
Abstract
The main objective of this study was to assess the frequency and possible sources of colonization and infection by Acinetobacter in the intensive care unit (ICU) of a university hospital in Rio de Janeiro, Brazil, and characterize the isolates for relatedness to internationally and locally disseminated lineages. Patients consecutively admitted to the ICU from April 2007 to April 2008 were screened for colonization and infection. Species were identified by rpoB sequencing. The presence of acquired and intrinsic carbapenemase genes was assessed by polymerase chain reaction (PCR). Strains were typed by random amplification of polymorphic DNA (RAPD)-PCR, pulsed-field gel electrophoresis, and multilocus sequence typing (MLST) using the schemes hosted at the University of Oxford (UO) and Institut Pasteur (IP). Of 234 patients, 98 (42%) had at least one specimen positive for the Acinetobacter isolate, and 24 (10%) had infection. A total of 22 (92%) infections were caused by Acinetobacter baumannii and one each (4%) by Acinetobacter nosocomialis and Acinetobacter berezinae. A. baumannii isolates from 60 patients belonged to RAPD types that corresponded to MLST clonal complexes (CCs) 109/1 (UO/IP scheme, known as International Clone I), CC 110/110 (UO/IP), CC 113/79 (UO/IP), and CC 104/15 (UO/IP). Most CCs were carbapenem resistant and carried the blaOXA-23-like gene. Strains were introduced by patients transferred from other wards of the same hospital (11 patients, 18%) or acquired from cross-transmission within the ICU (49 patients, 82%). A. nosocomialis lineage sequence type 260 colonized 10% of the whole study population. A. baumannii have become established in this hospital as a part of a global epidemic of successful clones. Once introduced into the hospital, such clones have become entrenched among patients in the ICU.
Introduction
The development of multilocus sequence typing (MLST) simplified significantly the analysis of relatedness among A. baumannii international clones. Three European clones previously defined by amplified fragment length polymorphism and PFGE fingerprints were then recognized as International Clone (IC) I, II, and III by MLST.2,6,24 The successful dissemination of these strains was possibly related to their ability to accumulate resistance genes. However, other species, such as Acinetobacter nosocomialis, previously known as genomic species (gen. sp.) 13TU, 25 may also accumulate resistance genes.4,17 MLST schemes developed for A. baumannii allow definition of A. nosocomialis lineages, though no international clone of this species has been described to date. 30
There are currently two MLST schemes in use to define A. baumannii sequence types (STs) and clonal complexes (CCs): one hosted at Institut Pasteur (IP, www.pasteur.fr) and another at the University of Oxford (UO, www.pubmlst.org). In 2011, the spread of two multidrug-resistant OXA-23-producing A. baumannii CCs was described throughout eight hospitals in Rio de Janeiro: CC 113/79 (UO/IP) and CC 104/15 (UO/IP).3,10 Recently, transmission of an IC I blaOXA-23-positive A. baumannii isolate from a donor lung to a transplant recipient was reported in Rio de Janeiro. 22
Published data about the isolation frequency of Acinetobacter in Brazil are restricted to case–series studies, and refer main to collections of carbapenem-resistant isolates.7,8,21,27 Such studies are unlikely to provide estimates of the distribution of the Acinetobacter lineages causing colonization and infection. This prospective cohort study was carried out at a university-affiliated hospital in Rio de Janeiro, Brazil, where, in recent years, Acinetobacter isolates became endemic agents of healthcare-associated infections. Its primary aim was to describe the distribution of Acinetobacter species isolated from patients admitted to the intensive care unit (ICU) of this hospital and to characterize the relatedness of local strains to internationally circulating clones. We hypothesized that patients staying in the ICU served as an active ground for Acinetobacter species multiplication and spread.
