
Abstract
A total of 1,870 nonduplicate clinical Enterobacteriaceae from 13 teaching hospitals located in 11 provinces of mainland China from 2011 to 2012 were screened for the presence of the blaNDM gene. The high-throughput MiSeq sequencing method and comparative genomics were used to analyze the genetic environment of blaNDM among these isolates. Three blaNDM-1-carrying Klebsiella pneumoniae (0.16%, 3/1,870), isolated from a teaching hospital in Xi'an, exhibited high levels of resistance to all β-lactams, but remained susceptible to amikacin, tigecycline, and polymyxin B. These three isolates, belonging to ST147, presented an identical pulsed-field gel electrophoresis pattern. The IncX3 plasmid, pNDM-SX04 (KC876051) showed 99% identity with plasmid pNDM-HN380 (JX104760). Comparative analysis of the genetic environment of blaNDM-1 with previously published plasmids revealed the same 7,830-bp basic mobile element, which may have been derived from Acinetobacter spp. Partial ISAba125, ISAba125 promoter, blaNDM-1, and bleMBL could serve as the minimal mobile vehicle facilitating horizontal transfer of the blaNDM-1 gene. To our knowledge, this is the first report of an outbreak of blaNDM-1-carrying ST147 K. pneumoniae. Although the prevalence spread by the blaNDM-1 gene prevalence is at a low frequency in mainland China, a dynamic national surveillance of this gene is needed due to its potential transferability.
Introduction
NDM
In this study, we isolated three blaNDM-positive Klebsiella pneumoniae isolates and found that they belonged to the same clone ST147, which has not yet been reported in China. Furthermore, this study is the first to report on an outbreak of ST147 NDM-1-producing K. pneumoniae.
Materials and Methods
Bacterial strains and antimicrobial susceptibility testing
A total of 1,870 nonrepetitive clinical Enterobacteriaceae isolates collected through two national surveillance programs conducted from May to November 2011 for Chinese Antimicrobial Resistance Surveillance of Nosocomial Infections (CARES) and from January to August 2012 for Chinese Meropenem Susceptibility Surveillance (CMSS) (from 13 teaching hospitals located in 11 provinces of China) were sent to the central laboratory for a retrospective study. All these isolates were obtained from the south, north, northwest, east, and middle districts of China.
The VITEK GNI system (bioMerieux Vitek, Inc., Hazelwood, MO) was used for bacterial identification. The minimum inhibitory concentrations (MICs) were determined by using the microdilution method recommended by the Clinical and Laboratory Standards Institute. 4 The breakpoint of tigecycline for Enterobacteriaceae was in accordance with the FDA standard. Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as controls for antimicrobial susceptibility testing.
Phenotypic and molecular detection of blaNDM-1
For carbapenem nonsusceptible (CNS) Enterobacteriaceae isolates (imipenem/meropenem MIC ≥2 mg/L or ertapenem MIC ≥1 mg/L), the modified Hodge test and the imipenem-EDTA double-disc synergy test were used to detect carbapenemases production. Polymerase chain reaction (PCR) analysis was performed for carbapenemase genes (blaNDM, blaIMP, blaVIM, blaKPC, and blaOXA-48), other β-lactamase genes (blaTEM, blaSHV, blaCTX-M, blaAmpC, blaDHA, and blaCMY), as well as quinolone resistance determinants (qnrA, qnrB, qnrS, and aac(6′)-Ib), according to previous studies.3,13 All the PCR products were sequenced with an ABI7570 (Applied Biosystems, Foster City, CA).
