
Abstract
Introduction
S
Shigella infection is typically self-limiting although empirical treatment is often used. Shigella species progressively acquire resistance to several antimicrobial agents used for the treatment. 37 The emergence of multidrug-resistant (MDR) Shigella strains and the increasing resistance to commonly used antimicrobials is a growing concern worldwide4,37 as they affect both developed and developing countries due to increased international travel. 13 This is also leading to treatment failure and increased complications in the affected individuals. 24
The determinants of antibiotic resistance in Shigella isolates are frequently related to mobile genetic elements, including the resistance (R) plasmids, transposons, integrons, and genomic islands, on the bacterial genome that may facilitate the dissemination of resistance determinants among species, and even genera.17,27 In this regard, antibiotic resistance of Shigella isolates is related mainly to the presence of oxa-1-like β-lactamases for ampicillin, tetB genes for tetracycline, and activity of chloramphenicol acetyltransferase (CAT) for chloramphenicol. 20
There are limited existing data examining the change in the antimicrobial resistance profile of Shigella in Egypt. We previously reported that 58% of the Shigella isolates in Egypt were resistant to at least one member of three different antimicrobial groups.1,2 The objectives of the current study were to detect MDR in Shigella species isolated from patients with gastroenteritis at Minia Governorate, Egypt, determine the possible mechanisms of resistance, and compare their resistance profile to those reported in the same locality 20 years ago.
Subjects and Methods
Subjects
Five hundred patients suffering from gastroenteritis and attending Minia Fever Hospital participated in this study. Their age ranged from 1 to 70 years. Three hundred seven (61%) of the participants were males, while 193 were females. Three hundred six (61%) of the patients were residents of rural areas, while 194 were residents of urban areas.
Isolation and identification of Shigella
A total of 500 stool samples were collected from out-patients attending Minia Fever Hospital, with nausea, vomiting, fever, abdominal pain, and diarrhea with mucous and/or blood in the time period from August 2011 to August 2013. The study protocol was approved by the Council of Faculty of Medicine and its Institutional Review Board and the director of the Fever Hospital. Each subject consented before participation in the study. Shigella isolates were identified by standard microbiological methods, including Gram stain, and biochemical tests as previously described. 11 Isolates were kept frozen at −70°C in a trypticase soy broth containing 15% glycerol for further testing.
Antimicrobial susceptibility testing
Antibiotic sensitivity was determined by the disc diffusion method using the following antimicrobial discs: nalidixic acid (30 μg), ofloxacin (10 μg), ciprofloxacin (5 μg), tetracycline (30 μg), chloramphenicol (30 μg), sulfamethoxazole–trimethoprim (25 μg), streptomycin (10 μg), amikacin (30 μg), ampicillin (10 μg), ceftazidime (30 μg), and cefotaxime (30 μg; all from Bioanalyse). The testing and zone diameters were measured and interpreted according to the guidelines of the Clinical Laboratory Standards Institute. 10
Detection of β-lactamases
Shigella isolates resistant to penicillin and cephalosporin were examined for β-lactamase production as previously described. 34
DNA extraction and PCR amplification of tetB and cat genes
DNA was extracted from the Shigella isolates using a DNA extraction kit according to the manufacturer's instructions (Intron Biotechnology). DNA was used immediately or stored at −20°C until used. The tetB gene was amplified by PCR using the following primer set 36 : tetB F 5′ GAG ACG CAA TCG AAT TCG G 3′ and tetB R: 3′ TTT AGT GGC TAT TCT TCC TGC C 5′ (Eurofins). The sequence of the primers used for amplification of the cat gene 40 was as follows: Cat F: 5′ GGT GAT ATG GGA TAG TGT T 3′ and Cat R: 5′ CCA TCA CAT ACT GCA TGA TG 3′ (Eurofins). PCR was performed in a 25 μl reaction mixture containing 1 μl of template DNA (∼100 ng/μl), 12.5 μl of PCR master mix (2X DreamTaq® Green Master Mix; Fermentas), and 1 μl (10 pmol) of each primer and 9.5 μl of nuclease free water. The tetB reaction was carried out in a thermal cycler (Technie TC 512) as follows: initial denaturation at 94°C for 4 min, followed by 30 cycles of 1 min of denaturation at 94°C, 30 sec of annealing at 56°C, and 1 min of extension at 72°C and a final extension step at 72°C for 10 min. The cat gene was amplified using the same conditions except annealing at 50°C. PCR products were resolved on 1% agarose gel and visualized under a UV transilluminator (Biometra).
