
Abstract
The objectives of this study were to evaluate the clinical effectiveness of gentamicin as an initial empirical antimicrobial agent and to determine the effects of gentamicin resistance on clinical outcomes in women with uncomplicated acute pyelonephritis (APN). We analyzed data of 2,033 women with a diagnosis of APN admitted to Catholic University St. Vincent's Hospital. Of those, we enrolled 274 cases of community-acquired uncomplicated APN due to Escherichia coli who received gentamicin as initial antibiotics. Of these 274 patients, 47 patients had gentamicin-resistant (GM-R) E. coli APN, and 227 patients had gentamicin-susceptible (GM-S) E. coli APN. The early clinical response rates were 55.3% (26/47) versus 81.5% (185/227) at 72 hours; 61.7% (29/47) versus 96.9% (220/227) at 96 hours in the GM-R and GM-S groups, which was significantly higher in the GM-S group (p<0.001). Overall clinical cure rates were 100% (47/47) and 99.6% (226/227) in the GM-R and GM-S groups, respectively. APN patients in the GM-R group had longer hospitalization (9.72±3.46 and 7.89±2.27 days; p<0.001) than those in the GM-S group. Resistance of E. coli to gentamicin, bacteremia, and C-reactive protein level showed independent effects on early clinical failure. Aminoglycoside such as gentamicin can be an alternative antibiotic option for initial empirical therapy of community-acquired uncomplicated APN as the fluoroquinolone-sparing or broad-spectrum cephalosporin-sparing agents in an era of increasing antimicrobial resistance, especially in areas where medical resources are limited or antibiotic resistance rate of the uropathogens is high.
Introduction
Acute pyelonephritis (APN) patients who exhibit systemic symptoms or signs such as high fever, flank pain, nausea, vomiting, and leukocytosis may need hospitalization and the use of intravenous antimicrobial agents, such as an extended-spectrum cephalosporin, a fluoroquinolone, or an aminoglycoside. Current clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis as updated by the Infectious Diseases Society of America recommend that fluoroquinolones be reserved as an alternative only when other antimicrobials for UTIs cannot be used, for the prevention of the spread of fluoroquinolone resistance, among other clinically significant pathogens as well as among uropathogens.5,6 Aminoglycosides, which are not significantly associated with ESBL resistance compared with extended-spectrum cephalosporin, can be a good cephalosporin-sparing agent, if the clinical effectiveness of aminoglycoside monotherapy is proved.
Gentamicin exerts a bactericidal effect by binding irreversibly to the 30S subunit of the bacterial ribosome and interfering with reading of the genetic code, thus inhibiting the synthesis of protein. Plasmid-mediated aminoglycoside-modifying enzymes, including three acetyltransferases, four adenyltransferases, and five phosphotransferases, are known to be the most important of the mechanisms of aminoglycoside resistance. It is known that gentamicin is susceptible to at least these five enzymes, and amikacin is modified by only one of these enzymes. Therefore, amikacin can be considered to be the aminoglycoside active against gentamicin-resistant (GM-R) Enterobacteriaceae.4,26
Though it has been recognized by clinicians that aminoglycosides such as gentamicin or amikacin are effective in the treatment of APN,22,25,27 a few clinical studies have been focusing on the use of gentamicin as initial empiric antibiotic therapy of APN patients during the last 10 years. It is important to understand the therapeutic efficacy and safety of gentamicin in the treatment of APN, considering its low cost, its postantibiotic effect, and its concentration-dependent bactericidal action.1,11
Gentamicin was administered as an initial empirical antimicrobial agent in hospitalized uncomplicated APN patients with normal renal function from March 2000 to February 2010, according to Catholic University St. Vincent's Hospital Antibiotic Policy. The purpose of these antibiotic policies is to use low-priced antibiotics having a narrow spectrum of antibacterial activity, and to spare expensive broad-spectrum antibiotics, such as a fluoroquinolone, or extended-spectrum cephalosporin, in managing UTIs.