Multilocus sequence typing and pulsed-field gel electrophoresis
For the blaNDM-positive strains, multilocus sequence typing (MLST) primers for K. pneumoniae and sequences of the seven housekeeping genes were referred to those in the Pasteur Institute MLST database (www.pasteur.fr/recherche/genopole/PF8/mlst/Kpneumoniae.html). The chromosomal DNA of the three K. pneumoniae isolates was prepared in agarose blocks and digested with the restriction enzyme XbaI. The DNA fragments were separated using the CHEF-DR-III apparatus (Bio-Rad, Hercules, CA) for 22 hr at 6 V/cm and 14°C with the initial and final pulse times of 0.5 and 30 sec, respectively. The DNA macrorestriction patterns were analyzed by visual inspection, according to the criteria of relatedness proposed by Tenover et al. 14
Conjugation
The transferability of the blaNDM gene was tested by using a broth culture conjugation method with NDM producers as the donors and azide-resistant E. coli J53 as the recipient. The donor and recipient cells were mixed at a ratio of 1:1. Transconjugants were selected on Chinese Blue lactose agar supplemented with sodium azide (100 mg/L) and imipenem (0.5 mg/L). The absence of growth of the parent cells and the recipients in the selective agar plate was confirmed, and the transconjugants were identified and confirmed to be blaNDM-1-positive by PCR analysis.
Plasmid sequencing and comparative genomics
The plasmid DNAs of the parent cells and transconjugants were extracted with the QIAGEN Midi Kit (Qiagen, Hilden, Germany), according to the manufacturer's protocol. Replicon typing was applied for the identification of the Inc plasmid subtypes. 9 The plasmid restriction fingerprints of three transconjugants harboring blaNDM-1 were further analyzed with restriction enzymes EcoRI and PstI (Takara, Dalian, China) according to the manufacturer's instruction.
The plasmid DNA of NDM-producing K. pneumoniae isolates Kpn-SX04 was performed using MiSeq Illumina platforms (Illumina, Inc., San Diego, CA) for paired-end 150 bp sequencing. The procedures for functional annotation were performed as described previously. 2 The plasmid sequences were assembled by the Soap denovo software, version 1.06, and each predicted protein was further compared with the NCBI nonredundant protein database using BLASTP. 11 The genetic contexts of blaNDM located on plasmid pNDM-SX04 were compared with the published Enterobacteriaceae plasmids and Acinetobacter spp. plasmids isolated in China and around the world.
Plasmid nucleotide sequence accession numbers
The partial sequence (13,508 bp) of plasmid pNDM-SX04 has been deposited in the GenBank database, and the plasmid gene accession number is KC876051.
Results
Antimicrobial susceptibility testing and detection of resistance genes
A total of 74 isolates were CNS Enterobacteriaceae isolates, including 62 K. pneumoniae, 5 Enterobacter cloacae, 2 E. coli, 3 Citrobacter freundii, 1 Enterobacter aerogens, and 1 Serratia marcescens. Among these isolates, 43 blaKPC-2-producing K. pneumoniae, 2 blaKPC-2 and blaIMP-1 double-positive C. freundii, 4 blaIMP-4-producing K. pneumoniae, and 2 blaIMP-4-producing E. cloacae were identified. Only three blaNDM-1-positive K. pneumoniae isolates were confirmed.
The blaNDM-1 (813 bp, GenBank accession no. KC537739), blaSHV-12, and aac(6′)-Ib-cr genes were confirmed coexists in the three K. pneumoniae isolates. In addition, Kpn-SX04 was found to coharbor blaTEM-1, and Kpn-SX02 was noted to carry blaTEM-1 and blaCTX-M-3 (Table 1). Other resistance genes were not detected. All the three K. pneumoniae isolates (designated as Kpn-SX02, Kpn-SX03, and Kpn-SX04), isolated from sputum samples, exhibited high levels of resistance to cephalosporins (ceftriaxone, ceftazidime, cefepime), carbapenems (imipenem, meropenem), β-lactam/β-lactamase inhibitor combinations (piperacillin/tazobactam), monobactams (aztreonam), and quinolones (ciprofloxacin, levofloxacin), but remained susceptible to amikacin, tigecycline, and polymyxin B (Table 1).
For conjugational assay, the donors were Kpn-SX02, Kpn-SX03, and Kpn-SX04, and the recipient was E. coli J53 Azr. The corresponding transconjugants were Kpn-SX02-T, Kpn-SX03-T, and Kpn-SX04-T, respectively.
