
Abstract
We investigated the prevalence of methicillin-resistant coagulase-negative staphylococci (MRCoNS) isolated from hospitalized patients and outpatients (OP). Out of 350 staphylococcal isolates collected from three hospitals, 190 were coagulase-negative staphylococci (CoNS). These isolates were subjected to antimicrobial susceptibility tests, detection of mecA, and pulsed-field gel electrophoresis (PFGE) typing. Among the 190 isolated CoNS, Staphylococcus epidermidis (47.3%) and Staphylococcus haemolyticus (44.2%) were the most prevalent species. Other CoNS species that were isolated were Staphylococcus saprophyticus (2.1%), Staphylococcus warneri (2.1%), Staphylococcus simulans (1.6%), Staphylococcus capitis (1.1%), Staphylococcus schleiferi (1.1%), and Staphylococcus hominis (0.5%). The rate of resistance to methicillin was 60% with 58 (50%) S. epidermidis and 55 (49%) S. haemolyticus. The rate of resistance to 13 antibiotics tested with the lowest and highest to chloramphenicol and penicillin, respectively. High clonal diversity with different PFGE patterns was obtained for methicillin-resistant S. epidermidis and S. haemolyticus by 32 and 31 types, respectively. Our results indicated that the dissemination of MRCoNS is widespread in Tehran. The majority of these isolates showed distinct genotyping patterns. At the same time, the common patterns were found among the MRCoNS obtained from outpatient and inpatient isolates, suggestive of an epidemiological link.
Introduction
C
Methicillin resistance is determined by mecA gene, located on a large mobile genome known as staphylococcal cassette chromosome mec (SCCmec), 6 which also carries the genetic elements for other antibiotic resistance and transmissibility. 7 This gene has been found in more than 80% of CoNS late-onset sepsis isolates. 8
The mechanisms of dissemination of CoNS have been elucidated by many investigators3,23 suggesting the involvement of multiple factors, social and biological, in spreading of this bacteria. It is, therefore, critical to determine the level of methicillin-resistant staphylococcus (MRS) isolates at the local and international levels 25 and to determine their clonal diversity with the use of pulsed-field gel electrophoresis (PFGE) as a gold standard genotyping technique.24,25
The role of commensals in the spread of resistance among bacteria around the world cannot be ignored. We previously showed the prevalence of methicillin-resistant Staphylococcus aureus (MRSA) from clinical and hospital environment origins in Iran. 11 The present study has focused to identify the CoNS species, their frequencies and diversity in a comparative study, among hospitalized (HP) patients and outpatients.
Materials and Methods
Sampling, isolation, and identification
From July 2010 to March 2012, 350 staphylococcal isolates were collected from HP from three major hospitals 1, 2, and 3, and outpatients (OP) in Tehran, Iran. For HP patients, specimens were taken from patients whose date of admission to the healthcare facility and the date of discharge are on different calendar days, and the OP samples were collected from outpatient clinics. The inclusion criteria were based on the standard set by Center for Disease Control (Atlanta, Go). 9
All collected isolates were cultured on blood agar and incubated at 37°C for 24 hr. CoNS species were detected based on colony morphology, Gram staining, negative DNase activity, positive catalase, resistance to bacitracin (0.04 μg), and the absence of coagulase activity. In addition, for species identification, Voges-Proskauer test, arginine hydrolysis, urease test, nitrate reduction test, sugar fermentation tests (trehalose, sucrose, maltose, sorbitol, mannitol, and lactose), and novobiocin susceptibility were employed. 17
CoNS susceptibility testing
CoNS susceptibility was performed according to guidelines published by the Clinical and Laboratory Standards Institute (CLSI). 5 The following antimicrobial discs were used: penicillin (P) (10 U), gentamicin (GM) (10 μg), amikacin (AK) (30 μg), kanamycin (K) (30 μg), tobramycin (TO) (10 μg), erythromycin (E) (15 μg), tetracycline (TE) (15 μg), minocycline (MI) (30 μg), ciprofloxacin (CL) (5 μg), nitroforantoin (NI) (300 μg), clindamycin (CD) (2 μg), chloramphenicol (CL) (30 μg), rifampicin (RA) (5 μg), quinupristin/dalfopristin (SYN) (15 μg), cotrimoxazole (SXT) (25 μg), fusidic acid (10 μg), and linezolid (30 μg) (Mast Diagnostics Ltd, Bootle, Merseyside). The minimum inhibitory concentration (MIC) to vancomycin, teicoplanin, and oxacillin of the bacterial isolates resistant to cefoxitin disc (30 μg) was measured using the broth microdilution method as recommended by the CLSI. S. aureus ATCC 43300 (mecA positive) and ATCC 25923 (mecA negative) were used as quality control strains.
