected 24 strains described above, sequence type (ST) defined by multilocus sequence typing scheme was determined as described previously. 9 Based on sequence of X-region of protein A gene, spa type was determined by PCR and sequencing for the 24 strains as described previously, 29 using a public spa type data base (http://tools.egenomics.com/or http://spaserver.ridom.de/).
Detection of virulence factors and drug resistance genes
For the above-mentioned 24 representative strains, prevalence of genes encoding various toxins (sea, seb, sec, sed, see, seg, seh, sei, sej, selk, sell, selm, seln, selo, selp, selq, ser, ses, set, selu, eta, etb, etd, hla, hlb, hlg, hlg-v, hld, lukM, tsst-1) and virulence factors (cna, fnbA, ebpS, bbp, sdrC, edin-A, edin-B), and antimicrobial resistance genes was analyzed by multiplex or monoplex PCR, by using primers described previously.1,15,30
ACME typing, sequencing analysis of ACME-arcA, and sarU promoter
ACME types I, II, ΔII were classified by long-range PCR (LR-PCR), in terms of orientation and size of the ACME-arcA locus (LR-PCR 1), the region between ACME-arc and ACME-opp3 (LR-PCR 2), and the region between ACME-opp3 and the copA junction (PCR 3). LR-PCR 1 and LR-PCR 2 were performed as previously described. 3 The PCR 3 primers copA-F1 (5′-GTTACAGCTGTGGGAGAAGATGG-3′) and copA-R1 (5′-CATGCCAATGACTTGTTGATCCTC-3′), which amplify copA gene, were designed in the present study. Genetic diversity of ACME-arcA gene and sarU promoter located between sarU and sarT in S. aureus strains was analyzed, comparing the nucleotide sequence obtained with those of USA300 clones. Nucleotide sequences of these genetic targets were determined by PCR and direct sequencing. A DNA fragment containing full-length open reading frame (ORF) of ACME-arcA was amplified by PCR with primers arcA-F (5′-GAGCCAGAAGTACGCGAG-3′) and arcA-R (5′-CACGTAACTTGCTAGAACGAG-3′). Highlander et al. 12 revealed a number of single nucleotide polymorphisms (SNPs) within ORF or intergenic regions in different USA300 clones, and sarU promoter is described as one of the intergenic regions where sequence diversity was detected. In the present study, the sarU promoter genotyping was attempted to analyze relatedness of isolated MRSA strains (all the 11 PVL+ and/or ACME+ strains, and 10 PVL−/ACME− strains of which the STs were determined) to the USA300 clones. Intergenic region containing sarU promoter was amplified by PCR with primers SarT1 (5′-ATTTACGCAGCTCATATGTAG-3′) and SarU1 (5′-TTTAGTGAAATACTGTGTTC-3′). Multiple sequence alignment was performed by ClustalW program.
Results
Genetic background, PVL, ACME in S. aureus strains
Among the 1,366 S. aureus isolates analyzed this study, 601 isolates (44.0%) were judged as MRSA (mecA-positive). Most of MRSA belonged to coagulase genotype IIa, while methicillin-susceptible S. aureus (MSSA) were classified into various types (Table 1). The PVL gene was identified in three MRSA strains (0.5% in MRSA), while the ACME gene (arcA) was detected in nine strains: eight MRSA strains (1.3% in MRSA) including the two strains with PVL gene, and one MSSA strain (Table 1).
Number of PVL−/ACME+ isolates.
Two PVL+/ACME+ isolates and a PVL+/ACME− isolate.
Number of PVL−/ACME+ isolate.
PVL, Panton-Valentine Leukocidin; ACME, arginine catabolic mobile element; SCCmec, Staphylococcal cassette chromosome mec; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible S. aureus.
Three PVL+ MRSA strains belonged to ST8, spa type t008, coagulase genotype III, and agr-type I. The two PVL+/ACME+ strains (SA1483, SA2269) had type IVa SCCmec, while a PVL+/ACME− strain (SA1725) had SCCmec IVc (Table 2). All the PVL−/ACME+ MRSA strains, possessing SCCmec-II, belonged to ST5, one of the three spa types (t002, t067, and t071), coagulase type II, and agr-type II. One ACME+ MSSA strain was classified into ST81 (CC15), coagulase type VII, and agr-type III. Representative PVL−/ACME− MRSA strains with different SCCmec types and coagulase types were selected and analyzed for their genetic characteristics (Table 2). Among these strains showing various agr types, STs, two SCCmec IV strains belonged to ST8, coagulase type III, and agr-type I, which are identical to those of PVL+ strains. In summary, clonal types (ST-MRSA-spa-SCCmec) of PVL+ MRSA strains and PVL−/ACME+ MRSA strains were represented as ST8-MRSA-t008-IV and ST5-MRSA-t002-II, respectively.
