
Abstract
The rate of fluoroquinolone (FQ) resistance among the cephalosporin-resistant Klebsiella pneumoniae is considerably high, however, their genetic profiles have not been well investigated. We selected 61 ciprofloxacin-nonsusceptible isolates from 102 K. pneumoniae isolates judged to be “resistant” to some cephalosporins during 2009 and 2012 throughout Japan. Pulsed-field gel electrophoresis excluded clonal isolates, and 29 isolates were subjected to multilocus sequence typing (MLST), detection of the amino acid substitutions in the quinolone resistance determining regions (QRDRs) of GyrA and ParC, β-lactamase typing, and identification of plasmid-mediated quinolone resistance (PMQR) genes. PCR-based replicon typing was performed, after PMQR gene transfer. Four major sequence types (STs) or clonal complexes (CCs), that is, ST37, CC17 (consisting of ST17 and ST20), ST11, and CC528 (consisting of ST528 and ST1130), were found, and they accounted for 48.2% of the isolates tested. Amino acid substitutions in the QRDRs and the presence of PMQR genes were identified in 20 (68.9%) and 18 (62.0%) isolates, respectively. The replicon type of three PMQR-carrying plasmids was IncN, but others were nontypable. Fifteen (83.3%) of the 18 PMQR-harboring isolates coharbored blaCTX-M and/or blaDHA-1. Ciprofloxacin-nonsusceptible K. pneumoniae clinical isolates demonstrating cephalosporin resistance often belong to the global epidemic lineages and possess PMQR and/or QRDR substitutions.
Introduction
N
Klebsiella pneumoniae is one of the most important pathogens causing nosocomial and community-acquired infections and considered as the usual bacterial species of extended spectrum beta-lactamase (ESBL) producers among the family Enterobacteriaceae. Moreover, the strains producing carbapenemases such as KPC, NDM, and OXA-48 have so far been found mainly from K. pneumoniae isolated worldwide, including European, American, and Asian countries. Those carbapenemase-producing isolates usually demonstrate FQ resistance 22 through acquisition of amino acid substitutions in QRDRs and enhanced function of efflux systems. 1 Thus, the spread of multidrug-resistant K. pneumoniae is becoming an ongoing global threat to public health. Fortunately, the rate of FQ resistance among K. pneumoniae clinical isolates overall is still low at present in Japan. According to the report published in 2012 by the Japan Nosocomial Infections Surveillance (JANIS), the rate of levofloxacin-nonsusceptible isolates in K. pneumoniae was 2.4%, which was much lower than that (above 34%) in E. coli (www.nih-janis.jp/report/kensa.html) on the basis of the CLSI's breakpoints at 2007 (M100-S17). However, increased isolation of FQ-resistant K. pneumoniae has been accompanied with the increase of carbapenemase-producing K. pneumoniae worldwide, including the European countries and the United States. Multilocus sequence typing (MLST), an analysis of nucleotide sequence-based methods adequate for characterizing the genetic relationships of bacterial isolates in a broad perspective has become popular and has revealed that specific STs have some relationships with specific resistance genes, for example, E. coli ST131 with blaCTX-M and K. pneumoniae ST258 with blaKPC-2.12,35 Thus, we speculated that the clonal spreads of some K. pneumoniae clinical isolates belonging to specific genetic lineages may well contribute to the prevalence of FQ resistance among the cephalosporin-resistant K. pneumoniae, because FQ resistance was more frequently found among cephalosporin-resistant K. pneumoniae than among cephalosporin-susceptible ones. Therefore, we studied the genetic profiles of ciprofloxacin-nonsusceptible isolates among the cephalosporin-resistant K. pneumoniae clinical isolates from 24 different hospitals located in 11 different prefectures in Japan.
Materials and Methods
Preliminary study
Before we investigated the genetic lineages of FQ-resistant K. pneumoniae to exclude clonal spread among K. pneumoniae in Japan, we chose 22 of the 176 K. pneumoniae isolates susceptible to both FQs and cephalosporins recovered from separate regions in Japan and investigated their STs. As a result, no apparent ST clusters were found among them.