In Korea, one study showed that the resistance rates of Escherichia coli isolates to gentamicin in uncomplicated APN were 15.3% and 19.3% in 2001–2002 and 2008–2009, 12 respectively, and another showed that the resistance rates of E. coli to gentamicin in acute uncomplicated cystitis were 18.3% and 22.4% in 2002 and 2006, respectively. 10
We investigated clinical and microbiologic data of 274 women with community-acquired uncomplicated APN who were admitted to one university hospital in Korea to evaluate the clinical effectiveness of gentamicin as an initial empirical antimicrobial agent and to determine the effect of gentamicin resistance on clinical outcome in women with uncomplicated APN.
Materials and Methods
Study design
This was a retrospective study of community-acquired uncomplicated APN patients performed at Catholic University St. Vincent's Hospital, a 791-bed secondary teaching hospital in Suwon City, in South Korea. We analyzed data of all APN patients admitted to St. Vincent's Hospital from March 2000 to February 2010. The Institutional Review Board (IRB) of the Catholic University St. Vincent's Hospital, Suwon, South Korea, reviewed and approved all protocols to conduct the APN study titled “Retrospective clinical study to evaluate clinical and microbiological efficacies of empirical use of gentamicin for community-acquired uncomplicated APN caused by E. coli in women” (approval number VC12RISI0074). The IRB waived the requirement for the investigator to obtain a written, informed consent from each patient in this study.
Patient population
On 2,033 women with APN as a discharge diagnosis in the hospital discharge database from March 2000 to February 2010, we retrospectively evaluated clinical symptoms, medical history, etiologic microorganisms, antibiotic susceptibilities, and treatment regimens by reviewing their medical records. APN was defined by fever ≥38.0°C, and the presence of at least three of the following: pain in the upper urinary tract (pain in the flanks or pain in the back), costovertebral angle tenderness on examinations, symptoms in the lower urinary tract (dysuria, urgency, frequency, and pain in the vesical region), pyuria on microscopic examination of the urine (≥5–9 leukocytes/high-power field), and leukocytosis (peripheral white blood cell count greater than 11,600/mm3 or polymorphonuclear cells plus bands greater than 65%).15,21 Individuals without upper urinary tract symptoms and signs were enrolled only if radiologic findings of APN were demonstrated by computerized tomography, and the discharge diagnosis of APN was made under the supervision of the infectious disease specialist. Any patient who was diagnosed as APN 48 hours after admission or as urinary catheter-related infection or complicated APN was excluded from the study. Complicated APN was defined as APN combined with any systemic underlying disorder (diabetes mellitus, kidney transplantation, renal disease, liver disease, cerebrovascular disease, malignancy, pregnancy, and immunosuppression), urinary tract abnormalities (urolithiasis, ureter stricture, urologic surgery, urologic malignancy, polycystic kidney disease, vesicoureteral reflux, and neurogenic bladder), or age more than 65 years old. 12 Only urine culture-proven cases of community-acquired APN due to E. coli in the women aged ≥18 years were finally included and analyzed.
Data collection
Data on demographic characteristics, urinary symptoms and relevant physical findings, previous history of hospitalization, history of previous UTIs, antibiotic usage within previous 1 year before admitting to hospital, treatment regimens, laboratory results, microbiological data, days to defervescence, and days of hospital stay were collected for all eligible patients, based on a retrospective review of medical records.
Clinical outcome measures
Early clinical response at 72 or 96 hours was defined as resolution of fever with improvement of urinary tract symptoms or signs within 72 or 96 hours after the start of empirical antimicrobial therapy. Clinical cure was defined as absence of symptoms or signs at completion of therapy and/or at 4–10 day follow-up, when available.20,23 “Resolution of fever” was defined as an afebrile state where the body temperature (tympanic) remains at 37.0°C or below 37.0°C for 24 hours or longer after the body temperature returns to 37.0°C or below. “Time to defervescence” was assessed as the time from the start of empirical antimicrobial therapy to the afebrile state. We analyzed the data of the tympanic temperatures of each patient measured every 6 hours during hospitalization.