Materials and Methods
Setting
Hospital Universitário Clementino Fraga Filho (HUCFF) is a 474-bed public university hospital in Rio de Janeiro, Brazil. Acinetobacter-related infections were rare at HUCFF until 2000 when A. baumannii emerged as a main agent of hospital-acquired primary BSI (data not shown) and, ever since, has become endemic. Four years later, carbapenem resistance was first detected in A. baumannii at HUCFF. The 16-bed medical-surgical ICU, where the study was performed, had about 49 admissions per month during the study period. Hand hygiene facilities were conveniently located with six sinks, chlorhexidine liquid soap, and paper towels. Alcohol-based gel dispensers were available at the bedside. The environment was cleaned as suggested by the Infection Control Committee using alcohol- or chlorine-based solutions. The study was approved by the Institutional Review Board of HUCFF (protocol No. 120/06).
Study design and definitions
This report analyzes data from a prospective cohort study of colonization or infection by Acinetobacter species among patients admitted to the ICU from April 17, 2007, through April 14, 2008. Subjects staying in the ICU for ≥72 h were included in the study. Patients admitted to the ICU were screened for colonization with Acinetobacter isolates by cultures of respiratory (tracheal or oropharyngeal) secretions and rectal swab specimens at admission, on the third day after admission, and then weekly until discharge or death. A case of colonization was defined as a patient with the isolation of an Acinetobacter isolate from a nonsterile site, with no evidence of infection. A case of infection was defined as any patient with symptoms or signs of infection, according to the judgment of the Infection Control Committee medical staff and isolation of Acinetobacter, following standard infection definitions. 15 Clinical specimens for diagnosis of infection were collected according to the attending physician's judgment and were routinely cultured at the clinical microbiology laboratory of HUCFF, with no interference of the study team. Acinetobacter isolate detection was stratified by occurring within or after 24 h of admission to the ICU. When the first Acinetobacter isolate was detected within 24 h of admission, the strain was classified as imported to the ICU, and when detected after 24 h of admission and preceded by a negative screening specimen, the strain was classified as acquired in the ICU.
Microbiological procedures
Clinical specimens were collected with moistened swabs (screening specimens) or by standard techniques (for investigation of infectious episodes). Blood samples were inoculated into BacT/ALERT (BioMerieux, Askim, Sweden) bottles and subcultured onto blood agar and chocolate agar. Samples were subcultured onto MacConkey agar at 36°C for 48 h. After phenotypic identification, isolates were stored as 10% skim milk–10% glycerol suspensions at −20°C. Isolates identified as Acinetobacter species in the clinical microbiology laboratory of HUCFF were also stored. Susceptibility to 11 antimicrobial agents was determined for all isolates by disk diffusion; minimum inhibitory concentrations (MICs) were determined in triplicate by the broth microdilution test to colistin, and by Etest (bioMérieux, Solna, Sweden) to imipenem and meropenem for A. baumannii isolates that caused infection. 5 Multidrug resistance (MDR) was defined as resistance to drugs belonging to at least three of the following drug classes: aminoglycosides (amikacin, gentamicin, and tobramycin), ampicillin-sulbactam, carbapenems (imipenem and meropenem), fluoroquinolone (ciprofloxacin), colistin, extended-spectrum cephalosporin (cefepime and ceftazidime), piperacillin-tazobactam, and trimethoprim-sulfamethoxazole. 19 Extensively, drug-resistant (XDR) isolates were those susceptible to drugs in only one or two of these antimicrobial categories. 19
Species identification
A partial rpoB gene sequence was analyzed as proposed. 12 Polymerase chain reaction (PCR) amplicons were purified with the QIAquick DNA kit (Qiagen, CA), sequenced, and 351-bp overlapping sequences were compared to a set of reference strains. 12
Detection of carbapenemase encoding genes
Production of metallo-β-lactamase was screened by a double-disk synergy test as described previously. 26 The presence of the following carbapenemase-encoding genes was investigated by a multiplex PCR: blaOXA-23-like, blaOXA-24-like, blaOXA-51-like, blaOXA-58-like, blaOXA-143, blaGIM-1, blaIMP-type, blaSIM-1, blaSPM-1, and blaVIM-type.14,23 The nucleotide sequences were determined for all representative bands and compared to reference sequences in the GenBank database.