The breakpoint of tigecycline for Enterobacteriaceae was referred to the FDA standard.
IPM, imipenem; MEM, meropenem; CRO, ceftriaxone; CAZ, ceftazidime; FEP, cefepime; TZP, piperacillin-tazobactam; ATM, aztreonam; AMK, amikacin; CIP, ciprofloxacin; LVX, levofloxacin; TGC, tigecycline; PB, polymyxin B; SXT, sulfamethoxazole.
The clinical information of three patients infected with blaNDM-1-carrying K. pneumoniae
Three patients with no recent history of traveling to endemic regions or receiving any healthcare abroad were admitted with cerebral infarction. They developed ventilator-associated pneumonia (VAP) from April to June 2012 at one teaching hospital in Xi'an, Shanxi province, China. Patients SX02 and SX03 were in the same department, but not in the same room. Patient SX03, a 91-year-old man, had received healthcare in the geriatrics department several times. Patient SX02, an 84-year-old man, died owing to complications of respiratory failure and septic shock. Before isolation of carbapenem-resistant K. pneumoniae (CRKP), all the patients were administrated with meropenem and a series of other broad-spectrum antibiotics. The detailed patient profiles are summarized in Figure 1.
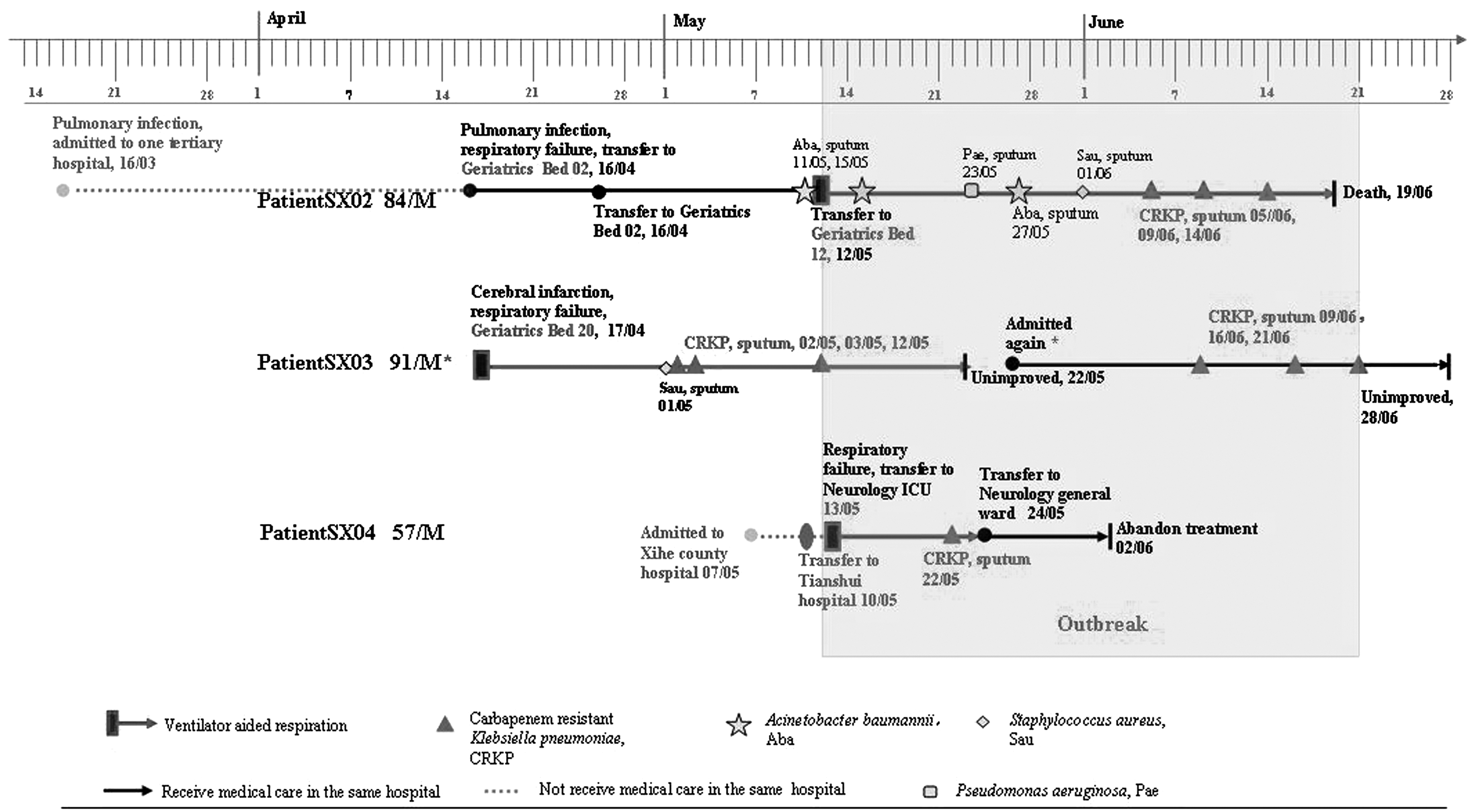
Timelines on the event of an outbreak of NDM-1-producing Klebsiella pneumoniae at a teaching hospital in Xi'an, China, in 2012. *Patient SX03 was discharged home on May 22, 2012, with unimproved condition and again hospitalized in the geriatrics department several days later. Because of hypertension, coronary atherosclerosis, and diabetes mellitus, he had been repeatedly receiving healthcare in the same hospital and in the same department in the past, and no organism producing blaNDM-1 gene had been detected until May 2, 2012.
Patient SX02, who died owing to complications of respiratory failure and septic shock, had been transferred from a second senior hospital with cerebral infarction and hospital-acquired severe pneumonia to the geriatrics department on 16 April 2012. He had been receiving antibiotic combination treatment comprising meropenem and linezolid. As A. baumannii had been isolated several times from the patient's sputum, imipenem/cilastatin, piperacillin/tazobactam, and minocycline were administrated. On 12 May 2012, he had received mechanical ventilation because of shock. CRKP had been isolated from the sputum on 5 June 2012, and imipenem/cilastatin and sulfamethoxazole were used to treat severe pneumonia. Finally, the patient SX02 died as a result of multiple organ dysfunction and disseminated intravascular coagulation.