Amplification of methicillin resistance gene (mecA)
All the isolates were first phenotypically tested for their resistance to methicillin by the oxacillin test. Among methicillin-resistant (MR) CoNS isolates, the presence of mecA gene was evaluated by polymerase chain reaction (PCR). DNA was extracted using a DNeasy kit (Qiagen GmbH, Hilden, Germany) according to the manufacturer's instruction. Primer sequences were derived from previously designed primers mecA1: 5′-GTA GAA ATG ACT GAA CGT CCG ATA A-3′ and mecA2: 5′-CCA ATT CCA CAT TGT TTC GGT CTA A-3′. 4 PCRs were done in a 25 μL volume, including 1×PCR buffer, 2.5 mM MgCl2, each primer (40 pmole), 2.5 U Taq DNA polymerase, 0.2 mM dNTP Mix, and 5 μL of DNA template (10 μg/ml). Validation of the MRCoNS isolates was performed by amplification of the mecA gene in the following condition: 30 cycles of 15 sec at 94°C, 15 sec at 61°C, and 30 sec at 72°C. mecA-positive isolates produced a 310-bp band length, which was visualized by agarose gel electrophoresis.
PFGE typing
PFGE was performed for S. epidermidis and S. haemolyticus resistant to methicillin in a CHEF-DR II apparatus (Bio-Rad Laboratories, Richmond, CA). Briefly, a single and well-isolated colony grown on blood agar was inoculated into 10 ml of tryptic soy broth and grown on a reciprocal shaker at 37°C overnight. A bacterial suspension with 150 ml EC buffer (100 mM EDTA, 1 M NaCl, 6 mM Tris–HCl, 0.2% deoxycholate, 0.5% sodium lauroyl sarcosine, and 0.5% Brij-58) containing 20 ml lysostaphin (20 mg/ml) was added to 150 ml molten agarose gel and placed in plug molds. The plugs were treated overnight at 37°C with a lysis buffer containing lysozyme (1 mg/mL) and 5 mg of RNase per mL to the lysis buffer (6 mM Tris [pH 7.5], 1 M NaCl, 100 mM EDTA [pH 7.5], 0.5% Brij-58, 0.2% sodium deoxycholate, and 1% sodium lauroyl sarcosine). This solution was replaced by ES solution (0.5 M EDTA [pH 9.5], 1% sarcosine) and ESP solution (0.5 M EDTA [pH 9.5], 1% sarcosine, and 0.5 mg of proteinase K/mL) and the plugs were incubated for 48 hr at 50°C. The plugs were washed with the TE buffer and stored at 4°C. After digestion with 20 U SmaI (Roche, Manhiem, Germany), the plugs were placed in the wells of 1% agarose in 0.5% 9 Tris/Borate/EDTA and electrophoresed with switch times ramped from 5 to 35 sec at 6 V with a run time of 27 hr at 16°C. The gels were then stained with ethidium bromide and the restricted DNA was visualized with ultraviolet light. The banding patterns were clustered by the unweighted pair group method with arithmetic averages method using the software Gelcompar II version 4.0 (Applied Maths, Sint-Matens-latem, Belgium). Isolates having the same banding patterns or differing by one to three bands were regarded as identical and were assigned the same type or a subtype, respectively. The isolates that differed by more than three bands were not considered to be related and were regarded as different types.
Statistical analyses
Statistical analyses were done in IBM SPSS Statistics, Version 19.0 (IBM Corp. Released 2010; IBM SPSS Statistics for Windows, Version 19.0; IBM Corp, Armonk, NY). This software was used to conduct a Fisher's exact test (two-tailed) with the level of significance set at a p-value <0.05.