Strain typing
All Acinetobacter isolates were typed by random amplification of polymorphic DNA (RAPD)-PCR with primer M-13, as described. 11 Band patterns were analyzed with GelCompar version 4.01 (Applied Maths, Kortrijk, Belgium) using the Dice coefficient and unweighted pair group method with arithmetic average. Isolates with 100% level of similarity were included in a single RAPD genotype. To validate RAPD-PCR results, a sample of 15 A. baumannii and 3 A. nosocomialis isolates of the predominant RAPD types were selected for PFGE, performed with ApaI. 28
Multilocus sequence typing
Isolates from the predominant A. baumannii RAPD types were selected for MLST analysis. MLST schemes hosted at IP (www.pasteur.fr) and at the UO (PubMLST, www.pubmlst.org) were performed as suggested.2,24 CCs (referred from now on by the UO/IP scheme) were defined for isolates with five or more identical alleles by eBURST software (http://eburst.mlst.net) and minimum spanning tree analysis (www.pasteur.fr), for data obtained with UO and IP schemes, respectively.
Statistical analysis
Fisher or chi-square test was used to compare resistance prevalence with EPI Info 6.0 software. Statistical significance was defined as p<0.05.
Results
Study population, detection of Acinetobacter, and identification of species
During the study period, 502 patients were admitted to the ICU: 235 (46.8%) stayed ≥72 h in the ICU, and 1 patient did not consent to participate. Of the 234 patients included in the study, 98 (41.9%) had at least one specimen positive for Acinetobacter species. In 32 patients (13.7% of the 234), the first screening was positive within 24 h of ICU admission: 22 were from other wards in HUCFF, 7 from other hospitals, and 3 from the emergency room. Among 202 patients who had a negative screening at admission, 66 were positive after 24 h of ICU hospitalization (late acquisition), with an overall cumulative incidence of 32.7 case–patients/100 admissions. Infections caused by Acinetobacter species occurred in 24 patients (prevalence: 10.2/100 admissions), including BSI (n=14), ventilator-associated pneumonia (n=7), infection of a vascular access (n=2), and intra-abdominal infection (n=1). In 5 cases, infection was present at admission; other 19 cases occurred after 24 h, with a cumulative incidence of 9.4/100 admissions.
A total of 255 Acinetobacter isolates were obtained from the 98 patients (1–14 per patient), distributed into five species. The predominant species was A. baumannii: 177 isolates obtained from 70.4% (n=69) of the patients. The second most frequent species was A. nosocomialis: 72 isolates from 48% (n=47) of the patients. Other species isolated were as follows: Acinetobacter soli, obtained from three patients; Acinetobacter berezinae, obtained from two patients; and one Acinetobacter gen. sp. close to 13TU. Eighteen patients (18.3%) had A. baumannii and A. nosocomialis isolates concomitantly. Positive specimens were mostly tracheal secretions and rectal swabs. A. soli and Acinetobacter gen. sp. close to 13TU were obtained only from oropharyngeal swabs. Of the 24 infections, 22 (91.7%) were caused by A. baumannii, 1 by A. nosocomialis, and 1 by A. berezinae. The monthly prevalence and distribution of cases of colonization or infection caused by A. baumannii and A. nosocomialis are shown in Figure 1. The prevalence of patients with A. baumannii during December 2007 (37.8%) was higher than the maximum expected value of 35.5% (mean monthly prevalence±1.96×standard deviation=15%±20.5); thus, a cluster of cases occurred during this month. An elevated number of A. baumannii infections diagnosed after 24 h in the ICU contributed for this increase. The time-based distribution of A. nosocomialis (Fig. 1) did not show clusters.