Bacterial isolates
Among 16,526 clinical K. pneumoniae isolates sent to a private microbiology laboratory from 2009 to 2012, we collected 102 K. pneumoniae isolates from 24 separate hospitals located in 11 prefectures of Japan, which were first judged as “resistant” to cefotaxime, ceftazidime, cefozopran, cefepime, and/or cefpirome by the MicroScan WalkAway system (Siemens Healthcare Diagnostics, Inc.) in a private microbiology laboratory. Of the 102 isolates, 61 were selected because minimum inhibitory concentrations (MICs) of ciprofloxacin and/or levofloxacin were above the breakpoint of intermediate by the agar dilution method recommended by the CLSI (M100-S20). 15 For the multiple isolates recovered from the same hospital, pulsed-field gel electrophoresis (PFGE) was performed to exclude repetitious isolations of the same clone. Consequently, 29 ciprofloxacin-nonsusceptible K. pneumoniae clinical isolates were selected and subjected to this study.
Antimicrobial susceptibility
The antimicrobial susceptibility test was performed by the agar dilution method according to the protocol recommended by the CLSI (M07-A8) 14 for the following antimicrobial agents obtained from the indicated sources: cefotaxime (CTX), imipenem (IPM), amikacin (AMK), gentamicin (GEN), ciprofloxacin (CIP), colistin (CST), fosfomycin (FOF), Wako Pure Chemical Industries, Ltd.; ceftazidime (CAZ), levofloxacin (LVX) Tokyo Chemical Industry Co. Ltd.; cefepime (FEP), Santa Cruz Biotechnology, Inc.; cefminox (CMNX), Meiji Seika Pharma Co., Ltd.; and tigecycline (TGC), Pfizer Japan, Inc. Glucose-6-phosphatase (25 mg/L) (Sigma-Aldrich Co. LLC.) was added to the media for the susceptibility test against FOF.
Multilocus sequence typing
MLST was performed on the 29 isolates using the protocol for K. pneumoniae provided by the Institute Pasteur website (www.pasteur.fr/recherche/genopole/PF8/mlst/Kpneumoniae.html). New alleles and STs were submitted to the MLST website and new ST numbers were assigned. In the present study, clonal complex (CC) was defined as the group of STs that are related to each other by a single locus variant (SLV) level.
Screening of genes for β-lactamase and PMQR
PCR was performed on 29 isolates to detect the following genes: blaTEM, blaSHV, 36 blaCTX-M-1 group, blaCTX-M-2 group, blaCTX-M-9 group, 29 blaACC, 25 blaFOX, blaMOX, blaDHA, blaCIT, blaEBC, 27 qnrA, qnrB, qnrS, 6 qnrC, 34 qnrD, 7 qepA, 37 and aac-(6′)-Ib genes with the primers previously described. The obtained PCR amplicons of blaTEM/blaSHV and aac-(6′)-Ib genes were further subjected to nucleotide sequencing to determine whether or not they encode ESBLs and aac-(6′)-Ib-cr, respectively, and blaCTX-M genes were also sequenced with the appropriate primers.8,30
Analysis of alterations in QRDRs
The amino acid substitutions in QRDRs of GyrA and ParC were deduced by nucleotide sequencing of gyrA and parC genes with the primers described previously.4,24 The nucleotide mutations were identified based on the available nucleotide sequences of gyrA and parC of K. pneumoniae ATCC 13833.