The resident patient SX03, was hospitalized in the same department where patient SX02 was admitted, but not in the same room, on 15 March 2012 with large area cerebral infarction on the left side. The patient ultimately developed late-onset hospital-acquired pneumonia and respiratory failure. Because of hypertension, coronary atherosclerosis, and diabetes mellitus, patient SX03 had been repetitively receiving healthcare in the same hospital and in the same department in the past. During this hospitalization, he had been receiving mechanical ventilation because of cerebral infarction, and developed VAP. Methicillin-resistant Staphylococcus aureus and CRKP had been isolated from his sputum several times during this hospitalization, and hitherto, he had received antibiotic combination treatment comprising cefoperazone/sulbactam and linezolid. After the first CRKP had been identified on 2 May 2012, the patient was treated with meropenem, antiendotoxin, and other expectant treatment. He was discharged on 22 May 2012 with unimproved condition, and was again hospitalized in the geriatrics department several days later. CRKP was isolated from his sputum on 9, 16, and 21 June 2012, respectively. Later, on 28 June 2012, the patient was discharged with unimproved condition and no NDM-1 producing CRKP was detected subsequently.
Patient SX04 was a 57-year-old man admitted to the neurology intensive care unit department with respiratory failure, cerebral infarction, and hypertension (very high risk group). He was under mechanical ventilation for 12 days. CRKP isolated from his sputum samples on 22 May 2012 was resistant to all β-lactams and quinolones, but susceptible to amikacin. Subsequently, the patient was administered with meropenem and ceftriaxone/tazobactam. On 25 May 2012, he was transferred to the neurological general ward, and on 2 June 2012, further treatment was stopped with unimproved symptoms.