ACME type: I, arcA+/opp3AB+/copA+; Δ II, arcA+/opp3AB−/copA−.
OXA, oxacillin; AMP, ampicillin; CFX, cefoxitin; GM, gentamycin; KM, kanamycin; FOM, fosfomycin; TET, tetracycline; MINO, minocycline; CIP, ciprofloxacin; CLI, clindamycin; ERY, erythromycin. None of the strain showed resistance to vancomycin. Three PVL+ strains showed lower MICs to oxacillin (64–128 μg/ml) than PVL−/ACME+ MRSA strains (512 μg/ml).
The following genes, which were undetectable in any strains, were omitted in this Table; aac(6′)-li, aac(6′)-lm, ant(3′′)-la, ant(9)-lb, aph(2′′)-lb, aph(2′′)-lc, aph(2′′)-ld, eta, etb, etd, mupA, lukM, and cfr.
The following genes, which were detected in all strains, were omitted in this Table; lukE-lukD, hla, hlb, hlg, hlg-v, and hld.
Not assigned (singleton).
Although the SCCmec type was assigned to IIa, ccrC was also detected in these strains.
Subtype could not be determined.
ebps gene with internal deletion as reported previously1 was detected.
ST, sequence type.
Clinical information of PVL+ and/or ACME+ strains
The two PVL+/ACME+ strains, SA1483 and SA2269, were isolated from skin abscesses in leg (popliteal fossa) of a 37-year-old man and in neck of a 78-year-old woman, respectively. These cases visited the dermatology department in the hospital on different dates, July 2009 (SA1483) and September 2010 (SA2269), respectively. They had no history of overseas travel within at least 2 years. PVL+/ACME− strain SA1725 was isolated from pharyngeal swab of a 51-year-old male patient admitted to the department of internal medicine. The seven PVL−/ACME+ MRSA strains were derived from various specimens, including sputum (3), urine (1), feces (1), drainage (1), and ear exudate (1) of inpatients from three clinical departments.
Antimicrobial susceptibility and virulence factors
The PVL+ MRSA strains, despite showing resistance to beta-lactams, had lower number of drug resistance genes and enterotoxin genes than PVL−/ACME+ MRSA (Table 2). Two PVL+ MRSA strains, SA1725 and SA2269, had no resistance genes to tetracycline, aminoglycoside, and macrolide, showing susceptibility to tetracycline, gentamicin, kanamycin, clindamycin, and erythromycin. However, PVL+/ACME+ strain SA1483 harbored tet(K), msrA and aph(2′′)-IIIa, and was resistant to tetracycline, erythromycin, and kanamycin. Only selk and selq, or no enterotoxin gene were detected in the three ST8 PVL+/ACME+ MRSA strains. In contrast, all the PVL−/ACME+ MRSA had the enterotoxin gene cluster (seg, sei, selm, seln, selo, selu), and sec and tsst-1, and resistance genes ermA, ermB, and ant(9)-Ia, exhibiting resistance to macrolides, fosfomycin, ciprofloxacin, and high-level resistance to gentamicin (except for strain SA1885). Similarly, PVL−/ACME− MRSA strains harbored various drug-resistance genes and enterotoxin genes (except for strain SA2268) (Table 2).
ACME types and sarU promoter sequence typing
By LA-PCR assay, the two PVL+/ACME+ ST8 MRSA strains SA1483 and SA2269 were found to have the type I ACME, which is typically present in the USA300 clone. 31 The ACME+ ST5-SCCmec IIa MRSA strains had type ΔII ACME which is integrated between SCCmec and orfX. ACME-arcA gene sequences of the two ST8 PVL+/ACME+ MRSA strains were identical to that of the USA300-FPR3757 strain. In contrast, between the USA300 clone and seven PVL−/ACME+ ST5 MRSA strains, two-nucleotide difference in ACME-arcA was detected (data not shown).
