
Abstract
Community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) is now endemic in the United States. In Japan, CA-MRSA infections and CA-MRSA surveillance have been scarcely reported. In this study, we conducted a nationwide survey of CA-MRSA in Japan. We collected MRSA strains isolated from outpatients with skin and soft-tissue infection (SSTI) at 107 medical facilities from 24 prefectures in 2010 and 2012. Among 10,385 clinical samples from SSTI patients, 3,581 S. aureus isolates (35%) were obtained and 673 of the S. aureus strains (19%) were identified as MRSA. Among 625 MRSA strains tested in this study, 266 strains (43%) and 114 strains (18%) were classified as SCCmec types IV and V, respectively. Detection of virulence genes was as follows: Panton-Valentine leukocidin (PVL) gene (57 strains, 9%), exfoliative toxin (ET) gene (179 strains, 29%), toxic shock syndrome toxin-1 (TSST-1) gene (195 strains, 31%), or none. PVL-positive strains were classified into eight sequence types (STs) (i.e., ST1, ST5, ST8, ST22, ST30, ST452, ST59, and ST154) and six clonal complexes (i.e., CC1, CC5, CC8, CC22, CC30, and CC59). Only 10 PVL-positive strains (2%) were pulsed-field type USA300 clone. There were a wide variety of CA-MRSA clones in Japan, which were different from the situation in the United States.
Introduction
S
Molecular typing studies have shown that CA-MRSA differs from hospital-acquired MRSA (HA-MRSA). CA-MRSA belongs to distinct genetic lineages and it usually carries smaller SCCmec cassettes and specific virulence factors such as Panton-Valentine leukocidin (PVL) and arginine catabolic mobile element (ACME).1,10 CA-MRSA was also shown to have higher expression levels of toxins, phenol-soluble modulins and hemolysins, suggesting that these isolates are more virulent than HA-MRSA.2,24
Previous studies have reported that CA-MRSA infections caused by the USA300 clone (ST8/SCCmec IVa/PVL+) are extremely widespread in the United States, 16 whereas CA-MRSA infections in other parts of the world are generally caused by other clones, namely, the Southwest-Pacific clone (ST30/SCCmec IVc/PVL+), the Taiwan clone (ST59/SCCmec V/PVL+), and the European clone (ST80/IVc/PVL+).7,20
The few reports of CA-MRSA in Japan have suggested that PVL-positive CA-MRSA is very rare in the Japanese population22,25,29; however, the strains mentioned in these previous reports included HA-MRSA or were isolated from limited areas. It is therefore difficult to determine the epidemiological details of CA-MRSA clones in Japan from these reports alone.
To further characterize CA-MRSA in Japan, we collaborated with a large clinical microbiology laboratory in Japan that helped identify CA-MRSA strains from the skin and pus samples collected from outpatients all over Japan. Thereafter, we performed molecular characterization of these CA-MRSA strains. Our objectives were to determine the CA-MRSA population distribution structure and identify the main CA-MRSA clonal lineages in Japan.
Materials and Methods
Bacterial strains
Miroku Medical Laboratory Co. is a microbiology laboratory where clinical samples are sent from about 150 medical facilities all over Japan. We collaborated with Miroku Medical Laboratory Co., and collected skin and pus samples from outpatients in 2010 (between February and September 2010) and 2012 (between February 2012 and January 2013). We submitted these samples to the Miroku Medical Laboratory, which isolated S. aureus strains and tested them for antimicrobial susceptibility to oxacillin (OXA) using a broth microdilution method or to cefoxitin (CFX) using a disk diffusion method. The strains with ≥4 μg/ml minimum inhibitory concentration (MIC) for OXA or with ≤21-mm zone diameter for CFX were identified as MRSA. These MRSA strains from outpatients were likely to be community-acquired strains, although they may have included some HA-MRSA strains. These MRSA strains were treated as CA-MRSA in this study and were sent to the Department of Microbiology, Tokyo Medical University, for molecular characterization.
Since some of the SCCmec types are rare in Japan, the following strains were used as positive controls in this study: NCTC10442 (SCCmec type I), N315 (SCCmec type IIa), JCSC3063 (SCCmec type IIb), 85/2082 (SCCmec type III), JCSC4744 (SCCmec type IVa), JCSC2172 (SCCmec type IVb), JCSC4788 (SCCmec type IVc), JCSC4469 (SCCmec type IVd), JCSC4796 (SCCmec type IVg), WIS (SCCmec type V), and JCSC6774 (USA300 clone). These strains were provided by Prof. Keiichi Hiramatsu (Juntendo University, Tokyo, Japan). The strain JCSC7560 (ST8/SCCmec IVc) was provided by Dr. Masaaki Higashiyama (National Defense Medical College, Saitama, Japan). The strain ATCC49775 was used as a positive control for PVL genes.