Results
Characteristics of the study population and identification of Shigella
Of 500 stool cultures, 24 (4.8%) samples were positive for Shigella. The remaining 476 isolates contained organisms other than Shigella (not shown). The mean age of the total study subjects was 17.4±15.6, while that of those having positive Shigella culture was 20.9±15.9 years, but the difference was not statistically significant (p=0.2). The frequency of isolation of Shigella from urban areas was 5.2% and was higher than that from rural areas (4.6%; p=0.4). Regarding gender of the patients, Shigella was isolated at a higher frequency from females (5.7%) than males (4.2%; p=0.2). Among the 24 isolates, Shigella flexneri was the predominant Shigella species (62%) followed by Shigella boydii (25%) and then Shigella dysenteriae (13%). No Shigella sonnei was detected in this study.
Antimicrobial resistance of Shigella
The isolated Shigella was tested for their antimicrobial susceptibility as described in the Subjects and Methods section. Table 1 shows that the isolates had a high percentage of resistance to ampicillin (21 isolates; 88%), tetracycline (20 isolates; 83%), and sulfamethoxazole–trimethoprim (18 isolates; 75%). Eleven isolates (46%) were resistant to chloramphenicol and 10 isolates (42%) were resistant to streptomycin. Lower resistance rates were found for ceftazidime (8 isolates; 33%), cefotaxime (6 isolates; 25%), amikacin (4 isolates; 17%), nalidixic acid (4 isolates; 17%), and ofloxacin (2 isolates; 8%). No resistance to ciprofloxacin was found (0%).
Shigella isolates (n=24) were tested for susceptibility to 11 different antimicrobial agents and their resistance profiles are shown.
Average±SD.
The gray color was used to distinguish resistance from sensitivity.
AM, ampicillin; TE, tetracycline; SXT, sulfamethoxazole–trimethoprim; CAZ, ceftazidime; CTX, cefotaxime; AK, amikacin; SM, streptomycin; NA, nalidixic acid; OFX, ofloxacin; CIP, ciprofloxacin; C, chloramphenicol; R, resistant; S, sensitive.
β-Lactamases were detected only in 9 of the 21 (42.9%) β-lactam-resistant isolates (data not shown). The tetB gene was detected in 16 of the 20 (80%) tetracycline-resistant Shigella isolates, but not among the sensitive ones (not shown). Similarly, the cat gene was detected in 82% of the chloramphenicol-resistant isolates, but not among the sensitive ones (Fig. 1).
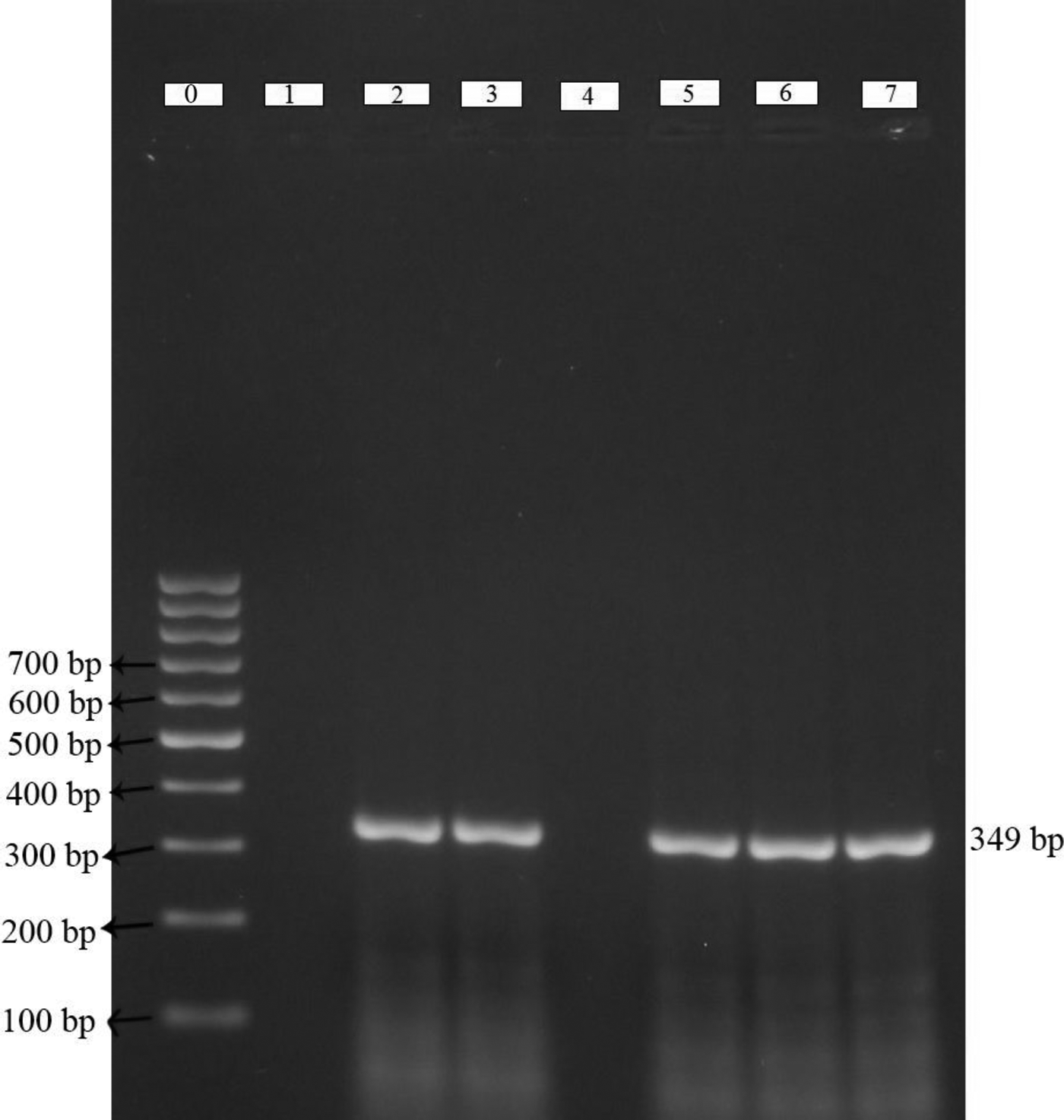
Amplification of cat gene by PCR in Shigella isolates. Amplicons of cat gene are as follows: lane 1 is for negative control, lane 4 is for chloramphenicol-sensitive isolates, while lanes 2, 3, and 5–7 are for chloramphenicol-resistant isolates. The cat gene band corresponds to a 349 bp, it is indicated with an arrow and left most lane is showing the 100 bp molecular weight marker.
The resistance patterns of the 24 Shigella isolates are shown in Table 1. As shown, 21 of the isolates (88%) were resistant to at least three different antimicrobial groups designating them as MDR isolates. Among these 21 MDR Shigella isolates, 6 isolates (29%) were resistant to 6 antimicrobials, and 6 isolates (29%) were resistant to 5 antimicrobials (Table 1). The average number of antimicrobial agents to which the Shigella isolates were resistant was 4.3±1.4. The 24 isolates also have 21 different resistance profiles (Table 1) suggesting considerable heterogeneity of their resistance patterns.
