
Abstract
Multidrug-resistant Acinetobacter baumannii infections are serious challenges for clinicians because of A. baumannii propensity to acquire resistance to a wide spectrum of antimicrobial agents. In this study, 91 A. baumannii isolates from patients in tertiary intensive care units of three university hospitals in the north, central, and south of Iran were selected and tested for susceptibility to 22 antimicrobials; amplified restriction fragment polymorphism and multiplex polymerase chain reaction methods were used to determine genetic relationships and International Clone (IC) of A. baumannii isolates, respectively. Twenty-four genotypes were identified in A. baumannii isolates. About 91.2% of isolates categorized into 4 distinct clusters; one was more heterogeneous and observed across the three locations. A considerable number of the isolates (27.5%) belonged to the novel IC variant, sequence group 7 (SG7), which was geographically widespread in three locations. The drug resistance pattern showed that 14.2%, 20%, and 77% of the A. baumannii isolates were resistant to colistin, tigecycline, and rifampicin, respectively. Nine percent of isolates (8) showed simultaneous resistance to colistin, rifampicin, and tigecycline. Interestingly, all of them were susceptible to ampicillin–sulbactam and/or tobramycin. According to our results, SG7 could be considered as a pan-Iranian clone.
Introduction
Spreading of carbapenem-hydrolyzing β-lactamases (carbapenemases) compromise the clinical efficacy of these efficient antibiotics, a situation that is an issue of concern, therefore urgently needs antibiotic alternatives.21,33,39,44 Despite the fact that no new drugs are currently in the pipeline to eliminate infections, surveillance of the activities of currently available agents that determine combinations are urgently needed to guide physicians to make decisions regarding the treatment of patients infected with such an alarming bacteria. 37 Several studies have demonstrated that carbapenem-resistant A. baumannii (CR-AB) infection is usually treated with a combination of three antibiotics—colistin, rifampicin, and tigecycline.9,13,21,23,29 Decrement of susceptibility to these three anti-CR-AB drugs has recently been reported among patients with A. baumannii infection in several countries.21,22,25,31,34
Genotyping allows epidemiological investigation of clonal transmission dynamics in outbreaks, which can be used as an important tool to identify the source of the original infection.5,8 Several epidemiological typing methods have been developed. 11 The Amplified fragment length polymorphism (AFLP) is a well-validated high-resolution DNA fingerprinting method that can be used on any DNA disregarding its origin. 15 Three international A. baumannii clones, the so-called European clones I, II, and III, are implicated in outbreaks worldwide and associated with carbapenem resistance.28,43
To date, no studies have addressed the efficacy of rifampicin and its combination with colistin or tigecycline against CR-AB and distribution of the dominant International clones (ICs) that cause infections in different areas of Iran. The objectives of the present study were (i) to compare the susceptibility of A. baumannii isolates at hospitals in the north, center, and south of Iran, (ii) to determine the relatedness of A. baumannii isolates of Iran to IC, and (iii) to investigate the molecular epidemiology of A. baumannii isolates in Iran using AFLP-based genotyping in comparison with known ICs.
Materials and Methods
Definition
A. baumannii is defined as MDR when the organism is resistant to at least one agent in three or more antimicrobial categories that would otherwise serve as treatments for Acinetobacter infection. 18
Isolates
A total of 94 nonrepetitive isolates of Acinetobacter spp. were isolated from several clinical sources, including the respiratory tract, postoperative wound, urine, blood, and cerebrospinal fluid (CSF) during February 2012 to June 2012 from ICUs of three university hospitals in the north (Gonbad), center (Tehran), and south (Shiraz) of Iran. The records provided the time of specimen collection.
Species of the isolates were identified initially using the API 20NE system (BioMérieux) and thereafter confirmed by polymerase chain reaction (PCR) for blaOXA-51-like genes.2,41 All clinical A. baumannii isolates were kept at −20°C in CRYOBANK™ (Copan Diagnostics, Inc.) until further testing.