Antimicrobial susceptibility testing
The MIC of each isolate was determined using a broth microdilution assay according to Clinical and Laboratory Standard Institute reference methods. 6 The antimicrobial susceptibility of each strain was tested using readymade dry plates (DP32) manufactured by Eiken Chemical Co., Ltd. Antimicrobial agents included OXA, CFX, gentamicin (GM), arbekacin (ABK), minocycline (MINO), erythromycin (EM), clindamycin (CLDM), sulfamethoxazole/trimethoprim (SXT), levofloxacin (LVFX), vancomycin (VCM), and teicoplanin (TEIC). The inoculum was adjusted to yield a cell density of 5×105 CFU/ml. The plates were incubated for 20 hr (24 hr for OXA and VCM) at 35°C and examined visually.
Molecular characterization
After the strains were cultured overnight in a heart infusion broth (Eiken Chemical Co., Ltd.), cells were harvested at 8000×g for 3 min. Bacterial DNA was extracted using the DNeasy Blood & Tissue Kit (Qiagen) with lysostaphin (Wako). Genomic DNA was used as a template for polymerase chain reactions (PCR) amplification.
SCCmec types (I–V) of MRSA were analyzed using a PCR assay, as previously described. 13 For the SCCmec type II and type IV, subtypes were further analyzed using a PCR assay.
Staphylococcal virulence genes were detected using a PCR assay with previously reported primers.9,14,19,26,27 Targeted genes included the PVL gene (luk-pv), 3 exfoliative toxin (ET) genes (eta, etb, and etd), toxic shock syndrome toxin-1 (TSST-1) gene (tst-1), and the ACME gene (arcA).
The PVL-positive strains were tested by MLST. MLST was performed using seven housekeeping genes, as previously described. 11 An allelic profile can be obtained from the MLST website (www.mlst.net/).
The PVL-positive strains were tested by the pulsed-field gel electrophoresis. After digestion of the genomic DNA by SmaI (New England Biolabs), the restriction fragments were separated using a temperature-controlled CHEF DR III system (Bio-Rad) under the following conditions: 6.0 V/cm for 24 hr at switch times ramped from 5 to 60 sec. After staining with ethidium bromide, the fragments were visualized using a UV transilluminator.
Results
Clinical and epidemiological data
During the study period, 15,042 samples of the skin or pus from outpatients were sent to Miroku Medical Laboratory Co., and various pathogens were isolated from 10,385 samples (Table 1). Among these isolates, 3,581 S. aureus isolates (34.5%) were obtained and 673 of these isolates (6.5%) were OXA-resistant MRSA. We targeted these strains on the assumption that these MRSA strains were community-acquired strains. We adopted only one strain when MRSA strains were isolated several times from the same patient. Eventually, 625 MRSA strains from the skin and pus samples were molecularly characterized. A total of 241 MRSA strains were isolated at 77 medical facilities from 23 prefectures between February 2010 and September 2010, and 384 MRSA strains were isolated at 107 medical facilities from 24 prefectures between February 2012 and January 2013. Most of the isolates were from the Kanto area (44.2%), where the population density is highest in Japan, followed by the Chubu area (41.3%) where the Miroku Medical Laboratory is located (Fig. 1). CA-MRSA strains were mainly isolated from patients up to 9 years of age (45.8%) (Fig. 2). The ratio of men to women was 51.7–46.7% (unknown, 1.6%). For contractual reasons between the Miroku Medical Laboratory and medical facilities, further clinical information was not obtained.