Table 2 shows the comparison of resistance to different antimicrobial agents between the current study (2014) and those we reported 20 years ago in our 1994 study in the same locality.1,2 As shown, there is a significant increase in the percentages of resistance of Shigella isolates to amikacin, nalidixic acid, ofloxacin, sulfamethoxazole–trimethoprim, cefotaxime, tetracycline, and ampicillin. By contrast, there was a decrease in streptomycin resistance. The resistance to chloramphenicol remained fairly stable (41% vs. 45%). Consistent with the previous report from 20 years ago, no resistance to ciprofloxacin was found. The 12 Shigella isolates from the 1994 studies1,2 had 8 different resistance profiles, while the 24 isolates reported in this study has 21 different resistance profiles.1,2 These data demonstrate the considerable heterogeneity of the resistance profiles of the Shigella isolates and their substantial change overtime.
MDR, multidrug resistance; ND, not determined.
Discussion
The emergence of MDR is a serious problem facing the management of shigellosis. In this study, we identified 24 Shigella isolates out of 500 stool samples (4.8%) from patients suffering from gastroenteritis. Among these isolates, we found a high percentage of resistance to ampicillin, tetracycline, and sulfamethoxazole–trimethoprim (≥75%). Also, there were moderate percentages of resistance to chloramphenicol (46%), streptomycin (42%), ceftazidime (33%), and cefotaxime (25%). Lower resistance rates were recorded for amikacin, nalidixic acid, and ofloxacin, while there was no resistant to ciprofloxacin. Twenty-one of the isolates (88%) were resistant to at least one member of three different antimicrobial groups classifying them as MDR isolates. The average number of antimicrobial agents to which the Shigella isolates were resistant was 4.3±1.4. When compared to our previous 1994 study in the same locality,1,2 the data show a marked increase in MDR and a change in the resistance profile of Shigella over the past 20 years.
The high percentage of ampicillin resistance recorded in this study (88%) is similar to previous reports,5,19 but higher than that reported in another study. 33 The percentage of tetracycline resistance found in this study (83%) was similar to those reported in Brazil, 29 China, 41 and Egypt. 5 In other studies, tetracycline resistance was found to be 63% 16 and 66% 20 in Mozambique. Sulfamethoxazole–trimethoprim resistance found in this study was 75%, while those reported in other studies included rates of 43%, 30 56%, 38 and 84%. 20 In this study, the resistance to chloramphenicol (46%) was similar to a previous report in the same locality,1,2 where the resistance was 42%, and also in other localities.14,23 Higher chloramphenicol resistance rates were recorded in other reports.28,41 This study shows a moderate percentage of resistance to streptomycin (42%) and a low percentage of resistance to amikacin (17%), which were similar to those found in other studies.12,22,32 However, another report showed higher resistance rates to streptomycin. 29 The high percentage of resistance rates recorded in this study and the above-mentioned reports may be due to the pattern of usage of these antimicrobials in these localities.