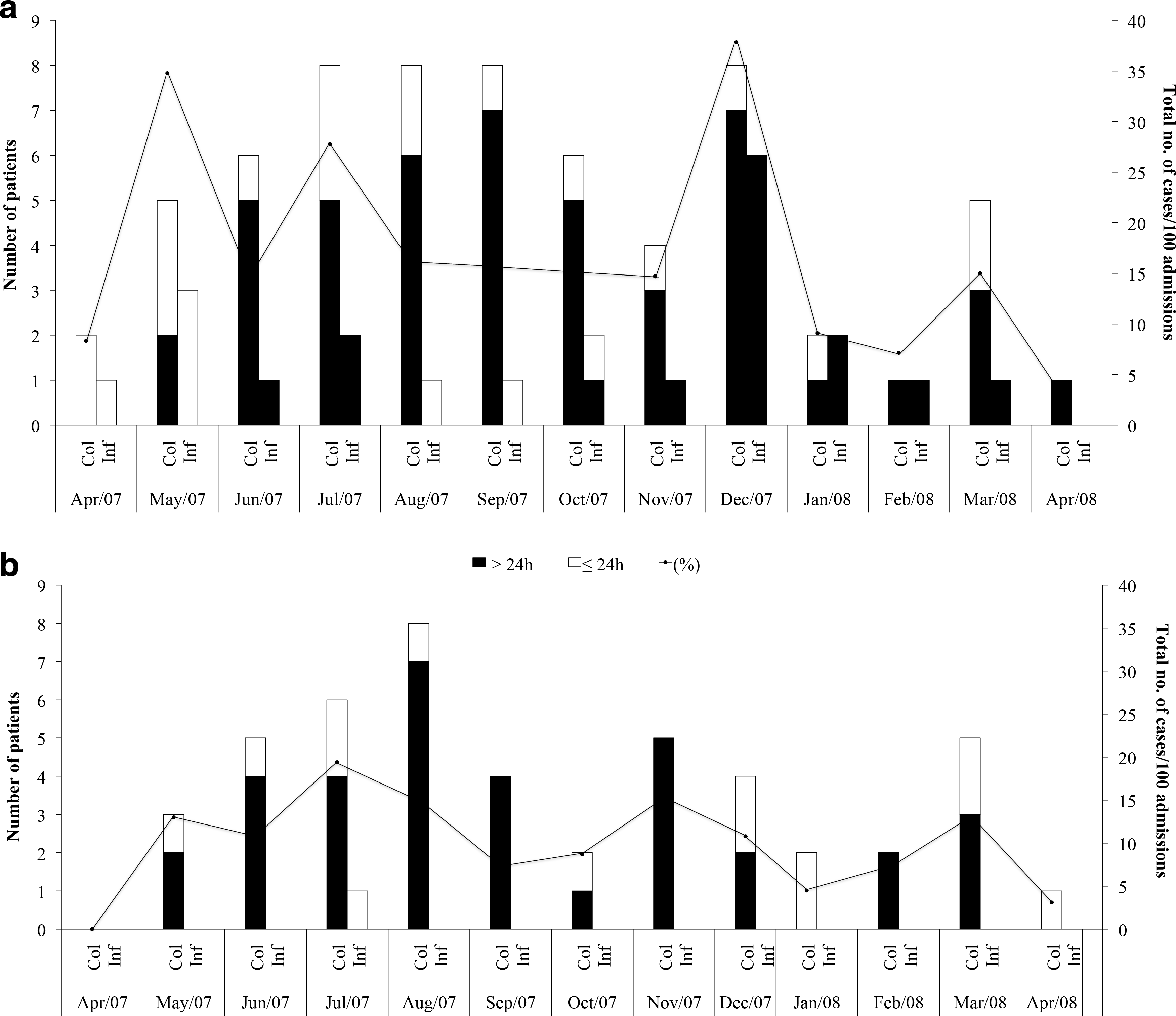
Prevalence curve and distribution of cases of infection (Inf) and colonization (Col) detected >24 h (gray bar) or≤24 h (white bar) after admission by A. baumannii
Strain types
RAPD typing of A. baumannii identified 28 types. Representative RAPD fingerprints are shown in Supplementary Figure S1 (Supplementary Data are available online at www.liebertpub.com/mdr). PFGE performed for 18 isolates showed equivalent clusters, with up to four band differences among isolates of the same type. Ten representative isolates of the five predominant types (A to E, two of each) were selected for MLST. For internal analysis of the transmission dynamics of clones within the study ICU, isolates with an RAPD band profile indistinguishable from the one selected for MLST were considered as belonging to the same CC.