Transfer of quinolone resistance genes and PCR-based replicon typing
The broth-mating conjugation experiment was carried out with E. coli J53 as the recipient strain, and transconjugants were selected on the Luria-Bertani (LB) agar plates containing sodium azide (150 mg/L) and ciprofloxacin (0.05 mg/L). In the isolates from which no transconjugant was obtained by the above-described conjugation procedure, transformation with purified plasmids was performed. The plasmid DNA was extracted by the method of Kado and Lui. 18 E. coli DH10B was used as the recipient strain, and transformants were selected on the plates containing ciprofloxacin (0.05 mg/L). For the isolates from which no transconjugants or transformants were obtained despite repeated attempts using LB agar plates containing ciprofloxacin as described above, we performed an alternative method to obtain transconjugants and/or transformants, depending on the fact that both PMQR genes and ESBL genes are frequently cocarried by the same plasmid. For this purpose, ampicillin-resistant transconjugants and/or transformants were first selected by the agar plates supplemented with ampicillin (100 mg/L). We also used E. coli CSH2 and J53 for the recipient in a conjugation experiment using an agar plate supplemented with rifampicin (150 mg/L) and ampicillin (100 mg/L). The presence of ESBL and PMQR genes was checked by PCR on several colonies grown on each plate, and then it was confirmed by nucleotide sequencing whether or not the objective genes were transferred. PCR-based replicon typing (PBRT) was performed on the obtained transconjugants and/or transformants. 5
Results
Bacterial isolates
First, we tried to collect quinolone-resistant K. pneumoniae, although they are still rare in Japan at present. Then, we screened quinolone-resistant K. pneumoniae isolates among the K. pneumoniae, which acquired resistance to cephalosporins, because the rate of quinolone resistance tended to be high among the cephalosporin-resistant K. pneumoniae isolates. Isolate Nos. 40, 53, and 56 were susceptible to cefotaxime and ceftazidime by the agar dilution method, even though they were first judged as resistant to cefotaxime, ceftazidime, cefozopran, cefepime, and/or cefpirome by the MicroScan WalkAway system. The 61 ciprofloxacin-nonsusceptible isolates selected were recovered from January 5, 2009, to October 3, 2012, from 24 hospitals located in 11 prefectures in Japan. Four, 2, and 2 isolates demonstrating different PFGE profiles from each other were recovered from hospitals S-1, A-1, and TK-3, respectively. In seven hospitals, more than two isolates belonging to the same clonal lineage in each hospital were found by PFGE. The isolates recovered from the seven hospitals belonged to separate sequence types (STs) (Table 1). Interestingly, 22 isolates belonging to the same clonal lineage were recovered from one hospital (hospital I-1), suggesting a probable nosocomial outbreak of FQ-resistant K. pneumoniae in hospital I-1. We selected a single isolate from the multiple isolates in these seven hospitals for further investigation.
A single isolate was recovered in remaining 16 hospitals.
PFGE, pulsed-field gel electrophoresis; ST, sequence type.
Antimicrobial susceptibility
The range of ciprofloxacin MICs for each isolate varied. The fourth-generation cephalosporin and cefepime showed relatively low MICs for the isolates compared with the MICs of cefotaxime and ceftazidime, although some isolates demonstrated intermediate or resistant profiles against cefepime. Most isolates were susceptible to imipenem, however, in some isolates, such as isolates 1 and 3, intermediate or resistant profiles to imipenem (MICs, 2–4 mg/L) were found. This was due to the harboring of blaIMP or blaNDM in the isolates 1 and 3, respectively, as detected later by PCR. A high MIC of fosfomycin (>256 mg/L) was found for two isolates. The MIC of tigecycline was >16 mg/L for three isolates. Colistin, which has not yet been approved for clinical use in Japan, seemed very effective for all isolates (Table 2).
Isolate no. is listed by the order as shown in Table 3.
MIC ranges measured: CTX, CAZ, FEP, CMNX, IPM, AMK, GEN, and FOF; 0.125 through 256, CIP and LVX; 1 through 128, CST; 0.016 through 8, TGC; 0.016 through 16.
MIC breakpoints for Enterobacteriaceae suggested by CLSI M100-S20, 2010 (S, I, R): CTX; (≤1, 2, ≥4), CAZ; (≤4, 8, ≥16), FEP; (≤8, 16, ≥32), IPM; (≤4, 8, ≥16), GEN; (≤4, 8, ≥16), AMK; (≤16, 32, ≥64), CIP; (≤1, 2, ≥4), LVX; (≤2, 4, ≥8).