Results
Bacterial isolates and MRCoNS strains
Among the samples, 190 (54%) CoNS isolates were isolated with 100 and 90 CoNS isolates from HP and OP, respectively. S. epidermidis (55%, n=55) and S. haemolyticus (60%, n=54) were the most common species identified in HP and OP, respectively. Other CoNS species that were isolated, were Staphylococcus saprophyticus (2.1%), Staphylococcus warneri (2.1%), Staphylococcus simulans (1.6%), Staphylococcus capitis (1.1%), Staphylococcus schleiferi (1.1%), and Staphylococcus hominis (0.5%) (Table 1). Almost 60% (n=115) of CoNS isolates displayed methicillin resistance by the cefoxitin disk test and the presence of mecA gene (310 bp) was confirmed in all cefoxitin resistance isolates. Age data are reported for 115 MRCoNS patients. The mean age of patients was 41±21 years (range, 1–79 years). We divided these patients into five age groups (1–16, 17–32, 33–48, 49–64, and 65–80). Group III and IV with 28 (24%) isolates were the most prevalent ages followed by group II (27, 23%), V (18, 16%), and I (14, 13%). For HP 6 (9.2%), 19 (29.2%), 12 (18.5%), 16 (24.6%), and 12 (18.5%) isolates were in group I, II, III, IV, and V, respectively. For OP, 7 (14%), 7 (14%), 13 (26%), 9 (18%), and 14 (28%) isolates were in group I, II, III, IV, and V, respectively. There were no significant differences (p>0.05) between inpatient condition (HP or OP) and patient ages. The gender distribution among the 115 patients was tested (49% males and 51% females). S. epidermidis were the most common isolates among the MRCoNS in HP (n=39, 60%) isolates (p<0.05). On the other hand, S. haemolyticus (n=31, 62%) was the most common MRCoNS among OP isolates (p<0.05). Among OP samples, 30 and 20 strains were isolated from urine and wound infections, respectively, whereas the most common sources in the HP (n=65 MRCoNS) isolates were blood (n=27), wound infections (n=12), trachea, and catheter (n=18). Other sources were obtained from urine (n=4), body fluid (n=2), cerebrospinal fluid (n=1), and abscess (n=1) (Table 2). Of the 65 MRCoNS isolates in HP, 18 isolates were collected from intensive care units (ICUs) (27.7%), 15 from bone marrow transplantation (23.1%), 10 from blood and oncology (15.4%), 7 from orthopedic (10.8%), 7 from infection (10.8%), 6 from surgery (9.2%), 1 from nephrology (1.5%), and 1 isolate from dialysis (1.5%) wards.
CoNS, coagulase-negative staphylococci; HP, hospitalized; MRCoNS, methicillin-resistant coagulase-negative staphylococci, OP, outpatients.
Antibiotic resistance of MRCoNS strains
All MRCoNS isolates were susceptible to minocycline, nitroforantoin, linezolid, and quinupristin/dalfopristin disks. The majority of isolates were resistant to penicillin, erythromycin, and cotrimoxazole, which were observed in 115 (100%), 88 (76.5%), and 85 (74%) isolates, respectively (Table 3). Resistance rates for remaining antibiotic agents in HP and OP MRCoNS isolates have been shown in Table 3. Antibiotic susceptibility tests for HP and OP that exhibited resistance to amikacin (83, 17%), gentamicin (74, 26%), clindamycin (69, 31%), and fusidic acid (77, 23%) were significantly more (p<0.05) in HP isolates.
S. epidermidis showed a higher level of resistance to amikacin, gentamicin, chloramphenicol, clindamycin, and rifampin than S. haemolyticus, but only rifampin was statistically significant (p=0.001). Meanwhile, resistance to kanamycin (73% compared to 55%) and cotrimoxazole (87% compared to 60%) were significantly more in S. haemolyticus (p<0.05) (Table 3).
The MIC test showed that 27.6% and 72.5% of MR S. epidermidis (MRSE) and MR S. haemolyticus (MRSH) were highly resistant (MIC≥512 μg/ml) to oxacillin, respectively (Figs. 1 and 2). In addition, the MIC test showed that all the isolates were susceptible to vancomycin and teicoplanin. Furthermore, the oxacillin MIC for two isolates of S. hominis and S. warneri were ≥2 μg/ml.