Both MLST schemes clustered the representative isolates of Rio de Janeiro into four CCs, including IC I, as shown in Table 1. Clusters formed by the UO scheme and by the IP scheme were congruent. CCs corresponded to seven STs in the UO scheme, and none of them previously deposited in the PubMLST database, and five STs in the IP scheme, including a new one from a single isolate. The most common RAPD types B and E, corresponding to CC (113/79), affected 24 (34.8%) of the patients with A. baumannii, 10 of whom (42%) had infections, and was detected in 11 of the 13 study months, as shown in Figure 2. The second most common RAPD type A (CC 104/15) affected 13 (18.8%) of the patients.
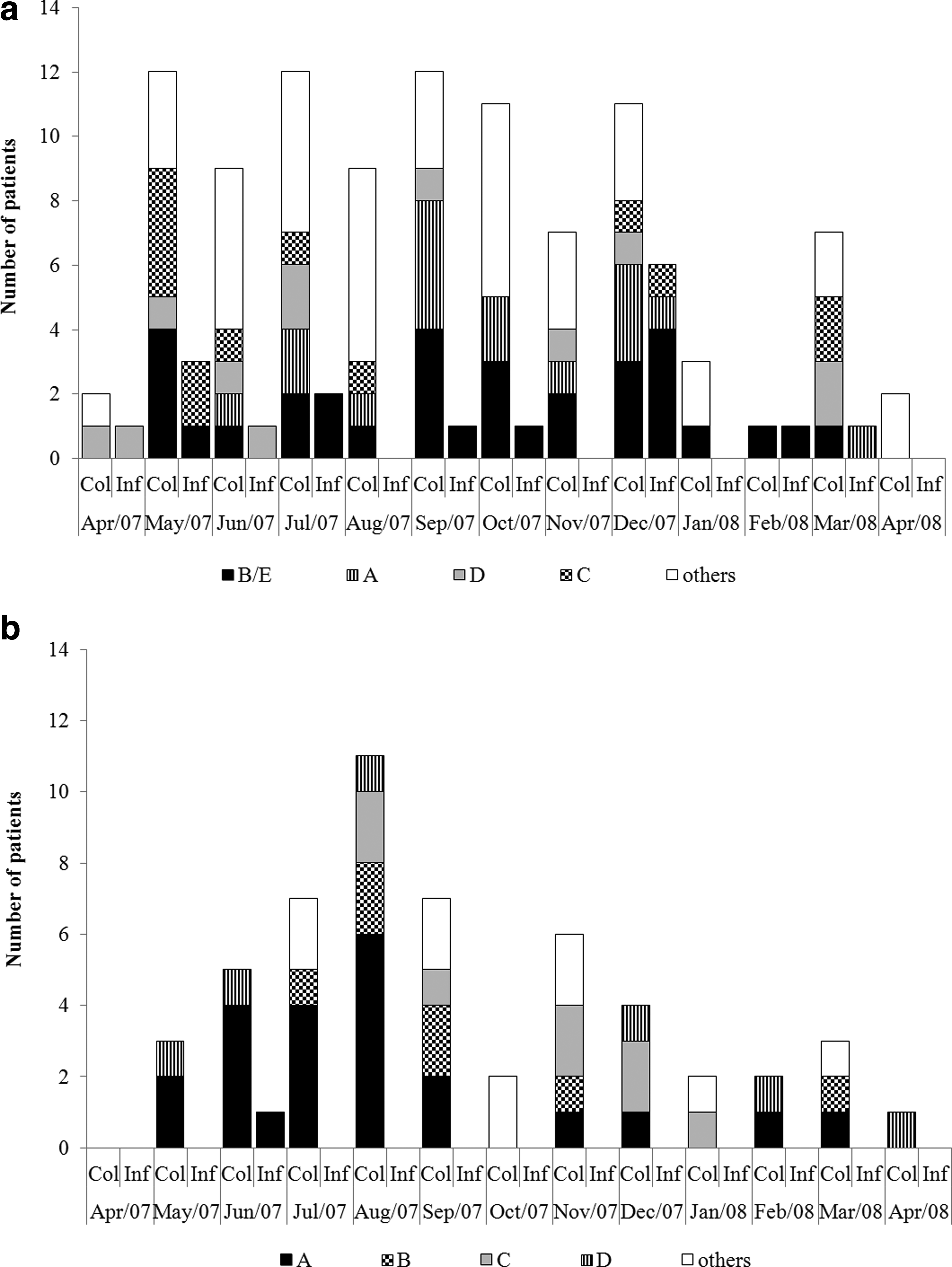
Temporal distribution of A. baumannii
Defined by RAPD and/or PFGE.
