
Abstract
Molecular features of the first carbapenem-resistant Klebsiella pneumoniae isolates (KP1 and KP2) from the University Hospital Tahar Sfar, Tunisia, were investigated. Antimicrobial susceptibility testing, multilocus sequence typing, S1 nuclease pulsed-field gel electrophoresis, Southern blot, and polymerase chain reaction (PCR)-based replicon typing were performed. Extended-spectrum β-lactamases and carbapenemase genes were detected by PCR and sequencing. Both isolates were multidrug resistant. KP1 was of sequence type (ST) ST101 and exhibited blaCTX-M-15 and blaTEM-1 on an untypeable plasmid and blaOXA-48 on an IncL/M plasmid. KP2 was genetically unrelated to KP1 (ST147) and harbored an IncA/C plasmid carrying blaCMY-4 and the blaOXA-48 derivative gene: blaOXA-204. This study reports the second case worldwide of an OXA-204-producing K. pneumoniae isolate from the same country, however, in a different genetic background.
Introduction
R
In Klebsiella pneumoniae, carbapenem resistance can be conferred by various carbapenemases, among which OXA-48, a carbapenem-hydrolyzing class D β-lactamase, was abundantly reported, in particular from North Africa and Middle East countries.16,19 Several OXA-48 derivatives were also recognized overtime, although with different hydrolysis spectra depending on those variants. 14 Hence, similar to OXA-48, OXA-181 hydrolyzes carbapenems at a low level and spares broad-spectrum cephalosporins. On the other hand, OXA-163 hydrolyses carbapenems at very low levels, but broad-spectrum cephalosporins very efficiently. Recently, OXA-204, a new OXA-48 derivative, was characterized, which possesses a β-lactam resistance profile similar to OXA-48. 20
In Tunisia, OXA-48 is regarded as the main resistance mechanism associated with carbapenem resistance in K. pneumoniae. 19 The first report of an OXA-48 producer in Tunisia was in 2006, and since then, numerous cases have been reported.1,4,9,10,22 Our work was initiated by the first isolation in our hospital of two K. pneumoniae isolates (KP1 and KP2) in December 2012 and May 2013, respectively. The aim of the study was to investigate the mechanisms of carbapenem resistance in those isolates.
Materials and Methods
Bacterial collection
From June 2012 to June 2013, 106 nonrepetitive K. pneumoniae isolates were consecutively obtained from clinical specimens of different wards in the 800-bed Taher Sfar University hospital in Mahdia, Tunisia.
Epidemiological data
On December 10, 2012, a 70-year-old woman with severe chronic nephropathology was hospitalized for fever and back pain, and an imipenem-susceptible K. pneumoniae isolate was recovered from urine. The patient was treated with imipenem through 13 days and on the 23rd of December, a carbapenem-resistant K. pneumoniae KP1 was isolated. The KP2 isolate was recovered from a 30-year-old woman on the 27th of May 2013. This woman was admitted in the gynecology ward on the 17th of May 2013 for reduction of amniotic fluid. After childbirth by cesarean, she got fever and was treated with co-amoxicillin clavulanate. On 27th of May 2013, a carbapenem-nonsusceptible K. pneumoniae isolate KP2 was recovered from urine.
Susceptibility testing
Isolates were identified by API20E (bioMérieux, Marcy l'Etoile, France). Antimicrobial susceptibility testing was performed by disk diffusion on Mueller–Hinton agar plates with 32 β-lactam and nonβ-lactam antibiotic-containing disks according to the guidelines of the Antibiogram Committee of the French Society for Microbiology (CA-SFM; www.sfm-microbiologie.fr). 3 Escherichia coli ATCC 25922 was used as quality control. Isolates with inhibition zone diameters of imipenem smaller than 22 mm, or of ertapenem smaller than 25 mm, were selected for this study. ESBL production was confirmed by the double-disc synergy test and carbapenemase production by the modified Hodge test. Minimum inhibitory concentrations (MICs) to imipenem, meropenem, ertapenem, colistin, and tigecycline were determined by E-test® (bioMérieux).
