
Abstract
The purpose of this study was to identify carbapenem-resistant Klebsiella pneumoniae in a tertiary care hospital in Sharjah Emirate, to identify the plasmids carrying the carbapenemase genes and to reveal clonal relationships among the isolates. Two hundred and two clinically relevant isolates collected between September 2011 and October 2012 at Al-Qassimi hospital, Sharjah, were investigated for meropenem resistance. Strains with decreased susceptibility were further tested with the modified Hodge test, by EDTA and phenylboronic acid synergy and by E-test. The genes of New Delhi metallo-β-lactamase (NDM), IMP, VIM, OXA-48, and KPC beta-lactamases were targeted by polymerase chain reaction and the genes were located on plasmids by Southern blotting. Clusters of the isolates were revealed by macrorestriction analysis. Seven percent of the isolates were originally found to be meropenem resistant, one isolate have lost its resistance during storage. All of the 13 resistant isolates were positive for the NDM-1 gene located on plasmids of 125 to >170 kb, while three isolates also carried the blaOXA-48-like genes. Clusters having repeatedly been isolated over the study period were identified. Carbapenem-resistant Klebsiella pneumoniae carrying the blaNDM-1 gene is a fast emerging problem, emphasizing the potential role of the Middle East as a secondary reservoir for these organisms.
Introduction
C
Materials and Methods
Study site and strains
The study was carried out at Al-Qassimi hospital, a 350-bed tertiary care hospital of the Ministry of Health in Sharjah, UAE. Two hundred and two consecutive, independent, clinically relevant strains of K. pneumoniae isolated between September 2011 and October 2012 were included in this study. Strains were initially identified by the MicroScan Walk Away® system (Siemens Healthcare Diagnostics, Inc., West Sacramento, CA) and this was subsequently confirmed manually using the API 20E®enteric identification system (bioMerieux, Inc., Hazelwood, MO). Strains were stored at −80°C in Tryptic Soy Broth (Oxoid, Basingstoke, United Kingdom) containing 10% glycerol.
Patient's data, including age, gender, travel history, month of detection, ward, specimen, and antimicrobial susceptibility patterns were collected.
Carbapenem susceptibility testing and carbapenemase detection
Susceptibility testing was performed on Mueller–Hinton agar (Oxoid) using a 10 μg meropenem disc (Mast Diagnostics) according to the Clinical and Laboratory Standards Institute (CLSI) guidelines 3 (CLSI, Wayne, PA). Strains with decreased meropenem susceptibility were further tested by E-test according to CLSI guidelines. 3
The modified Hodge test (MHT) was used 4 to detect carbapenemase production as recommended by the Centers for Disease Control (CDC, Atlanta, GA). 2 Synergism was tested between meropenem and EDTA to detect metallo-beta-lactamases or between meropenem and phenylboronic acid (PBA) to identify class A carbapenemases. 20
Detection and characterization of carbapenemase genes
Isolates were tested for the genes of IMP, VIM, OXA-48, and KPC beta-lactamases in separate PCRs using the primers described by Poirel et al. 15 Genes of the NDM beta-lactamases were detected by primers as described by Ghazawi et al. 7 DNA extracts from the following strains were used as controls: K. pneumoniae GR-KPC2 for KPC, Enterobacter cloaceae ABC104 for VIM, 19 K. pneumoniae ABC52 for NDM, 18 K. pneumonaie KP No.16 for OXA-48-like 5 , and Pseudomonas aeriginosa OEK-IMP for IMP PCR. PCR amplification and direct sequencing was used to determine the allele of the blaNDM genes, as described. 7
Plasmid analysis and Southern blotting
The plasmid profile of the isolates was established using the alkaline-lysis method 10 and the molecular mass of the plasmids were estimated as described. 18 Plasmids separated by agarose gel electrophoresis were capillary-transferred to Hybond-N+ membranes (Roche, Mannheim, Germany) and the blaNDM gene was localized on the plasmids by probing the membranes with a blaNDM or with a blaOXA48-like specific probe labeled with a digoxigenin-alkaline phosphatase labeling kit (Roche), according to the manufacturer's instructions, as described. 18
Molecular typing
Genetic relatedness of the strains was tested by pulsed field gel electrophoresis (PFGE) of the XbaI-digested genome 6 followed by the analysis of the PFGE patterns by GelCompareII software (Applied Maths, Sint-Martens-Latem, Belgium). The Dice similarity coefficient (SD) was calculated with a 1.5% position tolerance. Strains with SD≥80% were clustered into a pulsotype.