ST, sequence type; UO, University of Oxford MLST scheme; IP, Institut Pasteur scheme; CC, MLST clonal complex; RAPD, random amplification of polymorphic DNA; PFGE, pulsed-field gel electrophoresis; MLST, multilocus sequence typing.
RAPD typing of A. nosocomialis identified 12 types; a single type, called A, affected 24 (24.4%) of the patients (Fig. 2) and caused the single infection by this species. The two A. nosocomialis RAPD type-A isolates selected for MLST were included in a single ST by both MLST schemes: ST 260 of UO scheme and a new ST by IP scheme.
In Figure 3, cases caused by mainly A. baumannii and A. nosocomialis types are stratified by the supposed place of acquisition: within the ICU, which included most isolates; or imported to the ICU. Additionally, imported cases are further classified by the place of patient's origin—the hospital ward where patient was admitted before the ICU. A. baumannii strains were mostly introduced into the ICU with patients transferred from other HUCFF wards, while A. nosocomialis was introduced with subjects admitted from the emergency room and other hospitals.
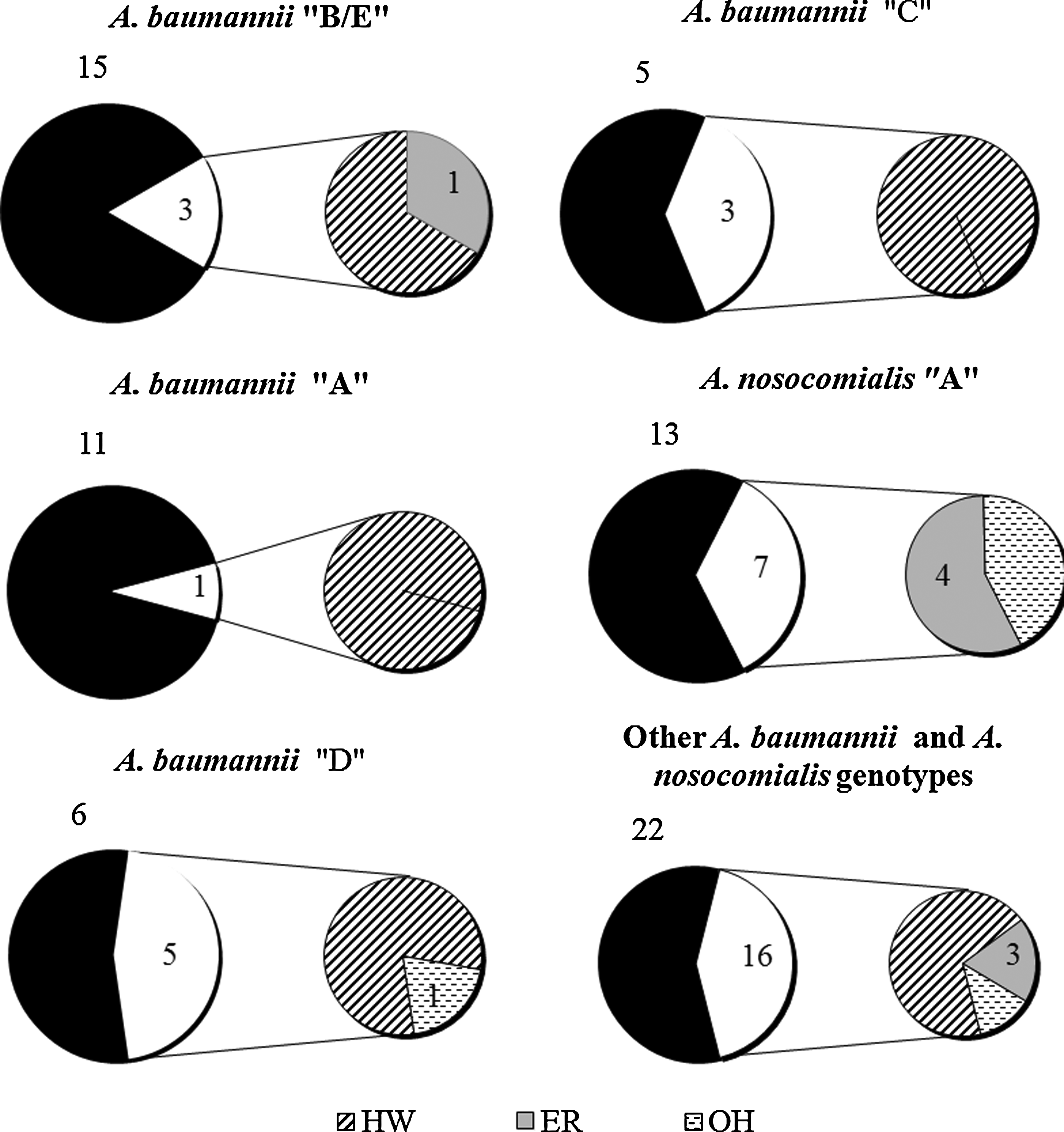
Representation of patients with main A. baumannii RAPD types (University of Oxford/Institute Pasteur [UO/IP] schemes) and A. nosocomialis genotype A (UO scheme) imported to the intensive care unit (ICU). RAPD types B/E, A, C, and D corresponded to following clonal complexes (UO/IP multilocus sequence typing scheme), 113/79, 104/15, 110/110, and 109/1, respectively. Only one isolate of each RAPD genotype per patient was included. White areas are cases diagnosed <24 h of admission. Black areas are cases diagnosed >24 h of admission. HW, patients from non-ICU wards of HUCFF; ER, patients from emergency room; and OH, patients from other hospitals.