Etest was performed for the isolates for which high TGC MICs (≥16 mg/L) were found by the CLSI agar dilution method.
Genes for NDM-1 and IMP-1 were detected by PCR in isolate numbers 1 and 3, respectively.
CTX, cefotaxime; CAZ, ceftazidime; FEP, cefepime; CMNX, cefminox; IPM, imipenem; AMK, amikacin; GEN, gentamicin; CIP, ciprofloxacin; LVX, levofloxacin; CST, colistin; FOF, fosfomycin; TGC, tigecycline; MIC, minimum inhibitory concentration.
Multilocus sequence typing
The results of MLST analysis are shown in Table 3. The most frequent ST was ST37 (5 of 29 isolates; 17%), followed by ST17 (4 of 29 isolates; 14%). One ST20, a SLV from ST17, was found; thus, CC17 consisted of five isolates. Two isolates belonging to ST17 were recovered from the hospital S-1, and PFGE revealed that those isolates were probably related by the criteria described by Tenover et al. 32 (data not shown). However, MICs of ciprofloxacin and levofloxacin for these two isolates were different, as shown in Table 3. Among the 29 isolates tested, two of them belonged to ST11 (7%). ST1130 was a SLV from ST528, and consequently, CC528 comprised two isolates (7%). ST37, ST17, ST20, and ST11 formed a large genetic complex CC37, and ST528 and ST1130 also formed another genetic complex CC528, as shown in Fig. 1, although CC17 and CC528 may have some genetic relatedness on the minimal spanning tree, as observed in Fig. 2.

Population snapshot by eBURST analysis (http://eburst.mlst.net) showing clusters of linked and unlinked STs in the entire K. pneumoniae MLST database. www.pasteur.fr/recherche/genopole/PF8/mlst/Kpneumoniae.html/. The dominant STs found in the present study are highlighted in box with arrowed lines. Most of them are within CC37 (inside the square), which includes many international multidrug-resistant STs. A color version of this figure is available in Supplementary Fig. S1 (Supplementary Data are available online at www.liebertpub.com/mdr).