Acute kidney injury was defined as an absolute serum creatinine increase >0.3 mg/dl or a relative increase in serum creatinine >50%, in accordance with the Acute Kidney Injury Network criteria. 14
Microbiological data
Blood and urine cultures were processed, and etiologic agents were determined when ≥105 CFU/ml of organisms were identified on urine culture, and/or isolation of urinary pathogens from blood culture.24,29 Species identification and susceptibilities to antimicrobial agents were determined by means of either a semiautomated system (Microscan, DADE Behring, West Sacramento, CA) or disk diffusion susceptibility tests according to the criteria of the Clinical and Laboratory Standard Institute (CLSI). 3 The minimum inhibitory concentration cutoff for gentamicin resistance was ≥8 mg/L.
Statistical methods
SPSS version 21.0 for Windows (SPSS, Inc., Chicago, IL) was used for statistical analysis. Categorical variables were analyzed by chi-square test or Fisher's exact test. Continuous variables were analyzed by independent t-test or Mann–Whitney test. Logistic regression analysis was performed to evaluate the effects of independent variables on clinical outcome. Results below a 5% significance level were considered statistically significant. A multivariate analysis was performed using logistic regression to evaluate the effects of independent variable on early clinical failure in the uncomplicated APN patients who were treated by gentamicin.
Results
Demographic and clinical characteristics
During the study period, a total of 2,033 patients with a diagnosis of community-acquired APN were screened. Of these patients, 1,128 cases received gentamicin, and 905 cases of other antibiotics as initial antimicrobial agents. Of the 1,128 patients treated by gentamicin initially, 561 cases gave positive urine and/or blood culture for E. coli, and 28 cases for non-E. coli such as 10 Klebsiella pneumoniae, three Proteus mirabilis, three Enterobacter aerogenes, two Staphylococcus saprophyticus, two Citrobacter koseri, one Citrobacter freundii, one Enterobacter cloacae, one Streptococcus agalactiae, one Staphylococcus aureus, one Klebsiella ozanae, one Pseudomonas aeruginosa, one Enterococcus faecalis, and one Enterococcus faecium. Among these 561 cases, 287 cases were excluded because of underlying systemic or urologic abnormalities that defined them as having complicated pyelonephritis. Finally, 274 cases of community-acquired uncomplicated APN due to E. coli who received gentamicin as initial antibiotics were enrolled and analyzed.
Of 274 patients, who were treated initially with gentamicin and were found to have E. coli as the cause of uncomplicated APN, 47 patients had GM-R E. coli APN, and 227 patients had gentamicin-susceptible (GM-S) E. coli APN. Table 1 shows the demographic data and clinical characteristics of the GM-R and GM-S groups. There were no significant differences in age, the prevalence of menopause, initial leukocytes counts, initial C-reactive protein (CRP) levels, initial body temperature, previous history of UTI, previous history of hospitalization, fever duration before hospital visit, and presence of bacteremia. The frequencies of antibiotic usage within 12 months before hospital visit in the GM-R and GM-S groups were 25.5% (12/47) and 11.0% (25/227), which was significantly higher in the GM-R group (p=0.008) (Table 1).
Data are shown as numbers of patients (% of total) or mean±standard deviation as appropriate.
By Mann–Whitney U test.
By Pearson chi-square test or Fisher's exact test.
Pyuria, ≥5–9 WBCs/HPF; hematuria, ≥5–9 RBCs/HPF; UTI, urinary tract infection; GM, gentamicin; Tx, therapy; CVA, costovertebral angle tenderness; Azotemia, serum blood urea nitrogen ≥20 mg/dl and/or serum creatinine ≥1.4 mg/dl; APN, acute pyelonephritis; GM-R, gentamicin-resistant; GM-S, gentamicin-susceptible; CRP, C-reactive protein; HPF, high power field.