Antimicrobial susceptibility testing
The Clinical and Laboratory Standards Institute (CLSI) guideline for the disk diffusion method was used to assess susceptibility to ampicillin/sulbactam, cefepime, cefotaxime, ceftazidime, ceftriaxone, ciprofloxacin, doxycycline, gentamicin, imipenem, levofloxacin, meropenem, minocycline, piperacillin, tetracycline, ticarcillin, ticarcillin/clavulanic acid, tobramycin, trimethoprim/sulfamethoxazole. 24 Minimum inhibitory concentration (MIC) values of all isolates for polymyxin B, colistin, tigecycline, and rifampicin were determined by the microbroth dilution method as described by the CLSI guideline. MICs of colistin and polymyxin B were interpreted according to the CLSI breakpoints. However, no breakpoints for tigecycline and rifampicin are available in the CLSI guidelines; therefore, the criteria of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) for members of the Enterobacteriaceae and CLSI criteria for Staphylococcus spp. were applied to tigecycline and rifampicin, respectively.24,36 MIC90 were calculated for these antimicrobials. All antimicrobial agents were purchased from Mast Diagnostics Ltd., except polymyxin B and tigecycline powders (both items were purchased from Sigma-Aldrich). During each test, Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as quality control organisms to ensure accuracy of the antimicrobial susceptibility assays.
Determination of clonal type
IC, the so-called European clones (EC) or sequence group (SG), were identified using two multiplex PCR sets (Table 1) amplifying group 1 (assigned as EC II), group 2 (assigned as EC I), and group 3 (assigned as EC III) alleles of the outer-membrane protein A (ompA), chaperone–subunit usher E (csuE), and the intrinsic carbapenemase (blaOXA-51-like) genes were used as previously described (Fig. 1). 40

Multiplex PCRs designed to selectively amplify ompA, csuE, and blaOXA-51-like alleles of standard strains belonging to Group 1, Group 2, and Group 3. All strains belonging to the Group 1 international clonal complex yielded all three fragments in the Group 1 PCR (lane 1), and none in the Group 2 PCR (lane 2), while strains belonging to the Group 2 gave the expected converse results (lanes 3 and 4), despite some mismatches between the primer sequences. Strains belonging to Group 3, which gave the top two fragments (for the other two loci) in the Group 1 PCR (lane 5) and share the same ompA allele as Group 2, gave only the middle fragment (for ompA) in the Group 2 PCR (lane 6). Lane labeled M contains a size ladder. PCR, polymerase chain reaction; ompA, outer-membrane protein A, csuE, chaperone–subunit usher E.
Nucleotide.
AFLP, amplified fragment length polymorphism; PCR, polymerase chain reaction; ompA, outer-membrane protein A; csuE, chaperone–subunit usher E.
Molecular typing
Epidemiological types of all A. baumannii isolates were determined by amplified restriction fragment polymorphism (AFLP) using the Vos method with some modifications. 42 Briefly, extracted bacterial DNA was quantified by UV-spectrophotometry (Eppendorf, Inc.) and analyzed by agarose gel electrophoresis to verify DNA integrity. DNA samples were double digested with Mbo I and Mse I (both items were purchased from Fermentas). To ligate the resulting double digested DNA (ddDNA) fragments to the corresponding adapters (Table 1), ddDNA products were added into a reaction mixture containing double-stranded adaptors and T4 DNA ligase (Takara Bio). The ligation products were diluted and used as a template for preliminary amplification, which contained the PreAmp-Mbo and PreAmp-Mse primers (Table 1) and PCR mastermix (Arya-Tous BioTec). The preamplification reaction thermal cycling consisted of preheating at 94 C for 4 min, 35 cycles of 94 C for 30 sec, 60 C for 30 sec, and 72 C for 90 sec, and final extension at 72 C for 5 min (Palm cycler; Corbett Life Science). Then, preamplified products were diluted 1:100 and used for the selective PCR amplifications to generate AFLP profiles. Selective amplification was performed as described earlier with selective primers. The reaction condition was preheating at 94 C for 4 min, 35 cycles of 40 sec at 95 C, 40 sec at 62 C, 80 sec at 72 C, and final extension at 72 C for 5 min. An initial screening of 24 combinations of selective primers was performed using four Mb1-4 (PreAmp-Mbo+A, +T, +C, +G) and four Ms1-4 (PreAmp-Mse +A, +T, +C, +G) (Table 1). The primer combination (Mb4-Ms4) generated the most clear and evenly distributed bands and was chosen for selective amplifications as well as AFLP analyses of all samples.