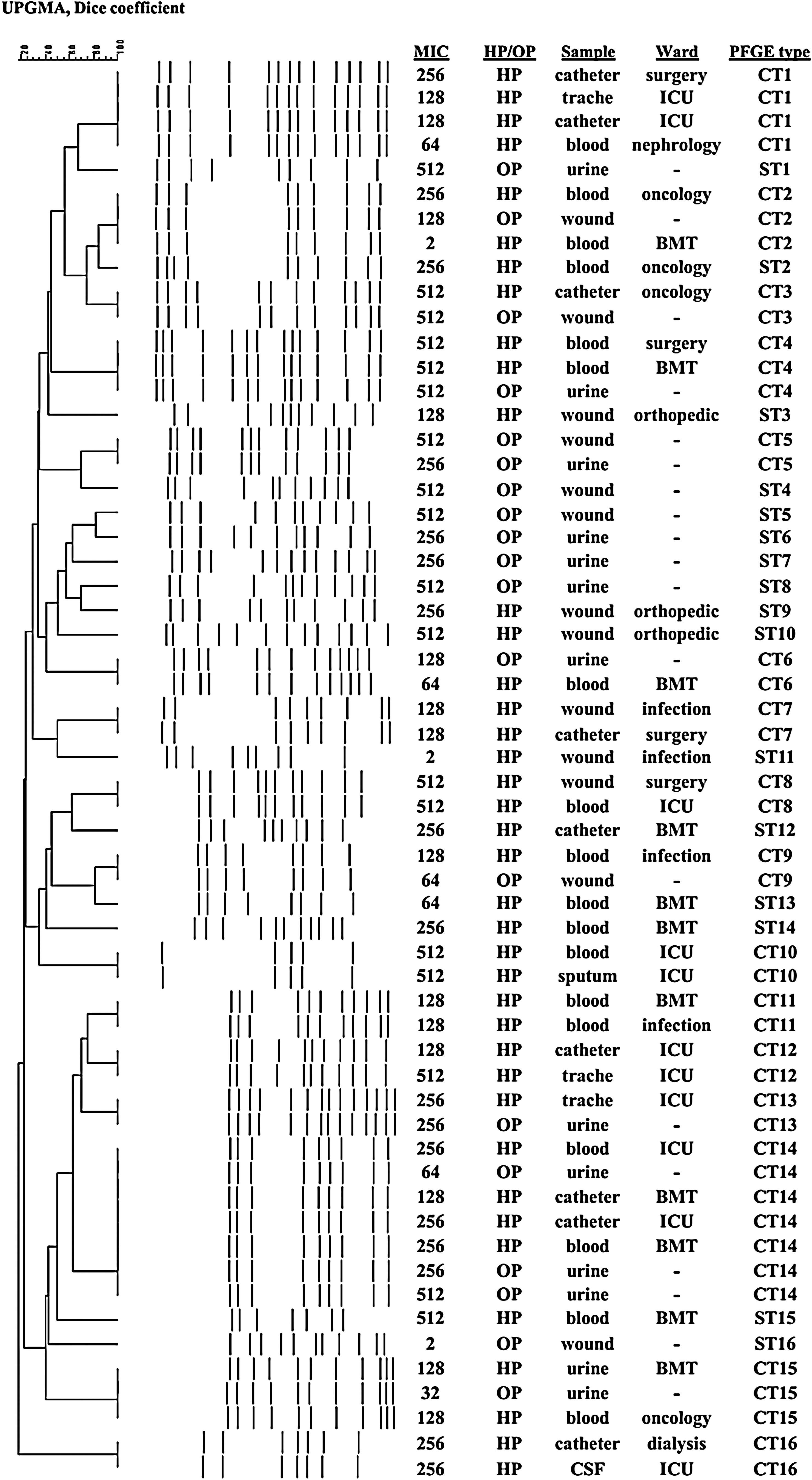
Pulsed-field gel electrophoresis (PFGE) patterns of MRSE isolated from outpatients and inpatients. HP, hospitalized; MIC, minimum inhibitory concentration; MRSE, methicillin-resistant S. epidermidis; OP, outpatient; UPGMA, unweighted pair group method with arithmetic averages.