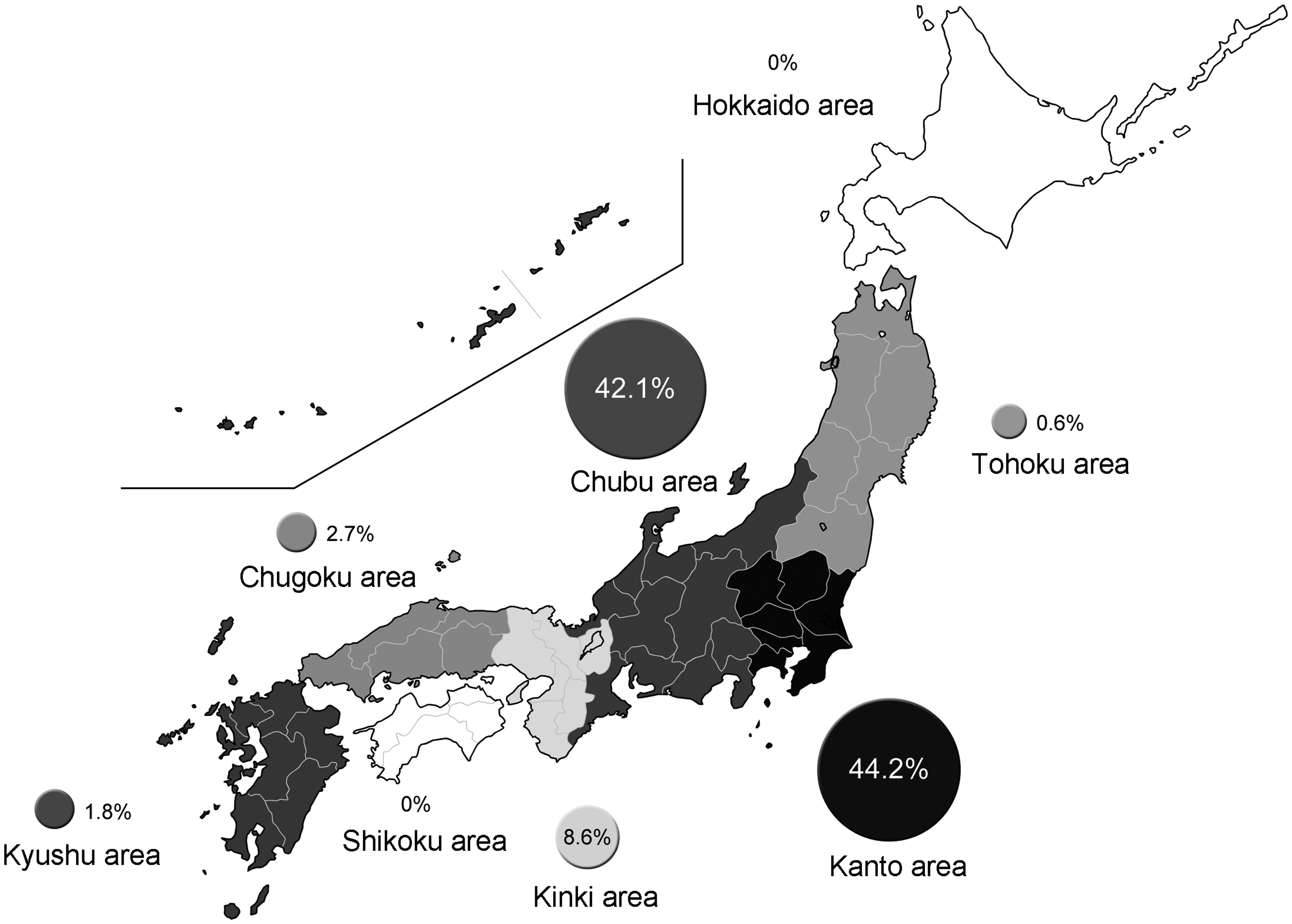
Area distribution of methicillin-resistant Staphylococcus aureus (MRSA) in Japan. Map adapted from http://edit.freemap.jp/rewriter_trial_version.php?id=edit/japan
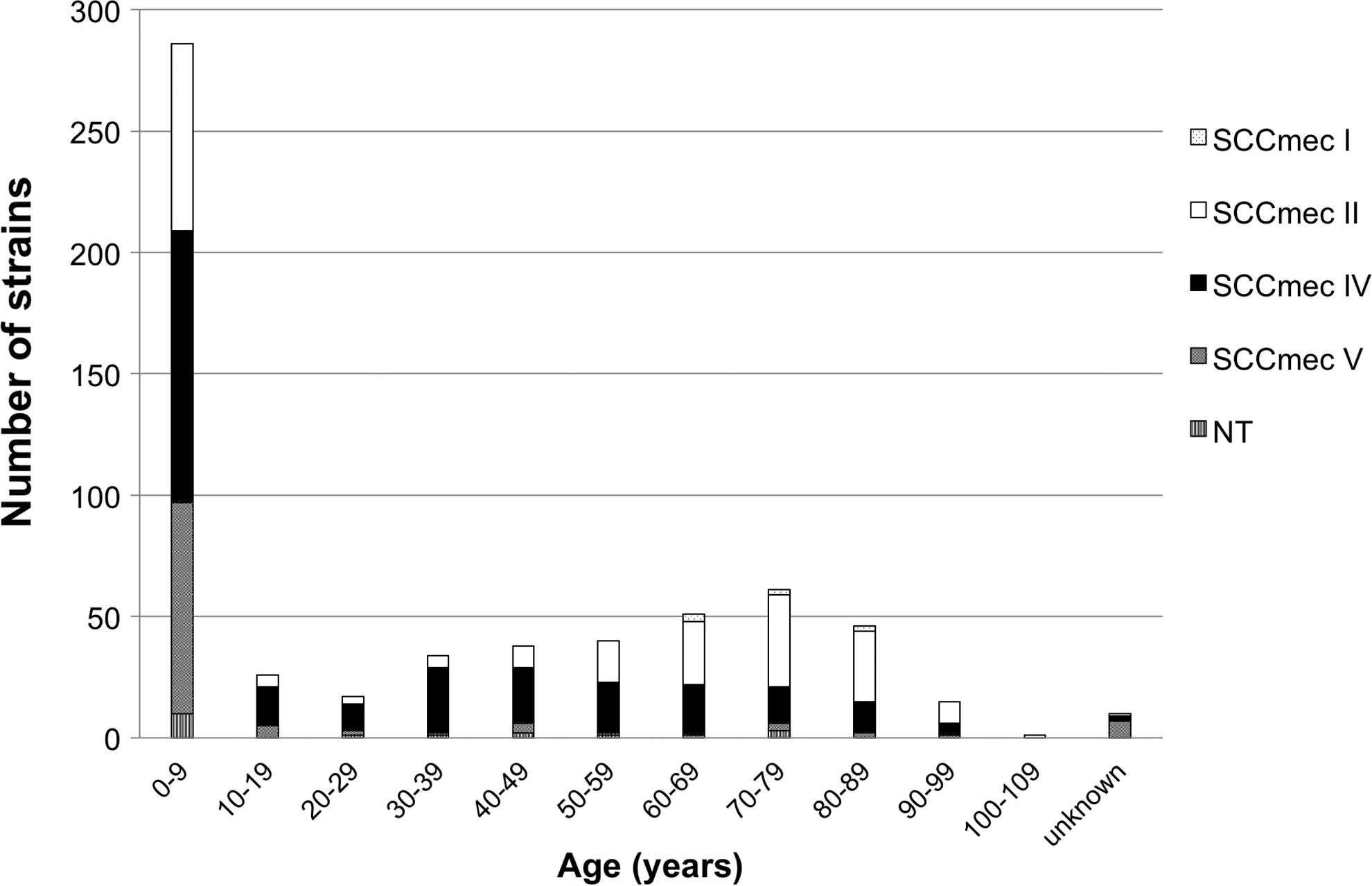
Age distribution. NT, not typed; SCCmec, staphylococcal cassette chromosome mec.
The detection aspects of the target sample in this study are shown.
About 20% of S. aureus were methicillin resistant, and there was no significant change (p<0.01) in the detection rate of MRSA between 2010 and 2012.
A total of 625 MRSA strains were molecularly characterized.
MRSA, methicillin-resistant Staphylococcus aureus.
SCCmec typing of MRSA
MRSA strains were classified into four types, namely, SCCmec type I (7; 1.1%), type II (220; 35.2%), type IV (266; 42.6%), and type V (114; 18.2%). The remaining 18 (2.9%) isolates were not typed (these isolates were not SCCmec types I–V).
SCCmec type IV strains were classified into two subtypes, namely, SCCmec type IVa (57; 21.4%) and SCCmec type IVc (63; 23.7%); 146 (54.9%) strains were not typed (these were not SCCmec types IVa–IVd). There were very few strains of SCCmec type IVa, the same type as the USA300 clone; type IVc strains were the most frequently isolated.
SCCmec type II strains were classified into two subtypes, namely, SCCmec type IIa (147; 66.8%) and SCCmec type IIb (42; 19.1%); 31 (14.1%) strains were not typed (these were not SCCmec type IIa or type IIb). SCCmec type II strains were frequently isolated from patients up to 9 years of age (35.0%), although another peak was identified in patients older than 60 years of age (47.3%) (Fig. 2). SCCmec type II strains accounted for more than a third of all the strains; these contained many SCCmec type IIb strains. Most SCCmec type IIb strains were isolated from children (90.5%), similarly as in CA-MRSA; however, SCCmec type IIa strains were mainly isolated from elderly patients.