Results
Using the disc diffusion screening, 14 of the 202 K. pneumoniae isolates (7%) were found to be resistant to meropenem. The characteristics of the isolates along with the data collected on the patients are listed in (Table 1). Of the 202 isolates, sixty-eight percent of the strains were isolated from intensive care unit (ICU) patients, 14% from internal medicine, and rest 18% from surgery wards, respectively. Fifty-four percent of the isolates were recovered from urine, 19% from respiratory tract, 16% from exudates, 7% from blood samples, and 4% from central venous catheters. The retrospective data collection of the patients with CRKP infection revealed that only 2 of the 14 patients had travel histories during the previous 6 months outside of the UAE, but none of them traveled to India. There was no death attributed to CRKP infection during the study period.
BLD, blood; ETT, endotracheal tube; UR, urine; MMW, male medical ward; ICU, intensive care unit; URO, urology; FMW, female medical ward; CCU, coronary care unit; MSW, male surgical ward; A, ampicillin; Ag, augmentin; Ak, amikacin; Az, aztreonam; C, cefotaxime; Cz, ceftazidim; Cf, ceftriaxone; Cm, cefipime; Cp, ciprofloxacin; L, levofloxacin; O, ofloxacin; I, imipenem; M, meropenem; G, gentamicin; P, pipercillin; NDM, New Delhi metallo-β-lactamase.
When the MIC testing was performed after recovering the isolates from the −80°C storage, only 13 of the original 14 strains exhibited MIC values above the resistance breakpoint (≥4 mg/L), while one strain (No. 6) showed susceptibility to meropenem (MIC=0.5 mg/L). The 13 meropenem-resistant strains were further tested with phenotypic carbapenemase detection. With the exception of isolate No. 5, all 13 strains exhibited positive MHT, and all showed >5 mm increase in the inhibition zone when meropenem was combined with EDTA. No inhibition was seen with PBA.
Screening for common carbapenemase genes by PCR detected blaNDM in all 13 meropenem resistant strains with three isolates also positive for blaOXA-48-like gene, while no carbapenemase gene was detected in the isolate converting to meropenem susceptible after storage. Sequencing of the entire blaNDM gene revealed the blaNDM-1 allele in all 13 isolates.
Plasmid analysis of the 13 strains revealed 2–6 plasmids in each isolates (data not shown). Plasmids of ∼170 kb or above hybridized with the NDM-1 probe in 10 of 13 the isolates. Isolate No. 13 contained two plasmids of ∼170 and 125 kb size and both gave a signal with the NDM probe. Two isolates with identical plasmid profile (No. 4 and 5) showed hybridization signal with a plasmid of approx.140 kb size (Table 1, Fig. 1). OXA-48 hybridization localized the gene in isolate No. 3, 10, and 14 on plasmids of identical size (<7.4 kb) (data not shown).