Antimicrobial susceptibility and presence of carbapenemase genes
Most isolates included in the major A. baumannii lineages were XDR. The 17 (25%) carbapenem-susceptible A. baumannii isolates were diverse, belonging to 13 RAPD types. A resistance prevalence of >50% to an antimicrobial agent and an MDR or XDR phenotype were significantly more frequent in A. baumannii than in A. nosocomialis (p<0.05, Table 2). All 22 A. baumannii isolates that caused infections had MICs of meropenem and imipenem >32 μg/ml. The six isolates of A. soli, A. berezinae, and A. gen. sp. close to 13TU were susceptible to all antimicrobial agents tested.
p<0.05 for all comparisons between resistance in A. baumannii and A. nosocomialis.
A single isolate of each RAPD genotype of each species per patient is included.
Isolate resistant to meropenem or imipenem.
All A. baumannii isolates had the natural β-lactamase-encoding blaoxa-51-like gene. The blaOXA-23-like gene was detected in 144 (81%) of the A. baumannii and in two A. nosocomialis isolates. Resistance prevalence was significantly higher (p<0.05) in A. baumannii containing the blaOXA-23-like gene than in the blaOXA-23-like gene negative for amikacin, ampicillin-sulbactam, cefepime, ciprofloxacin, ceftazidime, piperacillin-tazobactam, carbapenems, and trimethoprim-sulfamethoxazole. The blaOXA-23-like gene-positive A. baumannii isolates were distributed in all CCs; no other blaOXA genes or metallo-β-lactamase-encoding genes were found.