Molecular typing and plasmid characterization
Both pulsed-field gel electrophoresis (PFGE) and MLST data showed that the three K. pneumoniae isolates belonged to ST147 and had an identical PFGE pattern (Fig. 2). In conjugation experiments, the IncX3 plasmid of ∼54 kb, coharboring blaNDM-1 and blaSHV-12 from the donors, was transferred successfully into E. coli J53 at frequencies of 1.33×10−6, 4.04×10−7, and 6.94×10−7 transconjugants per recipient cell, respectively. All three transconjugants displayed no other resistance marker besides blaNDM-1 and blaSHV-12 genes. The three plasmids from the transconjugants showed identical patterns after EcoRI and PtsI digestion. The MICs of the antimicrobial agents tested against the transconjugants and recipients are shown in Table 1.
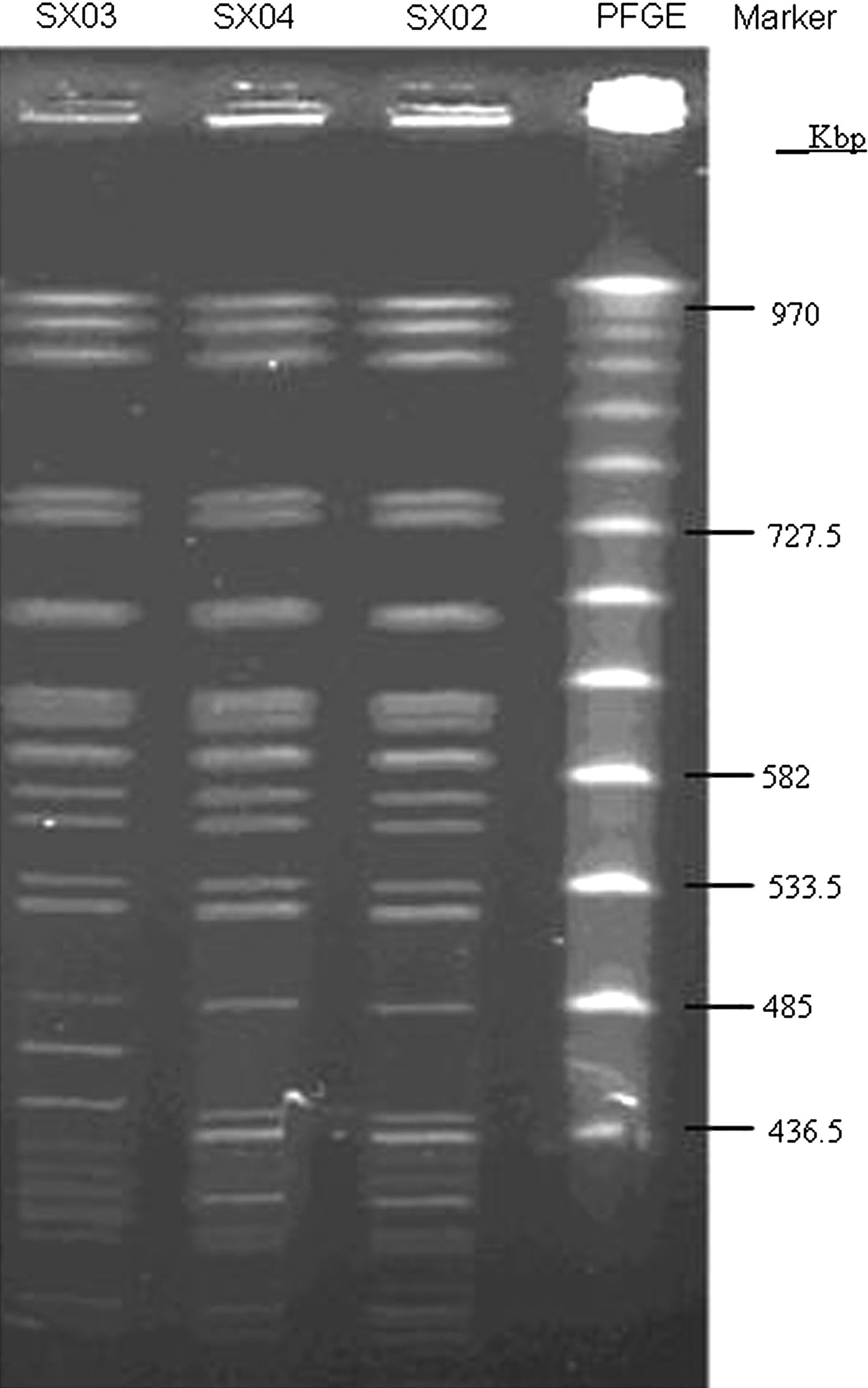
Pulsed-field gel electrophoresis (PFGE) of XbaI-digested DNA of K. pneumoniae isolates. PFGE marker, Lambda ladder PFG marker (NEB).
