
Abstract
We report the emergence and long-lasting persistence of linezolid resistance in an ampicillin-resistant Enterococcus faecium strain in the intestine of a neutropenic oncohematologic patient receiving chemotherapy. The patient was first colonized by an epidemic ampicillin-resistant E. faecium (ARE)-ST117 clustering into lineage 78. This clone exhibited resistance to levofloxacin, erythromycin and high-level resistance to streptomycin and gentamicin. After receiving treatment with several broad spectrum antibiotics for febrile neutropenia, a 9-day course of oral linezolid was administered once the patient developed bacteraemia by the same ARE colonizing clone. Linezolid-resistant ARE was detected 17 days later in the follow-up fecal samples and persisted 41 days after suppression of linezolid therapy. Resistance to linezolid was associated with G2576T transversion in the 23S rRNA and the presence of cfr gene was not detected. The persistence of G2576T-ARE strains, especially in oncohematologic patients with injured intestinal membranes, could increase the risk of bacteraemia.
Introduction
T
Linezolid resistance in enterococci has been increasingly noted since the first descriptions in the year 2006. 18 The most widely documented mechanism conferring resistance to linezolid in Enterococcus spp. is transversion G2576T in the domain V of 23S rRNA gene (Escherichia coli numbering). However, the expression of cfr gene (chloramphenicol-florfenicol resistance) encoding an rRNA methyltransferase, a well established mechanism in staphylococci, may be responsible for a number of cases in enterococci.6,13,20,26
In this work we report the intestinal colonization by an AREfm-ST117 belonging to lineage 78 and the later emergence and continuing persistence of linezolid-resistant AREfm-ST117 associated with G2576T mutation in the 23S rRNA after a short oral linezolid course.
Case Report
A 69-year-old male consulted for pancytopenia and was admitted to the Hematology ward with a diagnosis of acute leukemia. Levofloxacin (500 mg/24 hr oral) was administered as extended prophylaxis to prevent endogenous infections (day 0) and 10 days later induction to the remission chemotherapy (idarrubicin-cytarabin-panobinostat) was started. During admission the patient was screened for AREfm intestinal colonization, and on day 18, the first AREfm isolation was detected. Four days later (day +22) the patient developed febrile granulocytopenia (leucocytes: 1,300/μl, neutrophiles: 300/μl); blood cultures were collected and levofloxacin prophylaxis was discontinued to establish empirical treatment with piperacillin-tazobactam (4,000 mg/8 hr i.v.) plus vancomycin (1,000 mg/12 hr i.v.). On day 25, Staphylococcus epidermidis was recovered from blood cultures and 5 days later (day +30), when the patient became afebrile, vancomycin was discontinued but piperacillin-tazobactam was maintained. On day 33 (day +13 of neutropenia) fever reappeared and two days later blood cultures yielded an AREfm. Piperacillin-tazobactam was then discontinued and linezolid (600 mg/12 hr i.v.) was administered for 9 days until discharge (day +44) (see Fig. 1).
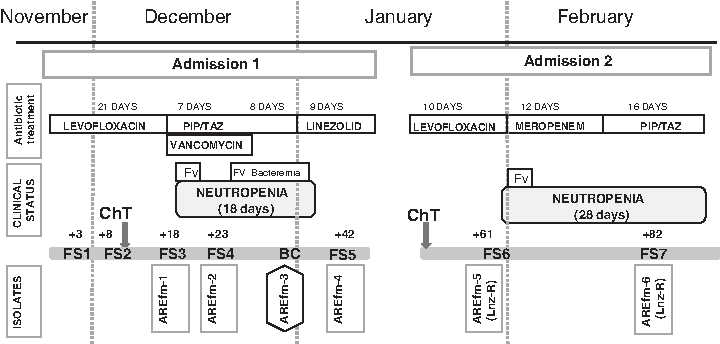
Chronological events occurring during patient admissions, clinical status, antibiotics administered and samples recovered along hospitalization. On the chronology line, samples are marked as FS (feces sample) or BC (blood culture) and above them, the days after admission when collection was performed. In turn, clinical status, extended levofloxacin prophylaxis, and antibiotic treatment are shown on top, while AREfm isolation is displayed in the lower part. Abbreviations: ChT (beginning of chemotherapy), AREfm (ampicillin-resistant Enterococcus faecium), PIP/TAZ (piperacillin-tazobactam), and Fv (fever).