To determine the AFLP genotypes, the selective PCR products were separated by electrophoresis on 2% (w/v) agarose gels. Gel images were analyzed with BioNumerics version 5.10 (Applied Maths) using A. baumannii NCTC 12156 as a normalization reference. The similarity between the band patterns was calculated using the Dice coefficient (with an optimization of 0.5% and a position tolerance of 1%). The AFLP clusters and type identification were defined by groups formed at 60% and 90% Dice similarity cutoffs, respectively, on a dendrogram constructed by the unweighted-pair group method using average linkages (UPGMA). 28
Statistical analysis
Statistical analysis, including Fisher's exact tests and the chi-squire test were performed with the SPSS software package (version 18). In all the experiments, p-values<0.05 were considered significant.
Results
Species identification
From the 94 isolates that were identified to be Acinetobacter spp. in the API 20NE system, the PCR for detection of the blaOXA-51-like genes confirmed 91 isolates as A. baumannii from the three locations: 44 isolates from Tehran, 27 isolates from Shiraz, and 20 isolates from Gonbad. The most common specimens from which A. baumannii was isolated were respiratory tract (44%; 40/91), followed by postoperative wound (32%), urine (11%), blood (10%), and CSF (3%).
Antimicrobial susceptibility testing
The antibiotic resistance profile of A. baumannii isolates from three locations is shown in Table 2 and 3. A. baumannii strains were resistant to 5–19 antibiotics per isolate (mean of 13) of 22 antibiotics; all isolates were resistant to ceftriaxone and cefepime. Tehran, Shiraz, and Gonbad had 91%, 89%, and 75% MDR phenotypes, respectively. Fortunately, despite alarming rates of imipenem resistance, only 4.9% of imipenem-resistant A. baumannii isolates were resistant to colistin. All our imipenem- and colistin-resistant A. baumannii isolates remain sensitive to tigecycline, whereas all these showed resistance to rifampicin. The drug resistance pattern showed the MICs of polymyxins (colistin and polymyxin B), tigacycline, and rifampicin ranged between <0.25–16, 0.25–8, and 2–64 μg/ml, with MIC90 values of 4, 2, and 16 μg/ml and overall resistance rates of 14%, 20%, and 77%, respectively (Table 2). All isolates resistant to colistin were also resistant to polymyxin B and vice versa. Nine percent of isolates showed resistance to colistin, rifampicin, and tigecycline (CRT) simultaneously. CRT resistance varied at each of the three locations, 11.4% (5/44) and 11.1% (3/27) of Tehran and Shiraz isolates showed CRT-resistant antibiotypes, respectively. All of the A. baumannii isolates taken from Gonbad were susceptible to colistin. Interestingly, all of the eight CRT resistance isolates were susceptible to ampicillin–sulbactam and/or tobramycin. Six CRT-resistant isolates were from respiratory tract specimens, one was from an operative wound specimen and the other one was from a patient with urinary tract infection and the other one was from an operative wound specimen.
Considerations in the assignment of agents to Groups A and B include clinical efficacy, prevalence of resistance, minimizing emergence of resistance, cost, FDA clinical indications for usage, and current consensus recommendations for first-choice and alternative drugs. Group A is considered appropriate for inclusion in a routine, primary testing panel, as well as for routine reporting of results for the specific organism. Group B comprises agents that may warrant primary testing. Group C includes agents that have a clinical indication for the organism. 24
Drug susceptibility was performed using the microbroth dilution protocol that determines the minimum inhibitory concentrations.