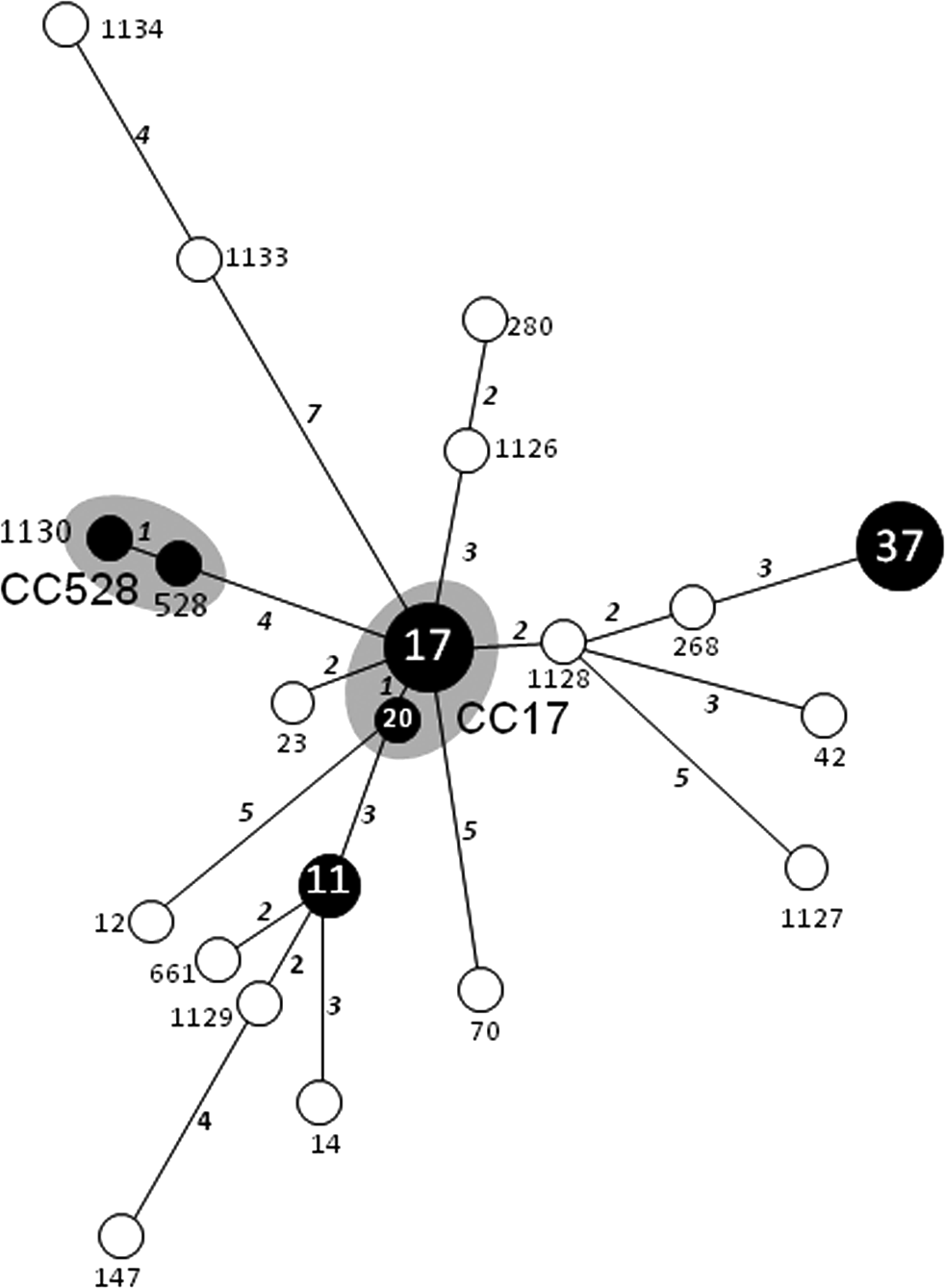
Minimal spanning tree of the 29 fluoroquinolone-nonsusceptible K. pneumoniae isolates in Japan. The gray zones represent the same clonal complex (six common alleles). The area of circles is equivalent to the number of isolates. The length of lines represents the number of alleles that are found in common between the STs connected to the lines, and the italic numbers next to the connecting lines correspond to the number of allelic differences. Black circles represent the dominant CCs and STs found in the present study.
No mutation was seen on the basis of gyrA and parC of K. pneumoniae ATCC 13833.
ESBL, extended spectrum beta-lactamase; PMQR, plasmid-mediated quinolone resistance; QRDR, quinolone resistance determining region.
ESBL and PMQR genes
As shown in Table 3, 15 of 29 isolates harbored genes for CTX-M-2, CTX-M-3, CTX-M-9, CTX-M-14, CTX-M-15, or CTX-M-65. Eleven isolates were positive for blaTEM, but none of them were ESBL producers; 10 of them were positive for blaTEM-1 and one was positive for blaTEM-1b. Most isolates had blaSHV, but only three of them harbored blaSHV-12. As plasmid-mediated AmpC, blaDHA-1 was found in 6 isolates. Eighteen isolates had PMQR genes, the most frequent one being qnrS, followed by qnrB, aac-(6′)-Ib-cr, and qnrA. Four of five aac(6′)-Ib-cr-positive isolates coharbored qnrB. The genes qnrC, qnrD, and qepA were not detected in the present study. fosA3 was found in the fosfomycin highly resistant (MIC, >256 mg/L) strain No. 9 (Table 2).