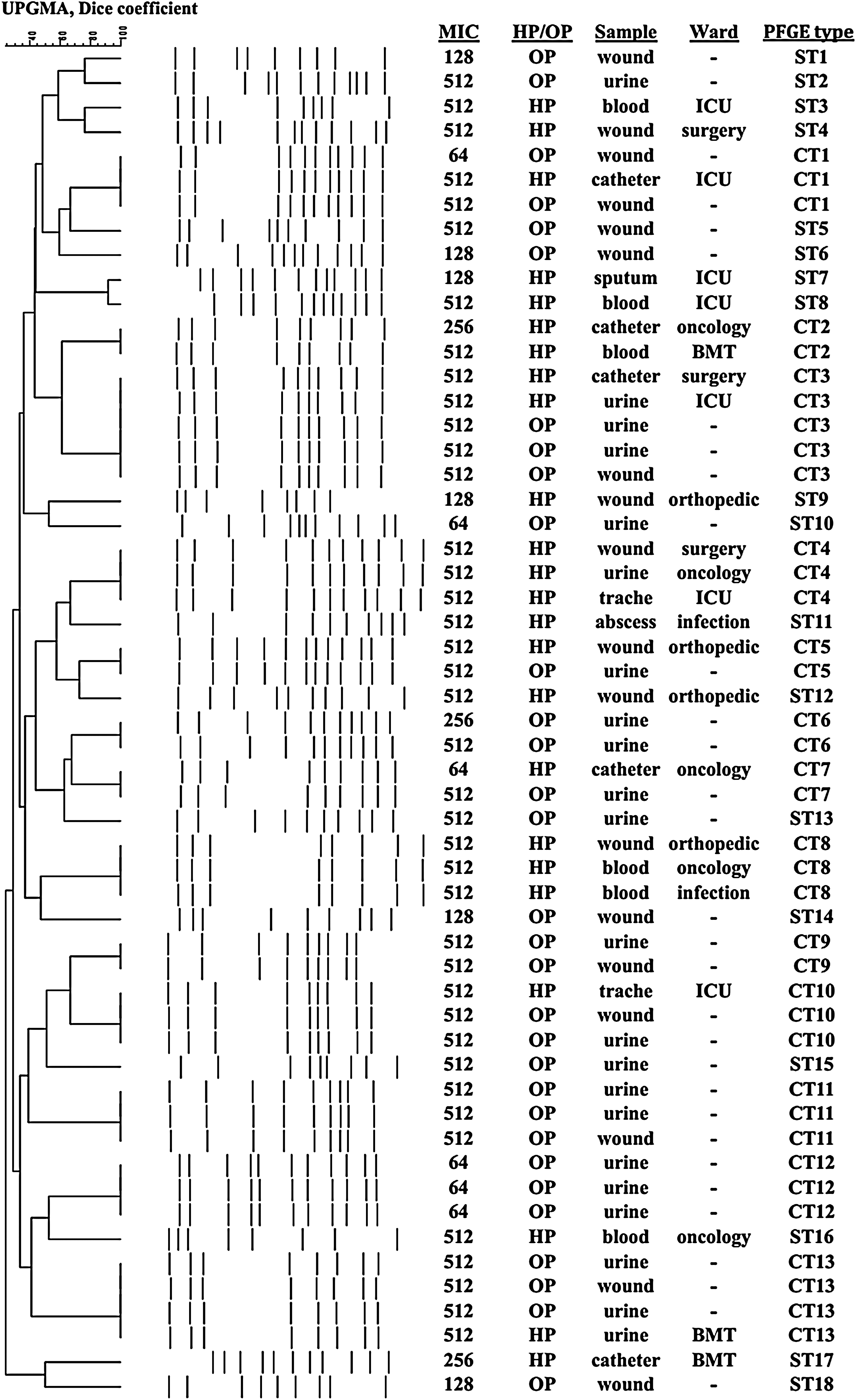
PFGE patterns of MRSH isolated from outpatients and inpatients. MRSH, MR S. haemolyticus.
PFGE typing
PFGE for MRSE (58) and MRSH (55) was performed and the results showed a notable genetic diversity among the strains (Figs. 1 and 2). Also, the results showed 32 PFGE patterns among the S. epidermidis (Fig. 1). The 58 MRSE showed 16 common pulsotypes (CT) constituting 42 (72%) isolates with 95% similarity (Fig. 1). The 16 isolates (28%) were highly dissimilar and were single types (ST). Among 16 CTs, there were five clusters with more than two isolates [clusters 1 (n=4), 2 (3), 4 (3), 14 (7), and 15 (3) comprising 20 isolates (48%)]. CT2, 3, 4, 6, 9, 13, 14, and 15 were found to be shared by HP and OP. CT strains, including 1, 7, 8, 10, 11, 12, and 16, were isolated from HP only and CT5 from OP. No significant differences were detected between the OP and HP (p>0.05).