A week later (day +51), the patient was readmitted to receive a 7 day cytarabine-idarubicine reinduction chemotherapy course. During this admission two stool samples were collected and linezolid-resistant AREfm was recovered from stool (FS6) on day +61. Moreover, the patient presented severe neutropenia and developed fever for which meropenem (1,000 mg/8 hr i.v.) therapy was administered. Fever reappeared 12 days later (day +73) and meropenem was changed to piperacillin-tazobactam (4,000 mg/8 hr i.v.) until discharge. On day +82 and 41 days after linezolid discontinuation, linezolid-resistant AREfm was again recovered from a colonization stool sample (FS7).
Material and Methods
Samples collection, identification, and antimicrobial susceptibility testing
The patient was included in a prospective ecological study aimed at screening for intestinal colonization with AREfm and follow-up stool samples were collected weekly (Fig. 1) (approved ethical committee reference number CEIC-106/09). Throughout the hospital stay, 7 feces samples were collected: 5 during the first admission (FS1 to FS5) and 2 during the second admission (FS6 and FS7). They were all screened for AREfm by seeding in m-Enterococcus agar (Difco; Becton Dickinson) supplemented with ampicillin (10 μg/ml). Plates were cultivated 48 hr at 37°C, and then, a pale pink colony was restreaked on Columbia blood agar (Oxoid) for identification and susceptibility testing. The bacteraemic isolate (BC- AREfm-3), recovered during the first admission, was also included in the study.
Bacterial identification was performed by mass spectrometry (MALDI TOF MS, Bruker-Daltonics) and antibiotic susceptibility was tested by an automated commercial microdilution method (MicroScan; Siemens). A gradient diffusion method (Etest; bioMérieux) was performed to confirm linezolid resistance.
Clonal diversity study
Clonal relatedness was established by pulsed field gel electrophoresis (PFGE) 5 and multilocus sequence typing (MLST) was performed for a further study. The PFGE patterns were interpreted by using the criteria proposed by Tenover et al. 25 designating those isolates with closely related patterns as belonging to a single clone. Sequence type (ST) was assigned according to the STs described in the MLST database (www.mlst.net).
Investigation of linezolid resistance