Sequence analysis of plasmid pNDM-SX04
The 54-kb sequenced plasmid pNDM-SX04, containing blaNDM-1 and blaSHV-12, shared 99% identity with the published pNDM-HN380. 8 The partial sequence (13,508 bp), including the blaNDM-1 gene of pNDM-SX04, shared 100% identity with plasmids pFR90 (JQ362415, Proteus rettgeri, 17,691 bp) and pYE315203 (JX254913, C. freundii, 14,425 bp), which were also isolated in mainland China.
Comparative analysis of the genetic environment of blaNDM-1 of Enterobacteriaceae isolated in China and around the world revealed a mobile element with a length of 7,830 bp (including ΔISAba125, promoter, blaNDM-1, bleMBL, trpF, dsbC, cutA1, groES, groEL, and insE), which facilitated horizontal mobilization of the blaNDM-1 gene (Fig. 3). At the head of ISAba125 and at the tail of the mobile element, the sequence could be truncated at arbitrary length and the remaining minimal mobile element contained only the partial ISAba125, ISAba125 promoter, blaNDM-1, and bleMBL. On comparing the genetic environment of blaNDM-1 of Acinetobacter spp. with that of Enterobacteriaceae, it was observed that only Acinetobacter. spp. had the complete ISAba125 transposon with a length of 10,038 bp, comprising two copies of complete full-length ISAba125 (1,026 bp) at each side.