Among 55 MRSH isolates, there were 18 STs and 13 CTs. CT isolates that accounted for 37 isolates (Fig. 2) and, among them, there were eight clusters with more than two isolates, including CT1 (n=3), CT3 (n=5), CT4, 8, 10, 11, 12 (n=3), and CT13 (n=4) [with 27 isolates (73%)]. CT isolates, including 1, 3, 5, 7, 10, and 13, were found to be shared by HP and OP. CT isolates in clusters 2, 4, and 8 were isolated only from HP, and CT6, 9, 11, 12, and 13 were isolated from OP. There were no significant differences (p>0.05) between the HP and OP.
Discussion
The distribution of MRCoNS was previously described in hospitals,3,6 as well as in the community.1,10 Our results were similar to the prevalence of MRCoNS in OP and HP isolates from Algeria and Brazil carried by Ruppe et al. 19 and Silva et al. 20 On the other hand, there was a similar prevalence of MRCONS in OP (44%) and HP (56%) isolates in our study suggesting that MRCoNS had been disseminated in the community, which has been attributed to the antimicrobial overuse in the community. 1
CoNS and especially S. epidermidis is endogenous human skin flora and, hence, is easily transmissible. 16 Two species, S. epidermidis (47.3%) and S. haemolyticus (44.2%), were the predominant CoNS isolates obtained in this study. Our results are similar to the results of Koksal and Wloch that showed the predominance of these species in Turkey and Poland, respectively.3,13
In addition, MRSE (60%) was the most isolated species from HP and MRSH (62%) from OP. This is in contrary to the results of Ruppe et al. and Silva et al. that reported S. epidermidis as the most prevalent species among OP isolates.19,20
In the present study, a significantly higher antibiotic resistance for the isolates obtained from HP was evident compared to OP, which could be due to antibiotic pressure. There were, however, some exceptions such as tetracycline. The level of tetracycline resistance for OP strains was significantly higher than HP as the use of this antibiotic, in different drug formats such as ointments, in community is overwhelming.
As expected, no resistance to vancomycin, teicoplanin, minocycline, linezolid, nitroforantoin, and quinupristin/dalfopristin was observed11,26 which could be due to the lack of usage of these antibiotics in Iran for CoNS. 22 Nevertheless, all the isolates, excepting two MRCoNS, were resistant to at least two antibiotics.
Furthermore, we found that MRCoNS were isolated more frequently from ICU wards (27.7%) compared with the other wards in the hospital. This increase could be due to the fact that the ICU ward could be the first arrival place in the hospital for the patients from community, consequently carrying MRCoNS in the hospital setting.
Using high resolution PFGE method, in accordance with other studies,2,10,15,23 a high degree of genetic diversity of MRCoNS isolates was found. Nosocomial circulation of S. epidermidis and S. haemolyticus strains has been documented by many authors and in many hospital wards.2,20 We observed 32 pulsotypes for MRSE with 16 STs and 16 CTs, including the 8 predominant ones (14, 2, 4, 15, 3, 6, 9, and 13), which were shared by HP and OP, suggestive of resistant isolates circulation between hospitals and community. Of the CTs, 10 and 12 were isolated only from ICUs. The CT1 with four isolates was predominant in hospital 1, which was isolated from different wards within the hospital (two ICUs, one surgery, and one nephrology). The 31 MRSH pulsotypes with 18 STs and 13 CTs, including the 6 predominant ones, were shared by HP and OP (3, 13, 1, 10, 5, and 7). Of these clones, the CT3 was found to have the same MIC in all isolates (MIC≥512 μg/ml). This result indicated the ability of this particular clone to disseminate and reach the high MIC level. We are in the process of further examining this strain and comparing its methicillin resistance genes to other clones.
The results indicated a strong link between the strains obtained from HP and OP. Of the isolates evaluated in this study, 23 (40%) MRSE and 21 (38%) MRSH were found with identical pulsotypes isolated from HP and OP. Indeed, these data suggest that the same MRCoNS clones can be identified in nosocomial and community settings. Thus, these findings of MRCoNS isolates would give us an understanding into the evolutionary dissemination of MRCoNS among inpatients and outpatients.
In conclusion, we found a high prevalence of MRCoNS among outpatients and inpatients. The presence of common MRCoNS PFGE types in the HP and OP further suggests the circulation of certain clonal types inside and outside hospitals. The control of either could result in a snap of the MRCoNS dissemination. Collectively, these data recommend that it may be required to establish infection control actions focused toward MRCoNS to avoid colonization of patients, mainly those at a nosocomial infection high risk, such as those receiving catheters, neonates, and immunocompromised patients.
Footnotes
Disclosure Statement
No competing financial interests exist.