In this study, there was a low percentage of resistance to nalidixic acid (17%) and ofloxacin (8%), and no resistance to ciprofloxacin (0%). In another report, all Shigella isolates were susceptible to nalidixic acid, ofloxacin, and ciprofloxacin. 16 Higher resistance rates were recorded in Cameroon for nalidixic acid (60%) and ofloxacin (20%), but not (0%) for ciprofloxacin, 25 and similar rates were recorded in Turkey. 26 The resistance rate to third-generation cephalosporins in this study was 33% for ceftazidime and 25% for cefotaxime. It was reported that ceftazidime resistance was 0% and that of cefotaxime was 6%. 39 A resistance rate of 8% to ceftazidime and 22% to cefotaxime was also reported. 21 On the other hand, all Shigella isolates were susceptible to ceftazidime and cefotaxime.7,9 In a different study in Egypt, all Shigella isolates were shown to be susceptible to ceftazidime and cefotaxime. 5
In the present study, the mechanism of resistance of Shigella to tetracycline was mainly (80%) due to tetB gene expression, and the chloramphenicol resistance was mainly due to cat gene expression (83%). The remaining isolates likely have other resistance mechanisms. From the 21 ampicillin-resistant isolates (88% of Shigella), β-lactamases were detected in only 43% of isolates. The low rate of β-lactamase detection may be due to the technique used for detection of these enzymes as well as the presence of other resistance mechanisms. It should be noted that the resistance rate to third-generation cephalosporins in this study was 33% for ceftazidime and 25% for cefotaxime, which was accompanied or not with ampicillin resistance. These data raise the possibility of production of extended-spectrum β-lactamases, which was not examined in this study. In India, all Shigella isolates harbored the tetB and cat genes, 28 which confer resistance to tetracycline and chloramphenicol, respectively. In Mozambique, tetB was the main cause of tetracycline resistance (98%) and cat conferred resistance to 89% of chloramphenicol resistance among the Shigella isolates. 20 In California, more than half of the tested strains carried the tetB and cat genes. 6 In Taiwan, 9 tetB and cat genes were detected in (97%) of isolates.
The 12 Shigella isolates of our 1994 study1,2 had 8 different resistance profiles, while the 24 isolates reported in this study had 21 different resistance patterns, suggesting considerable heterogeneity of the isolates. The average number of antimicrobial agents to which the Shigella isolates were resistant in this study was 4.3±1.4, while it was 3.4±1.5 in the same locality in 1994.1,2 These data demonstrate an increase in the resistance of Shigella over time and suggest that their resistance profiles were substantially different from those reported in the same locality 20 years ago.1,2
This study also shows a significant increase in resistance of Shigella isolates to several antimicrobials (ampicillin, tetracycline, amikacin, nalidixic acid, ofloxacin, cefotaxime) over the past 20 years,1,2 while there was a decrease in streptomycin resistance (Table 2). On the other hand, resistance to chloramphenicol seems to be fairly stable (41% vs. 45%). The fluctuation in the percentage of resistance of Shigella isolates to different antimicrobial agents may be parallel to the change in the usage patterns of these antimicrobials during this period. As mentioned above, the average number of antimicrobial agents to which the Shigella isolates were resistant was 4.3±1.4, which is similar to previous reports.25,35,41 In this study, 21 of the 24 Shigella isolates (88%) were resistant to at least three different antimicrobial groups (indicating MDR). However, lower rates of MDR Shigella isolates were reported.18,26 The data also show a marked increase in MDR at the same locality of Minia Governorate in the last 20 years from 58%1,2 to 88% highlighting an alarming increase in antibiotic resistance in Egypt. The increase in MDR over the past 20 years in the same locality may reflect the indiscriminate and widespread use of antimicrobials in public health practices in Egypt, where people have ready access to various antimicrobials. Taken together, these data suggest the heterogeneity of the resistance profiles of the Shigella isolates and their substantial change overtime.
In conclusion, there is a marked increase and change in the resistance profile of Shigella to different antimicrobial agents over time in the past 20 years in Minia, Egypt. Continuous search, sensitivity-guided treatment, and constant monitoring of drug resistance are important for effective management of Shigellosis at Minia Governorate in particular and Egypt in general.
Footnotes
Acknowledgment
The authors would like to thank the staff members of Minia Fever Hospital for helping with the sample collection. This study was supported by funds from Minia University and by personal funds.
Disclosure Statement
All authors have nothing to declare regarding the data presented in this study. Also, they do not have any conflicts of interest.