Molecular characterization of genes, plasmids, and clones
The β-lactamase genes (blaCTX-M, blaTEM, blaSHV, blaOXA, blaCMY, blaOXA-48, blaKPC, blaNDM, blaVIM, blaIMP) were screened by polymerase chain reaction (PCR).6,17,18 Detection of plasmid-mediated quinolone resistance genes was performed using primers targeting qnrA, qnrB, qnrS, qnrC, qnrD, qepA, aac(6′)-Ib-cr, and oqxAB genes. All amplicons were sequenced (Beckman Coulter, London, United Kingdom) and sequences were analyzed using a BLAST search (www.ncbi.nlm.nih.gov/Blast.cgi). Conjugative transfer was tested in a liquid medium using rifampicin-resistant E. coli K-12 J53 as a recipient cell and transconjugants were selected on plates containing cefotaxime (4 mg/L) or imipenem (10 mg/L). Presence of the blaCTX-M-15, blaCMY-4, and blaOXA-48/OXA-204 genes in transconjugants was confirmed by PCR. The genetic environment of the blaOXA-48 gene was determined as previously described. 17 Plasmids were typed in both donor and recipient using the PCR-based replicon typing scheme. 2 Plasmid sizes were determined using S1 nuclease treatment followed by pulsed field gel electrophoresis (S1-PFGE). Plasmids carrying the beta-lactamase genes were determined by S1-PFGE followed by Southern blot using the appropriate probes. The clonality of the K. pneumoniae isolates was investigated by PFGE and their genetic background by multilocus sequence typing. 7
Results
KP1 and KP2 isolates were resistant to all β-lactams tested, including carbapenems. For KP1, MICs to imipenem, meropenem, and ertapenem were all >32 μg/mL. For KP2, MIC to imipenem was >16 μg/mL, whereas MICs to meropenem and ertapenem were both >32 μg/mL. KP1 and KP2 also displayed high levels of resistance to tetracyclines, sulfonamides, aminoglycosides, and fluoroquinolones (Table 1). For both strains, MICs to colistin and tigecycline were 0.035 and 0.75 μg/mL, respectively. No other carbapenem-resistant K. pneumoniae isolate was recovered at the hospital between December 2012 and May 2013. The double-disk synergy test confirmed the ESBL production in KP1, but not in KP2. The modified Hodge test was positive for both strains.
KAN, kanamycin; TOB, tobramycin; NET, netilmicin; GEN, gentamicin; STR, streptomycin; TET, tetracyclines; SUL, sulfonamides; TMP, trimethoprim; NAL, nalidixic acid; ENR, enrofloxacin; OFL, ofloxacin.
PCR experiments followed by sequencing identified the blaCTX-M-15, blaTEM-1, and blaOXA-48 genes in KP1. Using a series of specific PCR primers, 17 two IS1999 insertion sequences bracketing the blaOXA-48 were identified, which correspond to the classical structure of the Tn1999.2 composite transposon. As demonstrated by S1-PFGE and Southern blot (Fig. 1), KP1 isolate possessed an 85-kb not typeable plasmid carrying blaCTX-M-15 and blaTEM-1 and a 70-kb IncL/M plasmid carrying blaOXA-48. Both plasmids proved to be conjugative. Finally, KP1 belonged to the ST101 clonal complex.