CSF, cerebrospinal fluid; CAZ, ceftazidime; CIP, ciprofloxacin; CRO, ceftriaxone; CST, colistin; CTX, cefotaxime; DOX, doxycycline; FEP, cefepime; GEN, gentamycin; IPM, imipenem; MEM, meropenem; MIN, minocycline; LVX, levofloxacin; PB, polymyxin B; PIP, piperacillin; RIF, rifampicin; SAM, ampicillin/sulbactam; SXT, trimethoprim/sulfamethoxazole; TET, tetracycline; TGC, tigecycline; TIC, ticarcillin; TIM, ticarcillin/clavulanic acid; TOB, tobramycin.
This study showed that the majority of rifampicin- and tigecycline-resistant isolates (81.8% and 22.7%, respectively), were found in Shiraz and Tehran, respectively. The MDR trait was higher among A. baumannii isolates from pneumonia than isolates from postoperative wound infection (Table 3). Based on our antibiotic susceptibility test results, colistin-susceptible A. baumannii (CS-AB) isolates showed higher antimicrobial resistance rates (6 to 19 antibiotics per isolate; mean of 16) than CR-AB isolates (5 to 14 antibiotics per isolate; mean of 10). Among all the selected antibiotics, gentamicin, tobramycin, imipenem, and tetracycline resistance rates showed significant difference between CS-AB and CR-AB isolates, 93.5% versus 69.2% (p=0.03), 76.9% versus 46.1% (p=0.039), 74.3% versus 23% (p=0.001), and 52.5% versus 92.3% (p=0.018), respectively. One CR-AB isolate from Shiraz, which was derived from the bloodstream, had a non-MDR phenotype.
Determination of clonal type
Nine different SGs were identified among the 91 A. baumannii isolates (Figs. 2 and 3). Considerable number of the isolates (27.5%; 25/91) belonged to the novel variant sequence group 7 (SG7) (Table 4). Twenty one (23%) isolates pertained to 6 other novel variant of SGs, defined according to the new combination of amplified products obtained from the two separate multiplex PCRs that did not correspond to previously defined SG1, SG2, and SG3 (EC II, I, and III, respectively) (Table 5). SG7 was as geographically widespread in three locations, could be considered as the pan-Iranian clone. A. baumannii isolates with the SG7 clone were assigned to various AFLP types (Fig. 3). In our study, no SG3 was found in 91 isolates.
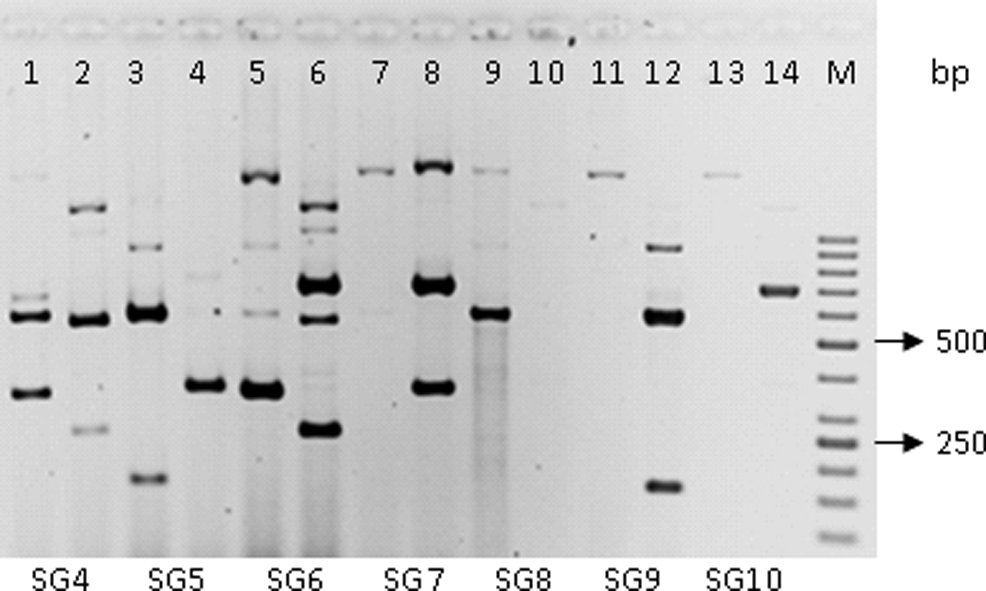
Examples of multiplex PCRs designed to selectively amplify ompA, csuE, and blaOXA-51-like alleles of isolates belonging to variant sequence groups that defined according to new combinations of amplified products obtained in the two separate multiplex PCRs that did not correspond to previously defined sequence groups 1, 2, and 3. Lanes 1, 3, 5, 7, 9, 12, 13 yielded fragments in the Group 2 PCR and lanes 2, 4, 6, 8, 10, 11, 14 yielded fragments in the Group 1 PCR. Lane labeled M contains a size ladder. The bottom of the figure showing the variant sequence groups found in this study according to yielded fragments in the Group 1 and 2 PCRs.