Linezolid resistance was characterized both by PCR amplification-sequencing of a 389-bp fragment of an internal region of domain-V in 23S rRNA genes 15 and pyrosequencing. Analysis of the 2576G/T polymorphism by pyrosequencing was performed according to Sinclair et al. specifications. 22 In addition, amplification of the 746 bp 23S rRNA region containing A2503 position, which is the target for cfr methyltransferase, was performed as described elsewhere. 13
Study of virulence determinants
The presence of esp gene, which codifies the Enterococcal surface protein (Esp) associated with increased virulence and colonization 27 and hyl gene, which encodes a glycoside hydrolase that facilitates intestinal colonization and peritoneal invasion, 2 was studied by multiplex-PCR. 28
Results
On day +17 during the first admission, AREfm was detected in feces (FS3) and from then, the colonization persisted until discharge (day +44) (samples FS4 and FS5) (Fig. 1). During his second admission, the patient remained colonized by AREfm, but this time isolates exhibited resistance to linezolid (samples FS6, FS7)
All bacteremic and colonization isolates (n=6) presented high-level streptomycin (>1,000 μg/ml) and gentamicin (>500 μg/ml) resistance, as well as resistance to levofloxacin (>4 μg/ml) and erythromycin (>4 μg/ml) and were susceptible to vancomycin (≤1 μg/ml), teicoplanin (≤2 μg/ml), and daptomicin (≤1 μg/ml). Moreover, isolates AREfm-5 and -6, recovered from fecal samples, which were collected 20 (FS6) and 41 (FS7) days after having stopped linezolid therapy, were resistant to this antibiotic (32 and 24 μg/ml, respectively),
SmaI-PFGE revealed that all isolates (stool and bacteraemia), including both linezolid susceptible and resistant isolates, and were genetically related according to international criteria 25 (Fig. 2). Moreover, MLST analysis resolved these isolates in the sequence type (ST) 117, a single locus variant of ST17, which belonged to the hospital adapted population previously designated as CC17 and now clustered in lineage 78 as belonging to BAPS 2-1 subgroup according to Willems et al. 30 The presence of virulence genes, esp and hyl, was demonstrated in all AREfm isolates
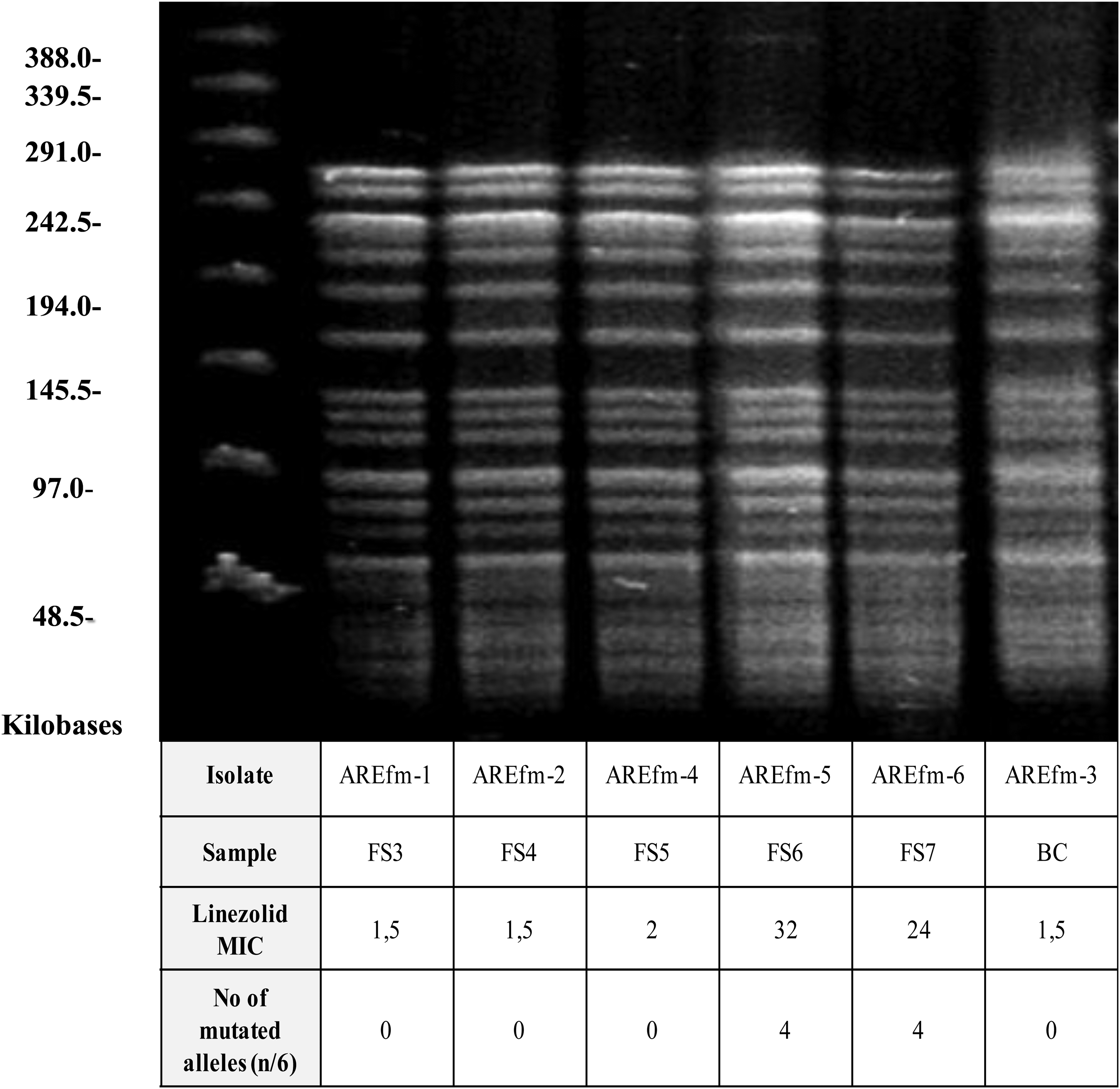
SmaI pulsed field gel electrophoresis (PFGE) pattern, linezolid MICs and number of 23S RNA mutated alleles of AREfm isolates. Lane 1: Lambda ladder; lanes 2, 3, and 4, AREfm feces isolates (FS) susceptible to linezolid; lanes 5 and 6, AREfm feces isolates resistant to linezolid; lane 7, AREfm bacteraemic (BC) isolate susceptible to linezolid.