Clinical outcomes
Clinical outcomes were compared between the GM-R and GM-S groups (Table 2). The dose of gentamicin was 4.88±0.91 (mg/kg/day) in the GM-R group, and 4.80±0.77 (mg/kg/day) in the GM-S group (p=0.551). The duration of gentamicin was 5.26±2.44 days in the GM-R group and 6.73±1.81 days in the GM-S group (p<0.001), and durations of total antimicrobial therapy were 14.81±2.32 and 13.34±1.62 days, respectively (p<0.001). The early clinical response rates were 55.3% (26/47) versus 81.5% (185/227) at 72 hours, 61.7% (29/47) versus 96.9% (220/227) at 96 hours in the GM-R and GM-S groups, which was significantly higher in the GM-S group (p<0.001) (Table 2 and Fig. 1). However, the early clinical response rates at 24 and 48 hours were not significantly different between the GM-R and GM-S groups, though higher clinical response rates were noted in the GM-S group (Table 2 and Fig. 1). Mean time to defervescence were 51.4±23.7 and 51.4±22.8 hours in the GM-R (only in early clinical response positive patients) and GM-S groups, respectively (p=0.294). In the GM-S groups, mean time to defervescence in bacteremic and nonbacteremia APN patients were 66.1±22.5 and 48.1±22.1 hours, respectively. Overall, clinical cure rates were 100% (47/47) and 99.6% (226/227) in the GM-R and GM-S groups (p=1.000), respectively. APN patients in the GM-R group had longer hospitalizaton (9.72±3.46 and 7.89±2.27 days; p<0.001) than those in the GM-S group. No complications, such as death, progression to septic shock, and renal and perirenal abscess, occurred in either GM-R or GM-S groups (Table 2).
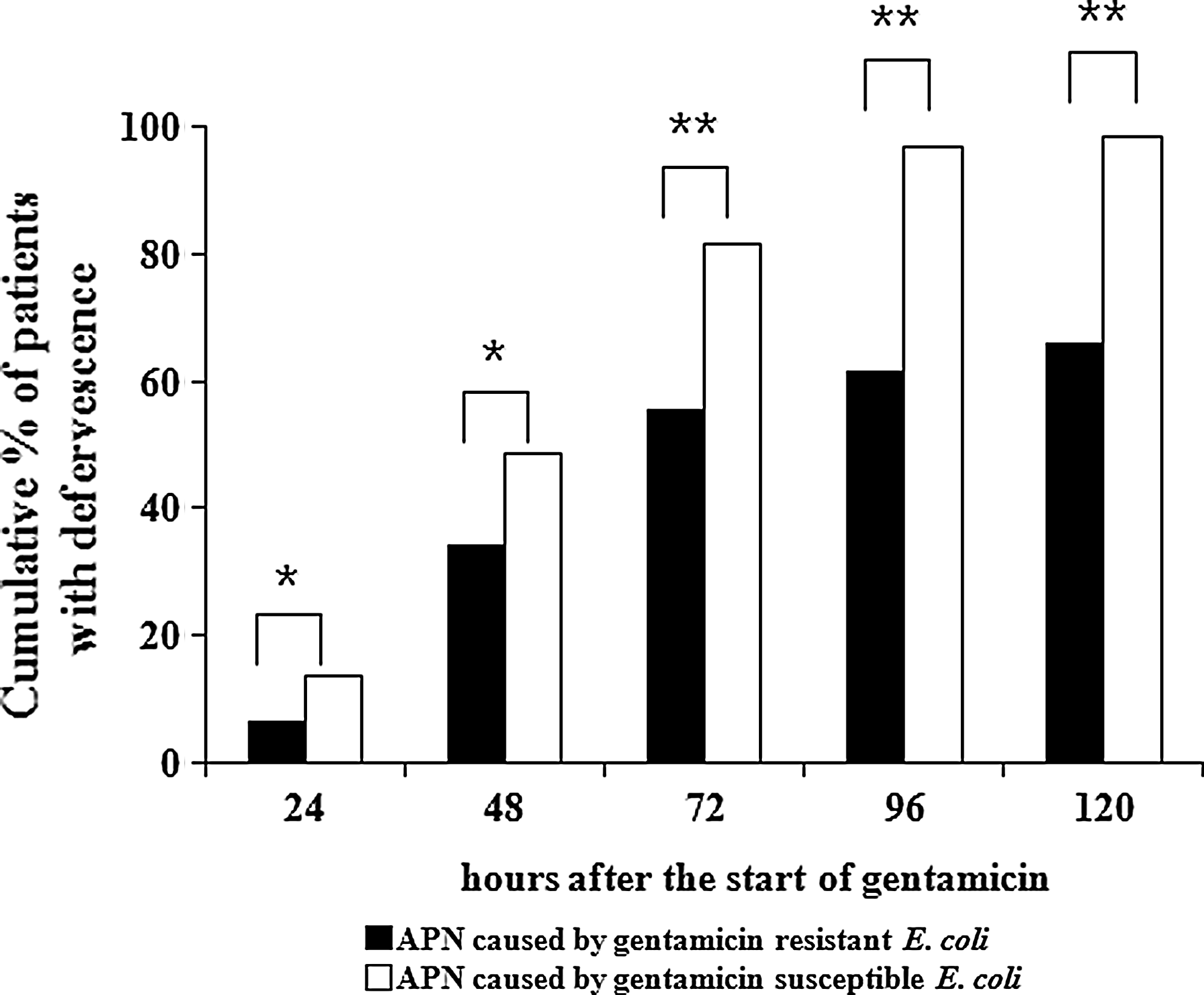
Cumulative percentage of all acute pyelonephritis patients in whom fever had resolved. *Statistically not significant; **p<0.001.