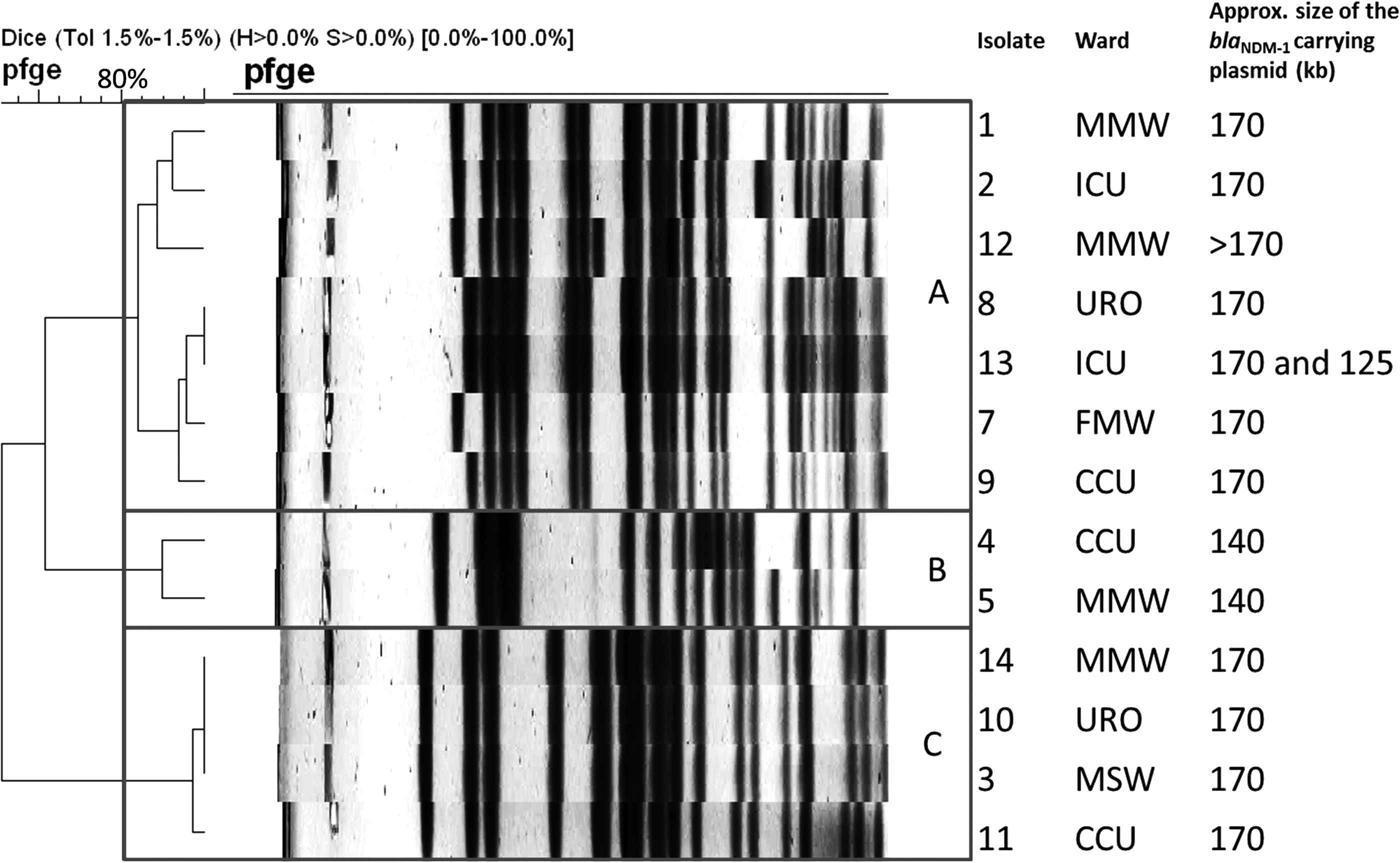
PFGE comparison of carbapenem resistant Klebsiella pneumoniae isolates. Boxes labeled A–C represent pulsotypes with >80% similarity. MMW, male medical ward; ICU, intensive care unit; URO, urology; FMW, female medical ward; CCU, coronary care unit; MSW, male surgical ward; PFGE, pulsed field gel electrophoresis.
Molecular fingerprinting grouped the 10 NDM-1 producer and the 3 NDM-1 and OXA-48-like producer isolates into three clusters (Fig. 1 and Table 1). The largest cluster (A) contained isolates carrying the blaNDM-1 gene mostly on plasmids of 170 kb (Fig. 1 and Table 1). In the other two clusters, isolates, although their plasmid profiles were not always identical, carried the blaNDM-1 on plasmids of the same size (i.e., 140 and 170 kb, respectively). Strains carrying both NDM-1 and OXA-48-like genes grouped together in cluster C with isolate No. 11 which was only positive for blaNDM-1.