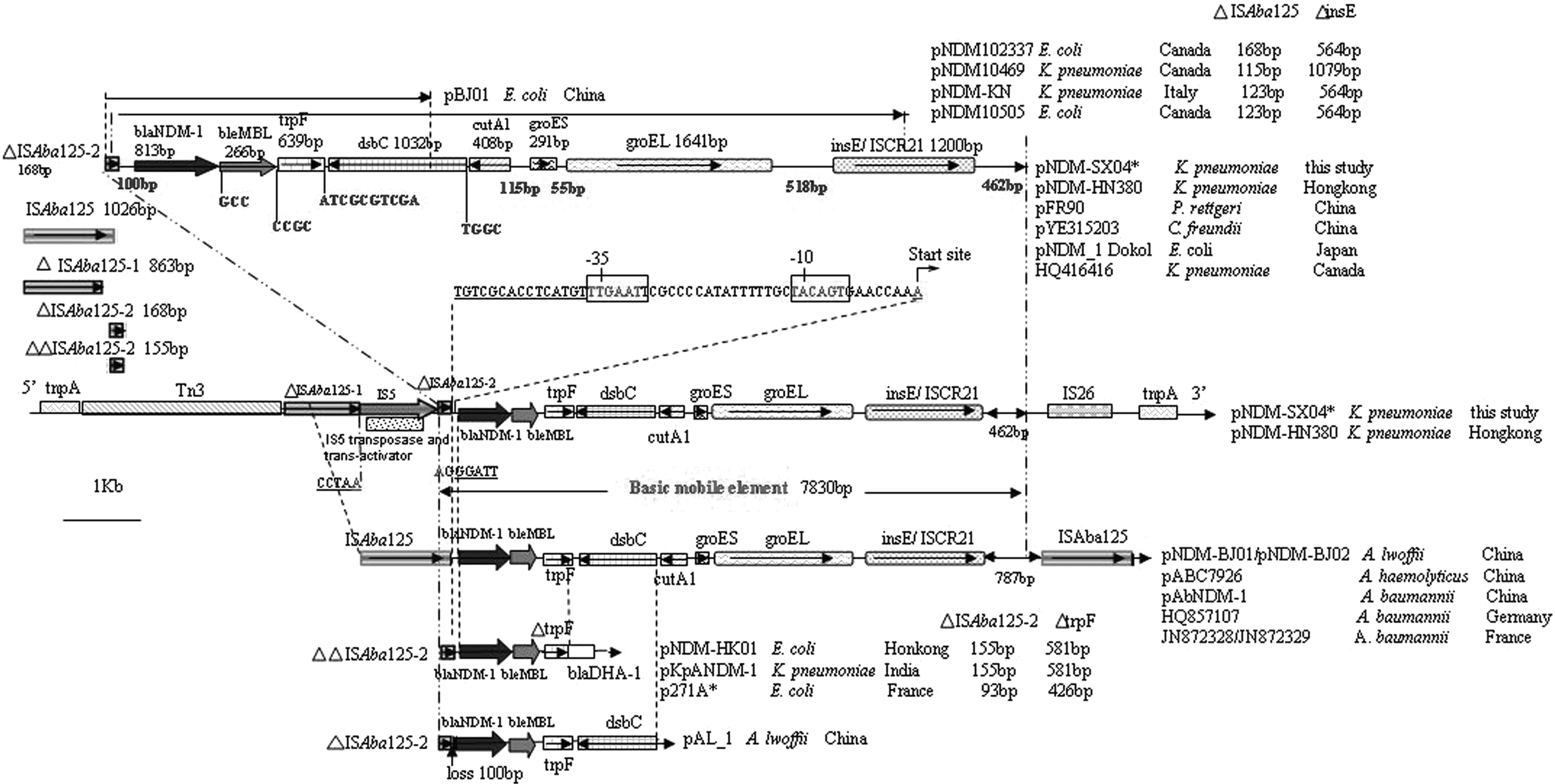
Comparative genetic environment of blaNDM-1 in Enterobacteriaceae and Acinetobacter spp. The accession numbers of Enterobacteriaceae strain origin plasmids isolated in China are as follows: pNDM-HN380 (JX104760, K. pneumoniae), pFR90 (JQ362415, Providencia rettgeri), pYE315203 (JX254913, Citrobacter freundii), and pNDM-HK01 (HQ45451074, Escherichia coli); and those isolated around the world are as follows: pNDM-1 Dokol (AP012208, K. pneumoniae, Japan), pNDM10469 (JN861072, K. pneumoniae, Canada), K. pneumoniae strain GN529 plasmid (HQ416416, K. pneumoniae, Canada), pNDM102337 (JF714412, K. pneumoniae, Canada), pNDM10505 (JF503991, K. pneumoniae, Canada), pNDM-KN (JN157804, K. pneumoniae, Italy), KpANDM-1 (FN396876, K. pneumoniae, India), and p271A (JF785549, E. coli, France). The accession numbers of Acinetobacter spp. origin plasmids isolated in China are as follows: pNDM-BJ01/pNDM-BJ02 (JQ0017091 and JQ060896, Acinetobacter lwoffii), pABC7926 (JQ080305, Acinetobacter haemolyticus), pAbNDM-1 (JN377410, Acinetobacter baumannii), and pAL-1 (JN616388 A. lwoffii, isolated from chicken); and those isolated around the world are as follows: HQ857107 (A. baumannii, Germany) and JN872328/JN872329 (A. baumannii, France).