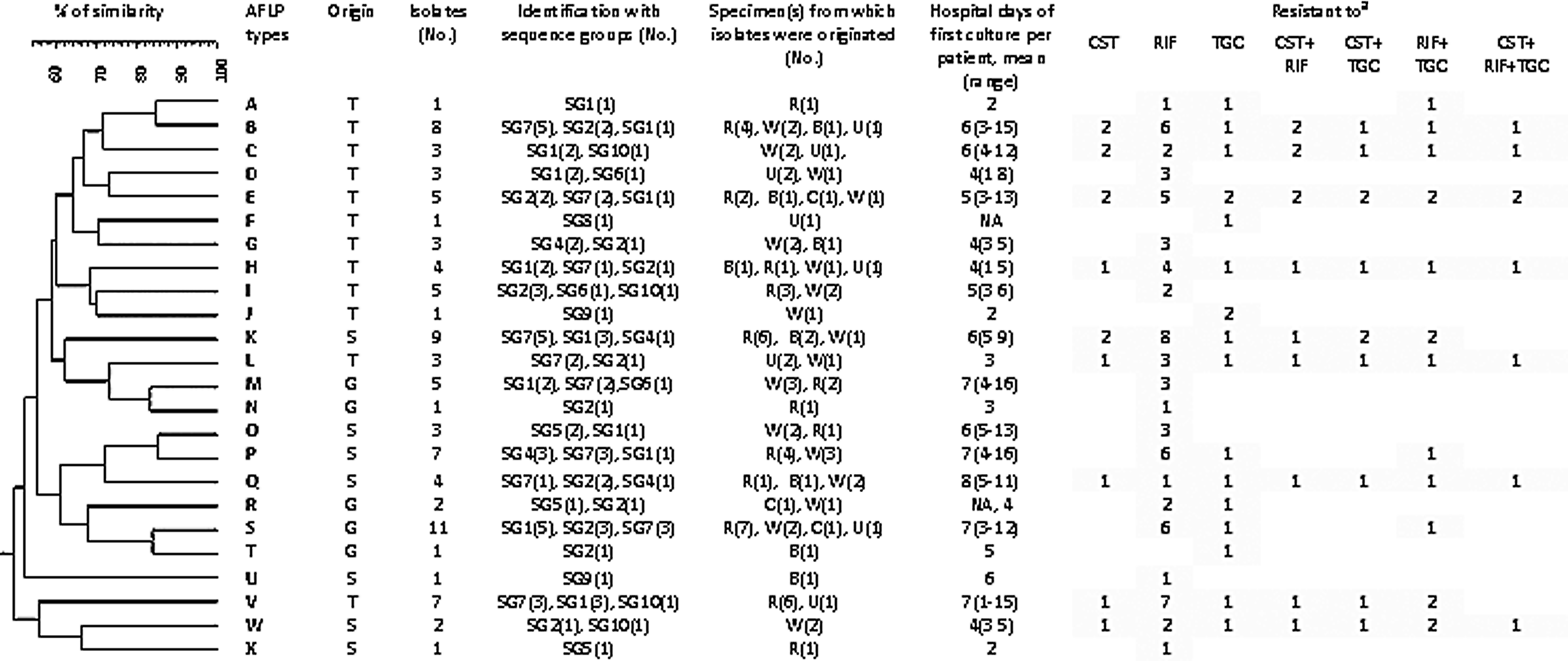
AFLP-based dendogram, summary of characters, origin, and resistance profiles of 91 Acinetobacter baumannii isolates in the present study. Dendrogram of different A. baumannii AFLP types produced using the Dice coefficient and UPGMA with a cutoff value of 90% similarity for differentiating closely related isolates. For cluster allocation, the cutoff level is 60%. AFLP, amplified fragment length polymorphism; UPGMA, unweighted-pair group method using average linkages. aT, Tehran; S, Shiraz; G, Gonbad; CST, colistin; RIF, rifampicin; TGC, tigecycline.