Data are shown as numbers of patients (% of total) or mean±standard deviation as appropriate.
By Mann–Whitney U test.
By Pearson chi-square test or Fisher's exact test.
Microbiological data
The antimicrobial susceptibility profiles of the 47 GM-R and 227 GM-S E. coli isolates are displayed in Table 3. Of the 274 E. coli isolates, the rate of susceptibility was 99.3% to amikacin; 85.4% to tobramycin; 82.8% to gentamicin; 40.3 to 65.9% to ampicillin, piperacillin, amoxicillin/clavulanate, and cephalothin; 98.0 to 98.9% to cefuroxime, cefotaxime, ceftriaxone, ceftazidime, and cefepime; 89.0% to ciprofloxacin; 66.1% to trimethoprim-sulfamethoxazole; 98.9% to piperacillin/tazobactam; and 100% to imipenem (Table 3). Susceptibility of E. coli for amikacin was significantly higher than gentamicin (99.3% vs. 82.8%; p<0.001). GM-S E. coli showed significantly higher susceptibilities for various antibiotics except imipenem than GM-R E. coli (p<0.01). In the GM-R group, susceptibility of E. coli for tobramycin was significantly higher than gentamicin (14.3% vs. 0%; p=0.008), and susceptibility for amikacin was significantly much higher than tobramycin or gentamicin (95.7% vs. 14.3% vs. 0%; p<0.001).
AMOX/CLA, amoxicillin/clavulanate; SXT, trimethoprim-sulfamethoxazole; TZP, piperacillin/tazobactam.
Risk-factor analysis for early clinical failure by comparing the early clinical response and failure groups
Among 274 cases, the number of the cases in the early clinical response group (at the 96 hour) was 248, and that of early clinical failure group was 26 (Table 4). There were no significant differences in age, the prevalence of menopause, initial body temperature, previous history of UTI, and antibiotic usage before hospital visit (Table 4). Initial leukocyte counts, CRP level were significantly higher, and the frequency of previous history of hospitalization, and the presence of bacteremia were also significantly higher in early clinical failure group. Furthermore, susceptibility of E. coli for gentamicin were significantly lower in the early clinical failure group (26.9% vs. 88.7%; p<0.001) (Table 4).
Data are shown as numbers of patients (% of total) or mean±standard deviation as appropriate.
By Mann–Whitney U test; bBy Pearson Chi-square test or Fisher's exact test
Antibiotic usage before visit, bacteremia, CRP level, menopause, previous history of admission, previous history of UTI, and resistance to gentamicin were the variables analyzed for evaluating effects of independent variable on early clinical failure. Bacteremia, CRP level, and resistance of E. coli to gentamicin showed significant differences, with p-values 0.016, 0.014, and <0.001 (Table 5).
Discussion
An intravenous antimicrobial regimen, such as an extended-spectrum cephalosporin, a fluoroquinolone, or an aminoglycoside, is recommended in women with pyelonephritis requiring hospitalization per the guidelines as updated by the Infectious Diseases Society of America (IDSA) and the European Society for Microbiology and Infectious Diseases (ESCMID). 5 Therefore, physicians may consider aminoglycosides, which achieve adequate renal tissue levels and induce ESBL resistance among Gram-negative bacteria less frequently than fluoroquinolones or broad-spectrum cephalosporins. However, in recent years, there is a lack of adequate studies with regard to the use of gentamicin in the treatment of uncomplicated APN.