Isolates AREfm-5 and AREfm-6 harbored the mutation G2576T in the 23S rRNA, while no linezolid-susceptible-AREfm presented this point mutation. Pyrosequencing confirmed that these linezolid-resistant isolates bore G and T at position 2576 in a 1:2 ratio indicating the presence of the T2576 polymorphism in four out of six alleles. None of the AREfm isolates harbored the cfr gene.
Discussion
Linezolid, an oxazolidinone with bacteriostatic activity against gram-positive bacteria, has proved to be safe-effective when treating multidrug resistant enterococcal infections in neutropenic patients. 23 Nevertheless, emergence of linezolid resistance mainly during long-term treatment of enterococcal infections, has been documented.3,7,21,24 We report the emergence of linezolid-resistant AREfm in the intestinal compartment of an oncohematologic patient after a 9 day treatment and its long persistence once linezolid was discontinued.
Molecular analysis of linezolid resistant strains showed that the 23S rRNA genes harboured the G2576T point mutation and pyrosequencing estimated the number of mutated alleles as four. E. faecium possesses six copies of this gene and a single mutated allele seemed to be sufficient to confer resistance. Furthermore, the greater the number of mutated alleles the higher the levels of MICs observed. 15 In enterococci, spontaneous mutation rates in genes conferring linezolid resistance are low (10−9–10−11), 16 but once this mutation is expressed and successful, the selective antibiotic pressure in the intestine can select these mutants. Levofloxacin extended prophylaxis and piperacillin-tazobactam administered during febrile neutropenia, before linezolid resistance development, could have contributed to enrich the AREfm population. It has been demonstrated that antibiotics with antianaerobic activity, such as piperacillin-tazobactam or meropenem, promote high-density colonization of multidrug-resistant enterococci. 9 Although in our study we did not quantify the amount of enterococci in stools, we observed a high-density of AREfm in the stool samples recovered during the antibiotic treatment. The probability of spontaneous mutations conferring linezolid-resistance is more likely to occur secondary to this AREfm intestinal overgrowth. Even though it has been described that linezolid elimination occurs preferably in the urine and only a small amount is excreted as inactive metabolites via feces, 8 low linezolid concentrations in the stool of the healthy volunteers were found, as well as a marked reduction in the enterococci population. 14 This finding supports the hypothesis that a small amount of linezolid in the intestinal compartment could be sufficient to select these linezolid-resistant mutants and suppress the susceptible enterococcal population. Furthermore, after the emergence of linezolid-resistant enterococci in our patient, the administration of levofloxacin and meropenem during the second admission could have contributed to the maintenance and persistence of these resistant mutants. Even if we cannot rule out the potential exogenous acquisition of the linezolid resistant isolate, the continuous monitoring of antimicrobial susceptibility in E. faecium demonstrated the absence of linezolid resistant isolates in both clinical and colonizing isolates in our hospital (data not shown).
Long term persistence of these strains in the gut is a remarkable event since these patients could act as a reservoir of linezolid resistant-AREfm, facilitating cross transmission between hospitalized-patients, especially in hospitals with high linezolid consumption. 12 This has been demonstrated in nosocomial outbreaks caused by clonal enterococcal strains carrying the G2576T mutation in the 23S rRNA gene. 11 Furthermore, colonization by linezolid resistant-AREfm could be an important risk in oncohematologic patients since they are more likely to develop bacteraemia and other infections as a consequence of neutropenia and chemotherapy induced-mucositis. This should be taken into account, particularly in countries where vancomycin resistant-E. faecium is endemic and linezolid has become the main therapeutic option, as this emergence could compromise therapeutic alternatives and successful outcomes.
Footnotes
Acknowledgments
This work was supported by research grant FIS-PS09/00825 from Instituto de Salud Carlos III, Ministry of Economy, Spain.
Disclosure Statement
No competing financial interests exist.