T, Tehran; S, Shiraz; G, Gonbad; R, respiratory tract; W, wound; C, cerebrospinal fluid (CSF); U, urine; B, blood; CST, colistin; RIF, rifampicin; TGC, tigecycline.
+, product present; −, no product.
Most of the isolates were derived from respiratory tract specimens that belonged to SG7 (15), SG1 (13), SG2 (7), and other SGs (5). In wound swab samples, 8, 7, 3, and 11 isolates were assigned to SG1, SG2, SG7, and the other SGs, respectively. Isolates attributed to urine samples were grouped to new variants (6), SG2 (3), and SG1 (1). Isolates derived from bloodstream samples were assigned to new variants (6) and SG2 (3). The CSF isolates belonged to SG1 (2) and SG2 (1). Our study demonstrated that 8.3%, 9.5%, and 16% of SG1, SG2, and SG7 were assigned to CRT-resistant antibiotypes, respectively. In this study, SG9 had the same pattern as a variable group described by Towner et al. 38 that yielded ompA fragment in the Group 1 PCR and csuE fragment in the Group 2 PCR. According to the best of our knowledge, this is the first time that the prevalence of ICs has been described in Iranian isolates.
Molecular typing
Dendrogram constructed the following AFLP pattern preparation and the results of cluster analysis of all A. baumannii isolates are shown in Fig. 3. Using a similarity index of ≥60% as the threshold categorized 91.2% of isolates into 4 distinct clusters (Fig. 3). Unclustered isolates (8.8%) comprised between 1 and 7 isolates originating from the same center. Almost 37.3% of the isolates clustered in one large cluster, including Tehran isolates. Cluster 2 was more heterogeneous with 4 AFLP types (K, L, M, and N) observed across three locations (Fig. 3). Two CRT-resistant MDR A. baumannii isolates had identical AFLP types (E), indicating infection with similar strains. There was no significant difference between distributions of the AFLP types among the three locations.
AFLP revealed that a total of 12, 7, and 5 different AFLP types were identified in Tehran, Shiraz, and Gonbad, respectively, at the strain cutoff level of 90%. Strains found in Tehran were slightly more heterogeneous with 12 AFLP types identified among 44 isolates (12/44; 27.2%), than strains found in Gonbad, with 5 AFLP types identified among 20 isolates (5/20; 25%). Each of the AFLP types A, F, J, N, T, U, and X was observed in one patient solely. The 17 remaining profiles were observed across multiple patients. Genotypes S and K were the most frequent, in 11 and 9 patients, respectively. Strain U also displayed a very low level of similarity (55%) to others and was clearly far less related to any of the other 90 isolates. The AFLP type V, S, and K comprised predominantly respiratory isolates (21%), which were isolated during 2–7 (mean of 5) days from initial hospitalization. AFLP types were not significantly related to culture sources for any of the 3 major types (V, S, and K) by the Fisher's exact test.
Correlation of A. baumannii genotypes with antibiotype and international clonal lineages
Genotypes A, F, J, N, T, U, and X corresponded to a unique SG comprising 6 strains. The other AFLP types were represented in more than one SG (Fig. 3). The AFLP types of the rifampicin-resistant A. baumannii strains identified in the three locations were further investigated, and the results are shown in Fig. 3. Eight of 12 (66.6%) rifampicin-resistant isolates obtained from Gonbad, were categorized to the same cluster, whereas rifampicin-resistant isolates from other locations showed more heterogeneous patterns.