By comparison of whole genomes of two USA300 strains, numerous subtle genetic differences, including SNPs in ORFs and intergenic sequences, were revealed, 12 although these USA300 clones were genetically similar. The sarU promoter sequence was described as one of such divergent regions and discriminate TCH1516 (USA300-HOU-MR) from USA300-FPR3757 by a four base deletion. Therefore, sequence analysis of this region for the MRSA strains may provide information of genetic relatedness to those USA300 clones. Among the MRSA strains analyzed in the present study, ST8 MRSA including PVL+/ACME+ strains SA1483 and SA2269, exhibited the most similar sarU promoter sequences to that of USA300-FPR3757, while two-nucleotide deletion near the SarA binding motif was identified (Fig. 1). At the same site, six-nucleotide deletion was found in all other MRSA strains including ACME+ ST5 strains.
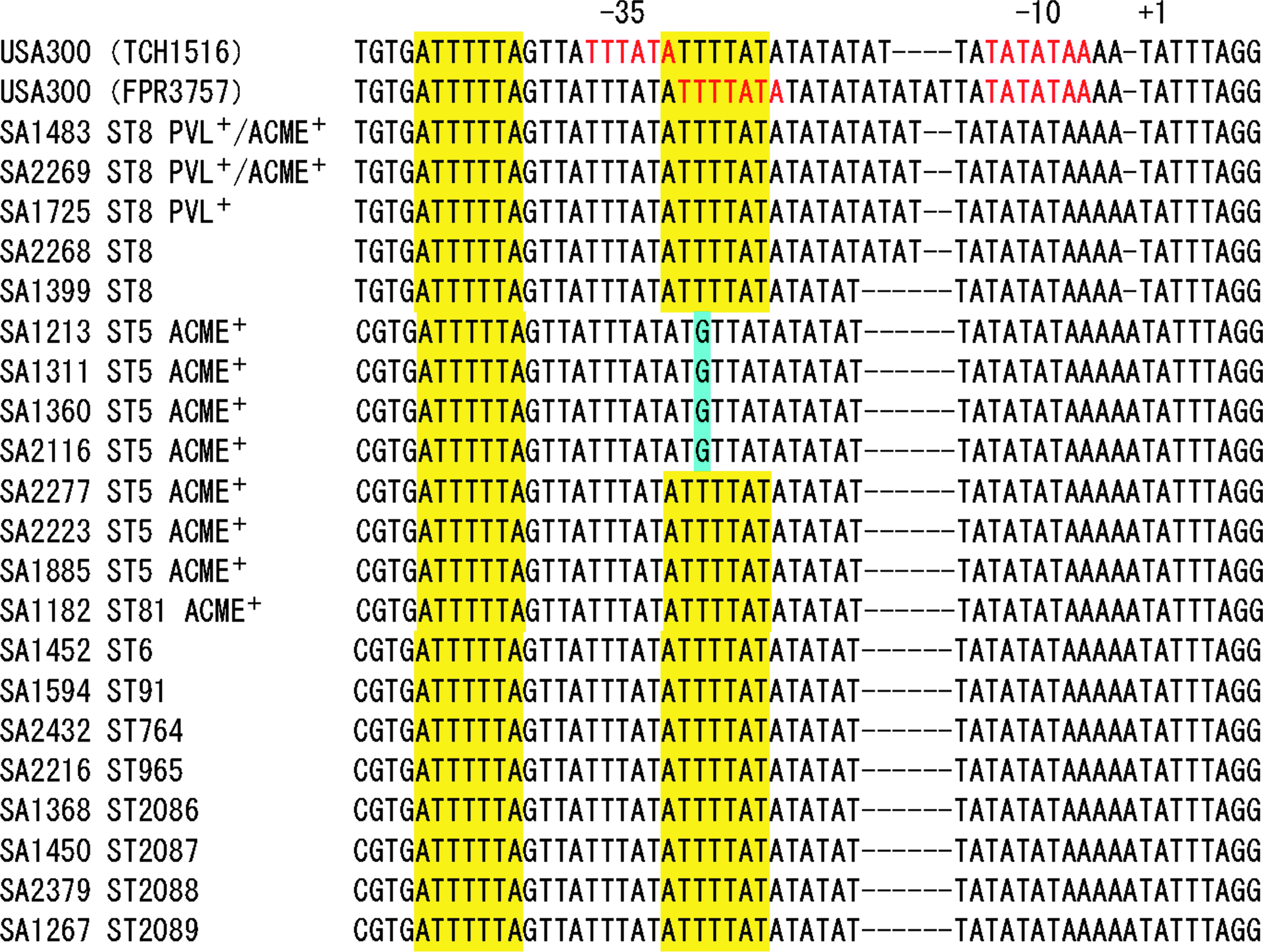
Comparison of nucleotide sequences of sarU promoter region of USA300 strains (FPR3757 and TCH1516) and PVL+/− and/or ACME+/− MRSA/MSSA strains analyzed in this study. sarU promoter region −10 and −35 sequences of USA300 strains are indicated in red letters (−35 is shown for the sequence of TCH1516). Putative SarA consensus binding sites are shown in yellow. A substituted nucleotide in this site is indicated by blue. Dash denotes gap. PVL, Panton-Valentine Leukocidin; ACME, arginine catabolic mobile element; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible S. aureus.