Even though most APN are easily treated in clinical practice with antimicrobial agents, risk factors such as the need for hospitalization, a resistant infecting organism, diabetes mellitus, and a history of kidney stones were known to be associated with treatment failure in APN.17,20 Therefore, after excluding complicated APN occurring in patients with functional, structural urinary tract abnormalities, diabetes mellitus, and renal stones, we analyzed clinical courses and outcomes in hospitalized women with uncomplicated APN caused by GM-S or GM-R E. coli, who were initially treated with intravenous gentamicin.
As has been noted, overall clinical cure and mortality rate were not significantly different between the GM-R group and GM-S group, even though APN patients in the GM-R group had longer duration of total antimicrobial therapy, longer hospitalization, and lower early clinical response rate than those in the GM-S group. However, 29 (61.7%) cases of 47 cases having GM-R isolates showed resolution of fever within 96 hours after the start of intravenous gentamicin, and were included in early clinical response group, which might be explained by high concentrations of gentamicin in the urine and renal tissue. Furthermore, even 18 (38.3%) cases of 47 cases having GM-R isolates showed resolution of fever and improvement of symptoms after changing over to appropriate intravenous or oral antibiotics after microbiological diagnosis, and were finally considered to be clinical cured patients. These results suggest that aminoglycoside such as gentamicin might be used as the initial empirical antimicrobial agent in hospitalized uncomplicated APN, with a later change to other antimicrobial regimens concordant with microbiological susceptibility data.
In our study, we were able to confirm a higher rate of resistance of E. coli isolates to gentamicin in uncomplicated APN in Korea, compared with a lower rate of resistance of E. coli isolates to gentamicin in uncomplicated UTIs in North America and Europe. 7 In the ECO·SENS study on the antimicrobial susceptibility of E. coli causing community-acquired, acute, uncomplicated, nonrecurrent UTI in Europe, the resistance rates of E. coli to gentamicin were 1.3% and 0.7% in 2007–2008 and 1999–2000, respectively. 8 In the CANWARD surveillance study in Canada, the resistance rate of E. coli to gentamicin was 7.5% from 2007 to 2009. 9 APN patients in our study showed an early clinical response rate of 90.9% and finally, an overall clinical cure rate of 99.6%, in spite of higher rate of resistance of E. coli isolates to gentamicin (17.2%). In this study, amikacin exhibited significantly higher in vitro susceptibility rate than gentamicin (99.3% vs. 82.8%; p<0.001). Therefore, amikacin might be a good alternative to gentamicin in areas where the prevalence of gentamicin resistance is high, considering the longer duration of total antimicrobial therapy, longer hospitalization, and lower early clinical response rate in the GM-R group, though gentamicin can be used effectively in community-acquired uncomplicated APN patients, especially in resource-limited areas.
This study has a few limitations. First, this is not a randomized, controlled trial but a retrospective study. We investigated clinical and microbiological data within the homogeneous group of hospitalized women with uncomplicated APN only who received gentamicin as an initial empirical antimicrobial agent. Therefore, patients not admitted to the hospital and who did not receive gentamicin were excluded. This could represent a sampling bias. Second, it was not possible to assess bacteriological cure rate due to limitations in available microbiological data. Third, ototoxicity was estimated only subjectively, based on the medical records regarding dizziness, vertigo, or hearing impairment after gentamicin. Fourth, the data for previous use of antibiotics before current hospital visit, and for previous history of UTI, might be underestimated, as we included cases according to the discharge diagnosis and analyzed data in the medical records. A higher culture negative rate in this study might be partly explained by an underestimation of previous antibiotic use.
In conclusion, aminoglycoside such as gentamicin can be an alternative antibiotic option for initial empirical therapy of community-acquired uncomplicated APN in an era of increasing antimicrobial resistance, especially in areas where medical resources are limited or antibiotic resistance rate of the uropathogens is high. These results might be the basis for the use of aminoglycosides as the fluoroquinolone-sparing or broad-spectrum cephalosporin-sparing agents in the treatment of uncomplicated APN. For evidence-based use of aminoglycosides, much larger and adequately powered prospective trials are needed in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.