Discussion
In this retrospective study, conducted over a year period, we established that 7% of K. pneumoniae strains isolated in our hospital were carbapenem-resistant among hospitalized patients. It was noteworthy, that 13 of the 14 CRKP isolates (and all which retained its CR phenotype all through the study) were carrying the blaNDM-1 gene. As originally identified as being resistant to meropenem, we surmise that the strain negative for all the carbapenemase genes but susceptible at the time of PCR might have lost its beta-lactamase-coding plasmid during storage. Theoretically, in this strain we cannot exclude an enzyme-independent resistance mechanisms (e.g., the loss of porins), but the resistance at the time of isolations and the subsequent full susceptibility favours the first possibility. Nevertheless, all attempts to recover a nonsusceptible form of strain No. 6 failed.
Interestingly, 3 of the 13 NDM-1 positive strains were additionally carrying the blaOXA-48-like gene, as well. The carriage of more than one carbapenemase genes, although not common, is a well known phenomenon and has already been reported from the region. 5 An important finding of the study was that no blaKPC carrying organism was detected. Although these strains are of serious concerns globally, to the best of our knowledge they have not been encountered in the Arabian Peninsula.
This is the first study reporting NDM-1 producing isolates from Sharjah Emirate of the UAE. Earlier observation from Abu Dhabi reported that a plasmid of ∼50 kb size, belonging to the incX3 incompatibility group, was carrying the blaNDM-1 gene in several Enterobacteriaceae, albeit not K. pneumoniae, isolates. 18 Similar size plasmids carrying blaNDM-1 were not encountered in our hospital, with the majority of isolates carrying the blaNDM-1 on much larger, ∼170 kb, plasmids. In one isolate, the NDM probe hybridized with two plasmids, a phenomenon also reported earlier by Kumarasamy and colleagues. 11 Further characterization of these plasmids was beyond the scope of this present study.
The high incidence of NDM-1 producer K. pneumoniae in the study period was not attributed to the spread of a single clone, as three clusters of strains could clearly be identified by PFGE. It was also interesting to note that, with the exception of isolates No.1 and 12, all CRKP with similar pulsotype were isolated from different wards of the hospital. While both strains No.1 and 12 were from Male Medical Ward, they were isolated 11 months apart. These observations suggest the possibility of multiple introductions of CRKP strains into our hospital, or, alternatively, an extended presence with occasional inter-ward transfers.
There are several potential limitations of the study. We targeted five key carbapenemase resistance genes, only, that is, IMP, VIM, OXA, KPC, and NDM. Although these genes are recognized as major resistance determinants, 17 several other, rare carbapenemase genes found in Klebsiella peumoniae, were not looked for by our study. While all the 202 isolates were from patients with active signs and symptoms of the disease present in them, a majority of the strains (73%) were obtained from urine and respiratory secretions, especially in ICU patients which can create some uncertainties in distinguishing critical colonization and infection. Furthermore, this is a retrospective, single hospital based study and does not allow us to draw a conclusion on the prevalence of NDM-1 positive CRKP in the UAE. Nevertheless, previous reports18,19 suggest that other Emirates of the UAE may face similar problems.
In conclusion, detection of NDM-1 positive CRKP strains in our hospital, particularly in patients with no travel history, clearly supports the earlier suggestion that the Middle East serves as a secondary reservoir for carbapenemase producer Enterobacteriaceae5,8,9,13,14,16,18,19 and highlights the need for action to prevent the emergence and interrupt the spread of these strains in the hospitals of the UAE.
Footnotes
Acknowledgments
We are thankful to the staff members of the A Qassimi hospital, Sharjah for providing us the K. pneumoniae isolates. The control strains GR-KPC2, KP No. 16, and OEK-IMP were kindly provided by P. Nordmann, L. Poirel (Paris, France) and by Á. Toth (Budapest, Hungary). This work was partly supported by a UAEU-NRF grant to A.S. (31M085).
Disclosure Statement
The authors have no competing interests to disclose. Ethical approval was obtained for this study from the Research Ethics Committee of the Al Qassimi Hospital (REC-02012-03).