The AFLP type analysis of all tigecycline-resistant A. baumannii strains revealed that 8 out of 10 (80%) Tehran isolates belonged to the same cluster, but isolates from two other locations were slightly more heterogeneous. The AFLP types of the CR-AB strains found in Tehran and Shiraz were evaluated; similar heterogeneity was found in colistin-resistant isolates. Among 8 CRT isolates, 6 (75%) included in this study had distinct genotype and antimicrobial resistance profiles. Two CRT isolates had the same AFLP type (E) with distinctive antibiotypes.
Discussion
Nosocomial infections caused by MDR A. baumannii are a major concern worldwide, especially in ICUs.4,7,17,31,34,39 In the current study, we have observed a high prevalence of the MDR phenotype (84.6%) in A. baumannii isolates from ICUs in agreement with other studies. 4 Increasing prevalence of MDR A. baumannii strains and limited treatment options have prompted the use of antibiotic combinations like tigecycline and colistin as therapeutic regimens.3,21 Resistance to tigecycline and colistin has been reported previously in two studies conducted in Tehran during 2009 to 2011.1,35 The present study revealed that 22.7% versus 8.8% and 18.2% versus 4% of A. baumannii isolates are resistant to tigecycline and colistin, respectively, by comparison with previous studies in Tehran.1,35 The definite and statistically significant increase in tigecycline and colistin resistance in this study might be due to differences in A. baumannii strains available for study or increasing empirical utilization of tigecycline and colistin since 2009 and consequent appearance of tigecycline- and colistin-resistant strains. Interstudy difference of collected isolates and higher prevalence of colistin resistance in Tehran hospitals may be justified by earlier empirical use of colistin in Tehran than medical centers, which are located farther away in small cities like Gonbad.
In this study, up to 77% of isolates were resistant to rifampicin. This high prevalence of rifampicin-resistant MDR A. baumannii is in consistent with the research conducted by Chang et al. 3 The nosocomial infection of MDR A. baumannii has been reported by several studies conducted in south, central, and northwest of Iran.1,14,30 Nevertheless, the localized intrahospital dissemination of MDR A. baumannii strains in north of Iran remains unclear. The present study showed that 80% of the isolates from north of Iran (Gonbad) belong to two AFLP types S and M. Thus, it is critical to assess the dissemination of A. baumannii in the hospitals of northern Iran through regular and continuous antimicrobial resistance surveillance and infection control programs. The intrahospital dissemination of MDR A. baumannii with resistance to tigecycline, colistin, and rifampicin is the main concern that hospitals must control.
In a timely manner, antimicrobial resistance surveillance and strict infection control strategies are still lacking in Iran, despite the alarming emergence of MDR strains of A. baumannii, particularly among those isolates that are not susceptible to colistin. This study shows that the intrahospital dissemination of CRT-resistant MDR A. baumannii isolates varies between the three locations. According to our AFLP fingerprinting data, slightly more heterogeneous MDR A. baumannii isolates are obtained from Tehran and Shiraz. These two locations receive more patients who are referred from smaller hospitals in nearby cities. Such referred patients can result in the spread of A. baumannii strains in hospitals. In contrast, the spread of MDR A. baumannii might account for the clonal dissemination of CRT-resistant isolates with different AFLP types in Tehran and Shiraz. This situation gives emphasis to the importance of periodical determination of the regional antibiotic susceptibility patterns and applying effective infection control strategies that can eradicate nosocomial strain of A. baumannii in hospitals.