Discussion
This is the first cohort study of patients presenting colonization and infection by Acinetobacter species, including susceptible and resistant isolates with strain typing data from Brazil. We describe a high incidence of colonization and infection by Acinetobacter isolates in the ICU of a large urban public referral hospital over 1 year; most of these were related to hospital transmission of highly successful clones. Prospective surveillance led to the observation that imported and ICU-acquired colonization by Acinetobacter species occurred, respectively, in 13.7% and 32.7% of patients. Those numbers are very high, twice as many as those detected in a similar study by Arvaniti and collaborators in a Greek ICU, where 5.6% and 15.7% of patients had imported and ICU-acquired colonization by Acinetobacter species. 1 Notably, about 24% of the colonized patients in the present study had infections.
Most of the isolates included in the main CCs were ICU born or came from other wards of the same hospital. The A. baumannii polyclonal outbreak in December 2007, with a high number of infections, suggests a deterioration in the quality of healthcare.
RAPD typing, validated by PFGE and complemented with MLST, was convenient and allowed classification of isolates into international clones. Strain typing detected a highly clonal population of A. baumannii isolates in the ICU, indicating intense cross-transmission of strains. The frequent admission of patients carrying successful clones from other wards or hospitals and poor staffing (not measured in the study) might have facilitated this scenario.
All STs detected by the UO scheme were new, but just one of the IP schemes was not described previously. The UO MLST scheme was more discriminatory than the IP scheme, possibly due to significant variations in the gyrB and gpi genes, as observed previously. 13 The predominant CC 113/79 was originally described in Argentina, and is highly successful in Rio de Janeiro. 10 This CC affected the largest number of patients, followed by CC 104/15. These data are in line with the study by Grosso and collaborators, performed with 96 A. baumannii isolates from Rio de Janeiro; CC 113/79 was also the predominant (70%), followed by CC 104/15 (25%), present in seven and five hospitals of the city, respectively. 10 In contrast with those authors, the present study also found that CC 110 and IC I strains disseminated in 17% and 16% of the patients with A. baumannii-positive cultures, respectively. The oldest IC I strain (HK302) was isolated in 1977 in Switzerland 18 and subsequently disseminated widely in Europe, East Asia, and Australia (http://pubmlst.org/abaumannii/).
Although A. nosocomialis was frequently isolated from screening specimens, it caused only one case of BSI in the present study. Recently, A. nosocomialis was reported as more prevalent than A. baumannii in blood cultures from patients admitted to hospitals in Norway. 16 Unfortunately, the distribution of Acinetobacter species by ward was not described in that report. In the present study, a single lineage of A. nosocomialis affected more than 10% of all patients. In fact, either this species has a clonal structure, or A. nosocomialis ST260 (UO scheme) is a highly successful clone in this hospital. Moreover, two blaOXA-23 gene-positive A. nosocomialis isolates recovered could indicate that this Acinetobacter species may provide, indeed, an efficient reservoir of resistance determinants. Another study documented the dissemination of a single A. nosocomialis strain, characterized by ribotyping, PFGE and amplified ribosomal DNA restriction analysis, over 23 patients, causing an outbreak in an ICU in the Netherlands. 29
In conclusion, the intense input of patients carrying Acinetobacter species observed in the ICU showed that subjects from other wards of the same hospital served as reservoirs of the pathogen.
Footnotes
Acknowledgments
This work was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Comissão Fullbright-Brasil, Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ), and Agência Nacional de Vigilância Sanitária (ANVISA) of Brazil and the Fogarty International Program in Global Infectious Diseases (TW006563) of the National Institutes of Health. The authors thank platform Genotyping of Pathogens and Public Health (IP) for coding MLST alleles and profiles. This publication also made use of the A. baumannii MLST Website (![]() ) developed by Keith Jolley at the UO (Jolley and Maiden 2010, BMC Bioinformatics, 11:595). Finally, we thank Leif Sorenson, who carefully reviewed the article.
) developed by Keith Jolley at the UO (Jolley and Maiden 2010, BMC Bioinformatics, 11:595). Finally, we thank Leif Sorenson, who carefully reviewed the article.
Author Disclosure Statement
All authors report no conflicts of interest relevant to this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.