Antimicrobial susceptibilities
The percentages of susceptible strains to each agent are shown in Table 2. Among all isolates, the MICs for SXT, ABK, VCM, and TEIC were very low. SCCmec type II strains tended to be resistant to LVFX, CLDM, FOM, and MINO; however, the strains of SCCmec types IV and V tended to be sensitive to these antimicrobial agents.
ABK, arbekacin; CFX, cefoxitin; CLDM, clindamycin; EM, erythromycin; FOM, fosfomycin; GM, gentamicin: LVFX, levofloxacin; MIC, minimum inhibitory concentration; MINO, minocycline; NT, not typed; OXA, oxacillin; SXT, sulfamethoxazole/trimethoprim; TEIC, teicoplanin; VCM, vancomycin.
Number of virulence gene-positive isolates
The results of virulence gene analysis are shown in Table 3. The TSST-1 gene was detected in 195 strains (31.2%), and most strains belonged to SCCmec type II (39.5%) and type IV (58.5%). ET genes (eta or etb) were detected in 179 strains (28.6%); etd was detected in no isolates, and most SCCmec type V strains were positive for ET genes (79.6%). The PVL gene was detected in only 57 strains (9.1%), and among them, 49 strains belonged to SCCmec type IV. Of the SCCmec type IV strains, 18.8% were PVL positive and all SCCmec type II strains were PVL negative. The ACME gene (arcA) was detected in only 27 strains that belonged to SCCmec type II, type IV, or to those unable to be typed.
ACME, arginine catabolic mobile element; ET, exfoliative toxin; NT, not typed; PVL, Panton-Valentine leukocidin; SCCmec, staphylococcal cassette chromosome mec; TSST-1, toxic shock syndrome toxin-1.
Molecular characteristics of PVL-positive MRSA isolates
Among the 57 PVL-positive strains, sequence type (ST) 30 clones were most frequently identified (24 isolates), followed by ST8 clones (20 isolates), and 6 additional STs, namely, ST1, ST5, ST22, ST59, ST154, and ST452 (Table 4). Most ST30 strains belonged to SCCmec type IVc, the same type as the Southwest-Pacific clone (ST30/SCCmec IVc/PVL+).
Pulsed-field types were divided into 8 clusters (A to H), and type A was the same banding pattern as that of USA400 clone, type B was USA800 clone, type C was USA300 clone, and type F was USA1100 clone, respectively.
MLST, multilocus sequence typing; CC, clonal complex; ST, sequence type; SCCmec, staphylococcal cassette chromosome mec; PFGE, pulsed-field gel electrophoresis.
ST8 strains belonged to SCCmec type IVa (10 isolates) and IVc (10 isolates). The pulsed-field types (PFTs) of ST8/SCCmec IVa strains showed the same banding pattern as that of the USA300 clone; however, the PFTs of ST8/SCCmec IVc strains showed a different banding pattern from that of the USA300 clone. The ST59 PVL-positive strain belonged to SCCmec type V and is regarded as the Taiwan clone.
Discussion
We performed molecular characterization of the CA-MRSA strains identified from samples collected nationwide in Japan. To the best of our knowledge, there has not been any nationwide surveillance of CA-MRSA in Japan. Yamasaki et al. reported that the MRSA ratio among S. aureus from furuncles was 17.5%, whereas Yamaguchi et al. reported that the MRSA ratio from impetigo was 51.1%.27,28 These ratios differed greatly because the strains analyzed in these reports were isolated from small groups in a limited region and were not generalizable. With regard to PVL-positive strains, there is less epidemiological information. In a Niigata survey, among the 84 S. aureus strains isolated from children with impetigo, 16 strains (19%) were MRSA and only 2 strains were PVL positive. 22 In a survey of healthy children, among the 231 S. aureus strains isolated from nasal swabs, 35 strains (15.2%) were MRSA and no strains were PVL positive. 12 From such a background, surveillance of MRSA isolated from some university hospitals in Japan was reported in 2012. 29 In that study, 857 MRSA isolates from 16 medical centers were analyzed and only six strains (0.7%) were found to be PVL positive. However, most patients who present to the university hospitals have chronic diseases and regularly visit hospitals in Japan. Thus, MRSA strains from university hospitals were isolated from the patients who have HA-MRSA risk factors, and the PVL-positive MRSA detection rate (0.7%) may show this among the MRSA strains containing HA-MRSA strains.