QRDR substitutions
Nine isolates (isolate Nos. 46, 49, 14, 28, 29, 52, 53, 62, and 65 shown in Table 3) did not have any amino acid substitutions in QRDRs, but they harbored at least one gene for PMQR and showed relatively low FQ MICs (≤32 mg/L) compared to the isolates having QRDR alterations. All the isolates belonging to ST37 and ST11 had more than two amino acid substitutions in QRDRs and showed higher quinolone resistance levels than those of other STs. Among the isolates belonging to singletons, four isolates (isolate Nos. 3, 11, 40, and 51) had more than two amino acid substitutions in the QRDRs of GyrA and/or ParC, and they also demonstrated considerably high resistance levels to FQs (Table 3).
Transfer of PMQR genes and PBRT
Transconjugants or transformants were obtained in 11 of 18 isolates that harbored PMQR (Table 4). Seven of them were selected directly by ciprofloxacin and four were indirectly selected by ampicillin. Genes transferred by conjugation and/or transformation by electroporation are also shown in Table 4, and ciprofloxacin and levofloxacin MICs for transconjugants and transformants with the PMQR gene are indicated in Table 4. PBRT was performed in all of the 11 transconjugants or transformants and only three were identified as IncN, but the others could not be determined by the PBRT.
tf, transformant; tc, transconjugant; A, ampicillin; C, ciprofloxacin.
ND, Inc type was not determined by the PBRT, PCR-based replicon typing.
Discussion
FQs have broad-spectrum antimicrobial activities against both gram-positive and gram-negative bacteria and have been used widely since the 1980s. In some parts of Europe like Greece, however, the rate of FQ resistance in K. pneumoniae has become very high, and this would be attributable to the high prevalence of carbapenemase-producing K. pneumoniae belonging to some genetic lineages like ST11. 33 On the other hand, there remain some regions, like Japan, where the prevalence of FQ-resistant K. pneumoniae is still much lower than that in the endemic areas of carbapenemase-producing K. pneumoniae (CPE). E. coli O25b:H4-ST131 has played a major role in worldwide dissemination of FQ-resistant E. coli, which have acquired genes for CTX-M-type ESBLs and multiple virulence factors.16,17,23,28 However, there are a few molecular epidemiological studies focused on FQ-resistant K. pneumoniae. Indeed, cephalosporin-resistant K. pneumoniae isolates, including ESBL-producing ones, tend to demonstrate resistance to FQs, but their genetic profiles still remain unclear. Thus, this is, to our knowledge, the first study on the genetic profiles of ciprofloxacin-nonsusceptible K. pneumoniae showing cephalosporin nonsusceptibility, conducted in the CPE nonepidemic areas.
The MLST analyses revealed that STs of ciprofloxacin-nonsusceptible K. pneumoniae isolated from Japan mainly consisted of two clusters: ST37 (n=5) and clonal complex 17 (CC17) (n=5), including ST17 and ST20, a SLV from ST17. Three major STs, that is, ST37, ST17, and ST11, related to FQ-resistant K. pneumoniae, have often been found in the isolates acquiring various antimicrobial resistance genes, and they are included in the CC37, in which KPC-producing ST258 10 was also included. 35 CC17, including ST17 and its SLV ST20, was one of the major STs associated with ESBL production in Canada, 26 and ST37 was often found among the isolates producing various β-lactamases, for example, plasmid-mediated AmpC, 15 KPC,2,19 and NDM. 14 Although only two isolates were identified as ST11 in the present study, it is the most widely distributed one among these three STs, especially related to carbapenemases like KPC, NDM, and OXA-48. From examining 39 K. pneumoniae producing NDM-1 carbapenemase from India, the United Kingdom, and Sweden, ST11 was the unique type commonly found in all three countries. 12 Furthermore, ST11 was one of the major STs among ciprofloxacin-resistant K. pneumoniae isolates acquiring blaCTX-M-15 that has spread in Hungary, 11 and the OXA-48-producing K. pneumoniae that caused a nosocomial outbreak in Greece also belonged to ST11. 33 Thus, the CC37 isolates that harbor blaKPC, blaNDM, or blaOXA-48 genes had been spreading worldwide, including the European countries and the United States. However, carbapenemase producers are still very rare in Japan despite the considerable presence of CC37 isolates among the CIP-nonsusceptible K. pneumoniae isolates, as shown in Fig. 1. Since CC37 isolates tend to easily acquire various plasmids mediating a variety of drug resistance genes and become endemic, the trends of CC37 isolates should be monitored intensively to block their further spread, especially in the areas where carbapenem-resistant K. pneumoniae has not become endemic as yet, like Japan.