It is now about 15 years since the first EC lineages were described. 6 Clonal lineages of A. baumannii were also described as IC or SG with a marked predominance of EC II, by investigation of isolates from mostly European countries and the United States. 45 Although only limited information is available concerning A. baumannii isolates in Asian countries. Some Asian countries like China, Pakistan, Singapore, South Korea, and Taiwan have investigated the European clonal lineage and they have been reported to be EC II. 12 In another study, the outbreak isolates in Turkey were not associated with A. baumannii strains of EC I, II, or III. 16 Diversity of the ompA, csuE, and blaOXA-51-like genes in A. baumannii has been reported in several studies. Towner et al. 38 identified four novel variants of SGs in 17 European countries. The results of their study demonstrated that the most prevalent novel variants of SGs in A. baumannii were SG that amplified blaOXA-51-like genes and ompA from amplifying group 1.12,38 A higher frequency of the novel variant of SGs in hospital-acquired strains of A. baumannii was observed in our study, and it is the first report of IC detection of A. baumannii in Iran. The novel variant, SG7, detected as predominant SG in Iran, could be considered as the pan-Iranian clone. The dissemination of the novel variant of clonal lineages has shown that these clones are clearly evolving particularly according to the antibiotic resistance genes, which they are harboring, and represent a serious challenge to eliminate A. baumannii outbreaks.12,38 Despite clonal variation in antibiotic susceptibility, usually the ICs are highly resistant to antibiotics, and it is conceivable that carbapenem resistance has substantially contributed to their spread in Europe. 26
Linkage analysis was performed for antimicrobial resistance profiles, IC lineages, and isolate sources. Our results have revealed remarkable correlations between CRT, IC lineages, and isolate sources. CRT-resistant strains are identified in 8.8% of isolates in our study, and predominant CRT resistance isolates are associated with SG7 and respiratory tract specimens in our isolate group. One CRT-resistant MDR A. baumannii isolate with identical AFLP profile is the same as other isolates with E AFLP type, probably indicating infection with identical strains.
All the CR-AB isolates in this study are more susceptible than CS-AB strains, which is consistent with the findings of Moffatt et al. 20 in their studies on A. baumannii clinical isolates. Interestingly, all of the 8 CRT resistance isolates are susceptible to ampicillin–sulbactam and/or tobramycin. This is very important for treating serious infections caused by colistin resistance A. baumannii. 20 However, this combination still needs to be validated in animal models and clinical trials. The results of this study are consistent with a recent report in which, a number of combinations exhibited a potent activity against MDR A. baumannii. 20 Studies demonstrate that CR-AB strains due to the increased expression of several efflux systems, such as adeIJK and macAB-tolC, results in increased sensitivity to other antibiotics and that this could be utilized in a combination in antibiotic therapy comprising colistin and a second antibiotic effective against CR-AB strains. 20 The difference in the prevalence of the colistin resistance strains found in clinical samples is probably due to the different selective pressures that bacteria are exposed to in different environmental conditions.
AFLP analysis grouped our isolates from three different locations of Iran into 24 distinct AFLP types. Cluster analysis of the AFLP patterns suggested that these outbreak isolates are genotypically quite diverse, and that outbreak strains of A. baumannii are low clonal, with a high diversity that may be caused by movement of insertion sequences, a feature already recognized as being important in A. baumannii. 26 These data support the view that the Iranian A. baumannii isolates are more diverse than the other locations in the world.12,38
The high rate of resistance to rifampicin in our isolates could be a reason for further investigation of the antibiotic susceptibility test in other medical centers to obtain a better estimation of the susceptibility pattern of A. baumannii in Iran. Suggestion of the antibiotic regimen is regional dependent, and accordingly, the database of antibiotyping results may help the clinicians for better decision making and better patient outcomes.
In conclusion, our data support that ampicillin–sulbactam alone or plus tobramycin exhibited a potent activity against CRT resistance A. baumannii isolates. Iranian A. baumannii strains are so heterogeneous and this is the first report of IC lineages of A. baumannii in Iran. SG7, the novel variant of IC, could be considered as the pan-Iranian clone. We also show that IC I and II were present in Iran at almost the same time as they were described worldwide.
Footnotes
Acknowledgments
This research has been supported by a study that was supported by the Tehran University of Medical Sciences & health Services grant 89-01-30/10430. We thank Dr. J. Kharazi for performing the statistical analysis.
Disclosure Statement
No competing financial interests exist.