In this study, we collaborated with the Miroku Medical Laboratory Co., one of the largest outsourcing microbiology laboratories in Japan, in identifying MRSA strains in samples collected from the outpatients of many small hospitals that possibly have no microbiology laboratories. As a result, 3,581 S. aureus strains were isolated from SSTI and 673 MRSA strains were analyzed. There has not been any large-scale investigation as this study to date, and we believe that this is apparently the first report of a nationwide CA-MRSA surveillance that provides the most up-to-date information on CA-MRSA characteristics in Japan.
The MRSA ratio among S. aureus isolates from SSTI was 18.1%, and in the United States, the MRSA ratio among S. aureus isolates from community-associated SSTI was reported to be 78%. 16 It is suggested that the prevalence rate of CA-MRSA strains in Japan is lower than that in the United States. Interestingly, the ratios of CA-MRSA differed between the two nations, despite the similar high ratios of HA-MRSA among S. aureus isolates from nosocomial infections in Japan (about 60%) and the United States.3,17 We analyzed CA-MRSA strains by several typing methods. SCCmec types IV and V were mainly isolated from patients up to 9 years of age (42.1% and 76.3%, respectively) (Fig. 2). This meets the characteristics of CA-MRSA that have been reported in the United States or Europe. Isolates contained many SCCmec type II strains; however, subtype IIa strains, the same type as the New York/Japan clone, were isolated mostly from elderly patients. These isolates may be from patients who have HA-MRSA risk factors. Most strains of subtype IIb were isolated from children and this type of clone has been reported as a CA-MRSA clone.5,12,21 We may need to consider these two subtypes (IIa and IIb) as different types.
In this study, TSST-1 and ET genes were detected more frequently than PVL genes. The SCCmec type II/TSST-1+ strain is known to be the same type as the New York/Japan clone; however, the SCCmec type IV/TSST-1+ clone is little known as the dominant clone in any country in the world. This study suggests that the SCCmec type IV/TSS T-1+ clone is a frequent clonotype in Japan. The high detection rate of ET-positive CA-MRSA is attributable to the fact that MRSA strains have been isolated from impetigo in Japan. PVL genes were detected in only 10% of CA-MRSA strains; however, we believe that the detection rate is fairly high because there were few reports of PVL-positive CA-MRSA infections and it has been thought that there was a lower detection rate of PVL-positive CA-MRSA in Japan. It may be the Japanese typical environment in which some kinds of CA-MRSA clones are isolated, and the presence of various toxins in CA-MRSA suggested that CA-MRSA infections show various clinical pictures in Japan.
The USA300 clone is extremely widespread in the United States and is one of the clones of which there is consensus about virulence.8,15,18 In the present study, only 10 (1.6%) USA300 clones among 625 CA-MRSA strains were isolated. It is thought that the USA300 clone has not yet spread extensively in Japan. Although the USA300 clone was not completely detected in the United States before 2000, this clone became the leading cause of CA-MRSA infections during the last decade. 23 Furthermore, in Europe, USA300 clones have become one of the most prominent CA-MRSA strains in recent years. 20 Any differences between the United States and Japan, such as environmental factors, host species, and host bacterial flora, may affect the virulence of CA-MRSA strains. Although the PVL-positive rate of CA-MRSA strains did not change, the number of USA300 clones increased between 2010 and 2012.
Although this study includes data from many hospitals, our clinical information was limited because of the contractual restrictions between the Miroku Medical Laboratory and hospitals. Diagnosis of infections was not provided, and this study may actually contain cases that were not infectious disease cases. However, we believe that most isolates in this study were pathogens causing infections because incubation of clinical samples is regularly needed when infections are suspected. We were able to determine the ratio of CA-MRSA, the ratio of PVL-positive strains, and the type of Japanese dominant PVL-positive CA-MRSA because we collected the CA-MRSA strains from many institutions at an unprecedented scale instead of relying on clinical information. The information regarding CA-MRSA strains analyzed in this study contributes further to the diagnosis and treatment of CA-MRSA infections in Japan. Importantly, the patterns and trends of CA-MRSA isolates in the Japanese population should be continuously monitored and given attention.
Footnotes
Acknowledgments
We are indebted to Professor Keiichi Hiramatsu of Juntendo University, Tokyo, Japan, for providing the positive control strains used in this study. The authors are grateful to Dr. Edward F. Barroga, associate professor and senior medical editor of the Department of International Medical Communications of Tokyo Medical University, for the editorial review of the English article.
Disclosure Statement
No competing financial interests exist.