Discussion
The USA300 clone, that is, ST8-MRSA-IVa, has become the prevalent CA-MRSA strain in the United States since the first report in 2000 as a cause of skin and soft tissue infections, and is recognized also as an emerging nosocomial MRSA. 32 Analysis of the complete genome sequence revealed that the USA300 (strain FPR3757) possesses PVL gene and ACME. 7 It was indicated that USA300 clone has undergone rapid clonal expansion, 16 associated with continuous evolution and acquisition of drug resistance genes and virulence factors.4,17
In the present study, two ST8-t008-MRSA strains with SCCmec type IVa harboring PVL gene and ACME were identified among the 601 hospital isolates of MRSA collected for about 3 years. These strains belonged to agr type I and possessed type I ACME, and selk and selq, which are the same traits as the USA300 clone, and also had identical ACME-arcA sequence to that of USA300-FPR3757 strain. Particularly, strain SA1483 carried tet(K), msrA, and aph(3′)-IIIa, and showed resistance to oxacilllin, kanamycin, tetracycline, erythromycin, and ciprofloxacin. Presence of tet(K) is the same characteristics as USA300-FPR3757 strain, while msrA and aph(3′)-IIIa as USA300-TCH1516 strain. 30 USA300-0114 isolates are typically resistant to erythromycin due to msrA and variably resistant to tetracycline mediated by tet(K).17,33 However, erm(C) and mupA that are present in FPR3757 were not detected in SA1483. ST8-MRSA-IV strain SA2269 did not harbor tet(K) and msrA, and another strain SA1725 has SCCmec type IVc and lacked ACME. These observations indicated that among the three ST8-MRSA-IV strains detected in the present study, SA1483 may be the most closely related to the USA300 strains reported in the United States. Presence of evident genetic diversity among the only three PVL-positive ST8-MRSA-IV strains with spa type t008 isolated in the present study suggests that this clone may readily vary in its drug resistance and virulence during transmission, as revealed for CA-MRSA isolates in Europe. 27
In Japan, two ST8-MRSA-IVa strains NN36 (spa type t008) and NN47 (spa type t024) derived from sporadic cases have been well characterized.13,28 NN47 was isolated from a Japanese girl and described as the first USA300 transmitted among people in Japan, while NN36 was derived from an Indian girl who moved from the United States. These strains belonged to agr type I and coagulase type III, and possessed the PVL gene and ACME, and msrA and aph(3′)-IIIa, as observed for SA1483 strain in our present study. However, the NN36 and NN47 strains lacked tet(K) and susceptible to tetracycline and ciprofloxacin, unlike the strain SA1483. Although ST8-MRSA-IVa (spa type t008) strains were reported as causative agents of a hospital outbreak in Okinawa island, these were not resistant to minocycline. 23 Therefore, compared with the ST8-MRSA-IV strains reported in Japan so far, strain SA1483 isolated in the present study may be more closely related to the USA300-0114 and considered as the first ST8 CA-MRSA having tet(K) in Japan, which has acquired resistance to more antimicrobials than those reported previously. Spa type of the NN47 strain, t024, is genetically close to the spa type t008 that was typically observed in USA300-0114, a type strain of USA300, 37 because t024 (11-12-21-17-34-24-34-22-25), except for lacking of a single repeat unit, has the same arrangement of nine different repeat units in the X-region of the spa gene as t008 (11-19-12-21-17-34-24-34-22-25). Therefore, strain NN47 is suggested to be evolved from USA300 clone through transmission. In contrast, strain SA1483 appears to be a direct derivative from the USA300 clone because of having the same spa type (t008) as USA300 clone, as well as drug resistance traits as described above, thus may not be originated from the Japanese strain NN47.