Multiple amino acid substitutions in QRDRs are needed to acquire high-level resistance to FQs, and the FQ MICs for the isolates possessing double or more amino acid substitutions in QRDRs were higher than those for the isolates without or with a single substitution, as found in the present study (Table 3). Interestingly, the isolates belonging to ST17 had one or no amino acid substitution in QRDRs, whereas all isolates belonging to ST37 and ST11 had double or more amino acid substitutions in QRDRs and augmented ciprofloxacin and levofloxacin MICs were found for these isolates. To the best of our knowledge, the relationship between MLST and QRDR alterations has not been well explicated in K. pneumoniae to date. Certain genetic lineages belonging to specific STs might have a tendency to accumulate multiple amino acid substitutions in QRDRs during frequent FQ use. It seems notable that 9 ciprofloxacin-nonsusceptible isolates investigated in the present study had no amino acid substitutions in their QRDRs, but all of them had at least one PMQR gene. Since the 9 isolates showed considerably high resistance levels to FQs by possessing wild-type GyrA and ParC, unidentified mechanisms other than PMQR acquisition, like altered permeability and augmented energy-dependent efflux pump systems such as AcrAB efflux system, 3 have been suggested among the 9 isolates.
Our study design has two limitations to discuss the genetic lineage of FQ-nonsusceptible K. pneumoniae in Japan. The first is that the investigated ciprofloxacin-nonsusceptible ones were selected among cephalosporin-resistant ones. The second is that the number of objective isolates does not seem to be enough. Before we investigated the genetic lineages of FQ-resistant K. pneumoniae, we chose 22 out of 176 K. pneumoniae isolates susceptible to both FQs and cephalosporins recovered from separate regions in Japan and investigated their STs as a preliminary study. As a result, no apparent ST clusters were found among them, and FQ-resistant K. pneumoniae was rarely found among the cephalosporin-susceptible ones. The fact that FQ-resistant ones are still very rare in Japan would depend on the scarce prevalence of carbapenemase-producing isolates. So, we select the objective isolates among the cephalosporin-resistant ones, in consideration of the fact that ESBL-producing isolates are often resistant to FQs. We believe that three STs (ST37, CC17, and ST11) are common among the ciprofloxacin-nonsusceptible K. pneumoniae isolates showing resistance to some cephalosporins, although these STs may well overlap the STs of ESBL producers.
In conclusion, we characterized 29 ciprofloxacin-nonsusceptible K. pneumoniae clinical isolates among the cephalosporin-resistant ones obtained from 24 hospitals located in 11 different prefectures of Japan; and 48.2% of the 29 isolates tested converged on four STs or CCs; ST37, CC17, ST11, and CC528. K. pneumoniae ST37, CC17, and ST11 are also known as the international epidemic lineages, which frequently produce KPC-, OXA-48-, or NDM-type carbapenemases worldwide. The remaining STs were singletons, however, some of them were novel ones newly identified in the present study. The trend of FQ-nonsusceptible K. pneumoniae isolates, particularly ST37, CC17, and ST11, should be carefully monitored hereafter to block their further spread.
Footnotes
Acknowledgments
Tigecycline was kindly provided by Pfizer Japan, Inc., Tokyo, Japan. This study was supported by a research grant from the Ministry of Health, Labour and Welfare, Japan (H24-Shinko-Ippan-010).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.