Discussion
Carbapenems are the last resort available for the treatment of severe nosocomial or community-acquired infections caused by multiresistant AmpC- or extended spectrum-β-lactamase-producing Enterobacteriaceae. 12 To date, there have been only a few reports on large-scale surveillance of the prevalence of NDM among Enterobacteriaceae in China, or surveillances have just been limited to Acinetobacter spp. The present study is the first organized multicenter investigation to report the prevalence of NDM-1 among 1,870 non-reduplicated Enterobacteriaceae isolates. Although the spread of the bla NDM-1 gene prevalence is at a low frequency of 0.16% (3/1,870) in mainland China, when compared with that of blaKPC-2 gene prevalence (2.4%, 45/1,870 Enterobacteriaceae; 60.8%, 45/74 CNS), it definitely acts as a warning to an emerging problem that has the potential to spread.
This study is the first to describe a nosocomial clonal outbreak of NDM-1-producing K. pneumoniae ST147 in China. The three bla NDM-1 -positive K. pneumonia isolates with an identical PFGE pattern also belonged to the same clone ST147. Furthermore, these three isolates also carried the same IncX3 plasmids harboring similar genetic antibiotic determinants (bla NDM-1 and bla SHV-12 ). Moreover, clinical data of all the three patients exhibited epidemiological links with each other, such as receiving mechanical ventilation during an overlapped period of hospitalization and isolation of the same clone of NDM-1-producing CRKP from patient SX02 after transferring to geriatrics Bed 12, which was close to the bed of patient SX03. To the best of our knowledge, although there have been a few reports of blaNDM-1-carrying Enterobacteriaceae in china, epidemiological relatedness among Enterobacteriaceae in China is relatively less. Reports about the sequence type of outbreak or nosocomial dissemination of NDM-1-producing K. pneumoniae around the world have involved ST2311 and ST340, 10 and the present study is the first to report on an outbreak of NDM-producing K. pneumoniae ST147. The role of mechanical ventilators as one of the vehicles spreading NDM-1-producing K. pneumoniae and use of large doses of broad-spectrum antibiotics cannot be ruled out as possible risk factors. Hence, potential clonal dissemination of the bla NDM-1 gene promptly needs to be monitored in the future not only among patients under mechanical ventilator, but also in the environments.
Possessing its own promoter for controlling replication, the horizontal transfer of the InX3 plasmid carrying the blaNDM-1 gene into the recipient E. coli J53 proved the prior capability of this plasmid for in vitro dissemination reported earlier. Comparative analysis of the genetic environment of blaNDM-1 with previously published plasmids isolated from Enterobacteriaceae 8 and Acinetobacter spp.2,6 revealed that the mobile element with a length of 7,830 bp harboring the blaNDM-1 gene in Enterobacteriaceae may have been derived from that of Acinetobacter spp., which possesses a complete ISAba125 transposon element with two copies of complete full-length ISAba125 (1,026 bp) at each side. Partial ISAba125, ISAba125 promoter, blaNDM-1, and bleMBL might serve as the minimal mobile vehicle facilitating horizontal transfer of the blaNDM-1 gene intra- or interspecies among Enterobacteriaceae and other genera.
The limitation of this study is its retrospective nature, and we were unable to acquire sufficient data to determine the origin of the blaNDM-1-producing bacteria in the hospital examined and check the nosocomial environment promptly. Nevertheless, it is necessary to monitor clonal dissemination of ST147 or other sequence type of blaNDM-1-producing K. pneumoniae as well as the IncX3 plasmids carrying blaNDM-1 and blaSHV-12 (determined in the present study and in the study carried out in Hong Kong, respectively) in the future.
Footnotes
Acknowledgments
We thank Wenqiang He, Henan Li, Zhanwei Wang, and Feifei Zhang of Peking University People's Hospital for their encouragement and guidance in the experiments conducted. We thank Yingmei Liu of Beijing Chaoyang Hospital for the assistance in the PFGE. This work was financially supported by the Beijing Natural Science Foundation (grant no. 5122041), Research Found for the Doctoral Program of Higher Education of China (RFDP, grant no. 20110001110043), Beijing City Board of Education Science and technology key project (grant no. KZ201210025025), and Trans-Century Training Programme Foundation for the Talents by the State Education Commission (grant no. NCET-10-0205).
Disclosure Statement
No competing financial interests exist.