The ACME is one of the most distinguishing features of the USA300 clone and was found to be important for its growth and survival, improving fitness and ability to colonize skin and mucous membrane.7,8 Three ACME allotypes have been described for staphylococci, that is, type I (arcA+/opp3AB+), type II (arcA+/opp3AB−), and type III (arcA−/opp3AB+). While type I ACME is characteristically harbored by ST8-MRSA-IV (USA300 clone), type ΔII, a variant of type II which lacks copA gene, has been identified in ST22-MRSA-IVh. 31 Although only limited reports are available, ACME-arcA has been detected in some subsets of S. aureus clones; ST8-MRSA-IVa at high frequency (almost 100%), and ST5-MRSA-II and ST22-MRSA-IVa/IVh at low frequency, and a few ST8-MSSA in the United States.10,31 ACME+ CC5-MRSA-II strains were also isolated in Hong Kong and Western Australia, despite a few isolates.6,25 Similarly to these reports, in our present study, ACME was detected in ST8 and ST5 MRSA strains, and only one MSSA belonging to ST81. While ST8-MRSA had type I ACME, it was of note that type ΔII was detected in all the seven ST5-MRSA-II and ST81-MSSA, indicating that origin of ACME for ST8 MRSA should have been different from those of ST5 and ST81 strains. It has been revealed that the type ΔII ACME in ST22-MRSA-IVh corresponds to a portion of type II ACME identified in S. epidermidis, suggesting occurrence of horizontal transfer of ACME from coagulase-negative staphylococci. 31 The ST5-MRSA with SCCmec II (coagulase type IIa) is known as New York/Japan clone, a most prevalent HA-MRSA in Japan, 36 as observed in the present study (∼90%). Therefore, acquisition of ACME by ST5-MRSA-II may facilitate persistence and dissemination of this MRSA in health care settings, which will be one of the concerns for infection control.
In our previous study of CA-MRSA in Hokkaido, Japan, ACME-arcA was detected in two ST5-MRSA strains (SCCmec type II and V) among 189 MRSA strains analyzed, 15 and thereafter the ACME of these strains were assigned to type ΔII. 34 Considering the extremely low frequency of ACME in ST5-MRSA-II, detection of seven ST5-MRSA-II strains with ACME from various specimens and departments in the present study may suggest dissemination of this MRSA strain in a hospital. Spa types of these strains, t002, t067, and t071, are genetically similar because deletion or addition of single repeat unit in X-region of t002-spa is found in t067- and t071-spa, respectively, implying occurrence of genetic evolution in the ST5-MRSA during their transmission among humans. These findings indicate a potential significance of ACME-positive ST5-MRSA-II as an emerging MRSA clone in a hospital, and thus continuous surveillance of ST5-MRSA may be necessary, particularly in terms of prevalence of ACME.
S. aureus regulatory element sarU, a sarA homologue, is reported as a positive activator of agr which up-regulates expression of many cell wall proteins and some exoproteins. 21 In the sarU promoter region containing sarA-binding motif, four nucleotide-deletion was described in USA300-TCH1516 strain as compared with that of USA300-FPR3757 strain. 12 In the present study, a two-nucleotide deletion was found in four strains among the five ST8-MRSA, while a six-nucleotide deletion was detected in all other strains including ST5-MRSA with ACME. This finding suggests that this region of FPR3757 was closer to that of most ST8-MRSA strains than MRSA and MSSA strains with other STs isolated in the present study. Although evidence has yet to be reported, the possibility that such subtle nucleotide difference could affect transcription of sarU is raised. 12 Presence of genetic diversity in the sarU promoter region among ST8-MRSA in the United States and Japan suggests that continuous evolution has been occurring in this clone, possibly associated with alteration of its virulence.
In conclusion, PVL+/ACME+ ST8-MRSA-IVa strains were first identified in a hospital in northern Japan, from patients who have not made overseas trip recently, suggesting a potential spread of this type of MRSA in health-care settings in Japan. One of these strains possessed tet(K), msrA, and aph(3′)-IIIa, and showed resistance to more antimicrobials than ST8-MRSA-IVa reported in Japan previously, suggesting acquisition of drug resistance during transmission among humans. ACME was detected in seven ST5-MRSA-II strains, the predominant HA-MRSA known as New York/Japan clone. Although detection of these strains is still rare in Japan, further surveillance is needed for their prevalence in hospitals and community.
Footnotes
Acknowledgments
This study was supported in part by a Grant-in-Aid for Scientific Research (No. 23590746) from the Ministry of Education, Culture, Sports, Science, and Technology, Japan.
Disclosure Statement
The authors of this article have no commercial associations that might create a conflict of interest in connection with the submitted manuscript.