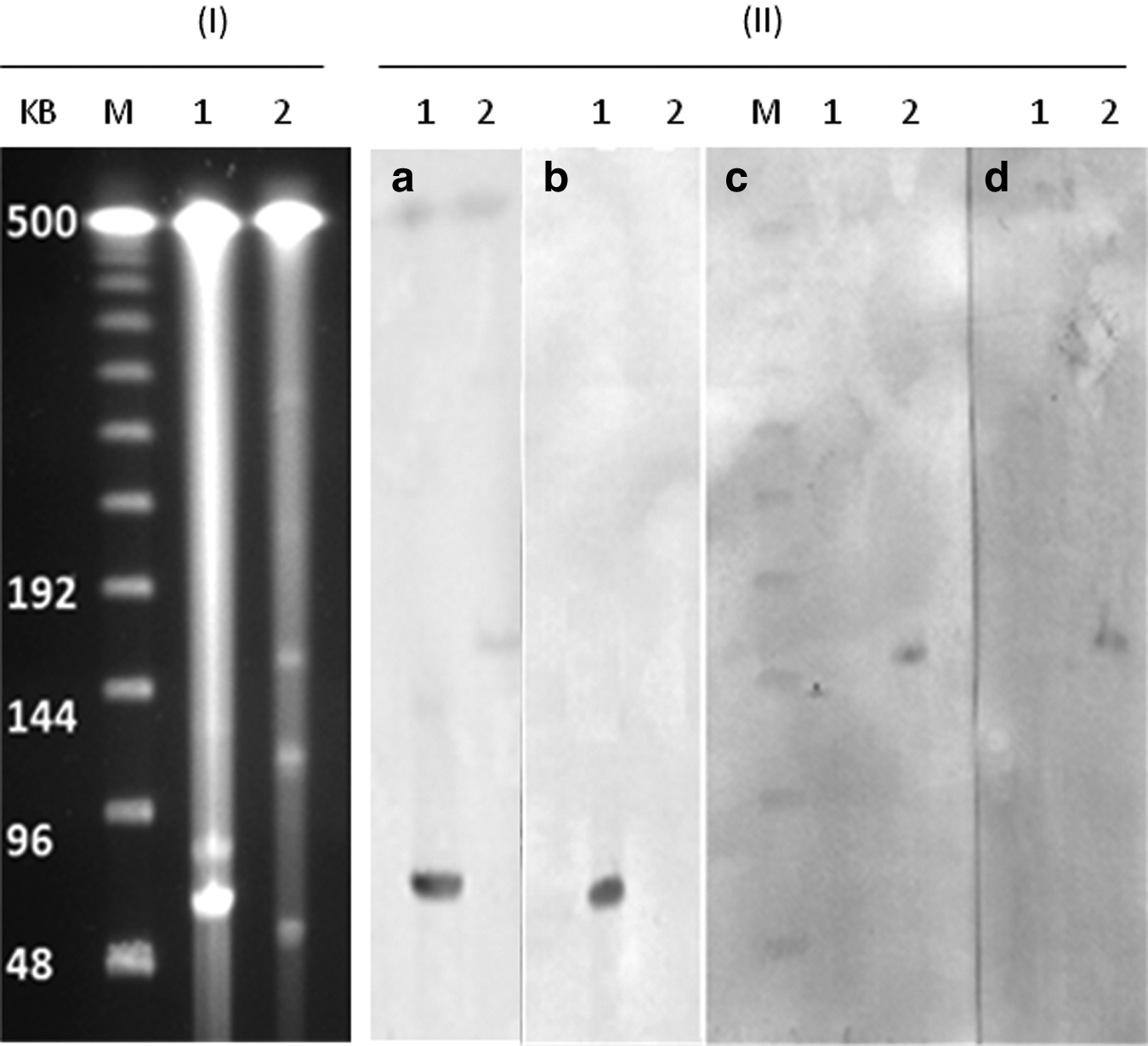
S1 nuclease pulsed-field gel electrophoresis (I) followed by Southern blot analysis (II) of KP1 (lane 1) and KP2 (lane 2). Hybridizations were carried out using OXA-48
On the contrary, KP2 harbored the blaCMY-4 gene and the blaOXA-48 derivative gene: blaOXA-204. The blaOXA-204 gene was preceded by ISEcp1 and the segment separating this gene from ISEcp1 was 46 pb. A unique 160-kb conjugative IncA/C plasmid harboring the blaOXA-204 and blaCMY-4 genes was found (Table 1, Fig. 1). In addition, KP2 belonged to ST147.
Beside beta-lactamase genes, KP1 and KP2 also possessed the oqxAB, qnrB1, and aac(6′)-Ib-cr genes.
Discussion
In this study, we characterized the first two carbapenemase-producing K. pneumoniae isolates (KP1 and KP2) in our hospital. Those isolates were identified from a series of 106 nonrepetitive K. pneumoniae isolates obtained from clinical specimens of different wards from June 2012 to June 2013.
KP1, which was a ST101 CTX-M-15-producing K. pneumoniae strain harboring a 70-kb IncL/M plasmid carrying blaOXA-48, reflects the common epidemiology of OXA-48-producing K. pneumoniae isolates in this geographical area. Hence, ST101 was reported as a predominant OXA-48-producing K. pneumoniae clone in several Mediterranean countries and IncL/M-type plasmids are also commonly reported as a vehicle of blaOXA-48 worldwide. 19
More interestingly, in KP2, we detected the blaCMY-4 gene and the blaOXA-48 derivative gene: blaOXA-204. This variant was published for the first time in 2013 in a K. pneumoniae isolate (K. pneumoniae 204) recovered in France from a patient who had been hospitalized in Tunis, Tunisia. 20 Till then, this variant had never been reported. Similar to K. pneumoniae 204, the blaOXA-204 gene was preceded by ISEcp1 and the segment separating this gene from ISEcp1 was 46 pb, as previously described. 20 The presence of ISKpn15 possibly truncating ISEcp1, as reported for K. pneumoniae 204, was not investigated. If present in KP2, this element obviously did not disrupt the promoter sequences located in ISEcp1 involved in the expression of blaOXA-204.
K. pneumoniae ST147 had never been reported in Tunisia before. However, ST147 was recognized at several occasions disseminating ESBLs 21 or carbapenemase genes. Recently, K. pneumoniae ST147 producing carbapenemases belonging to the VIM and NDM groups was reported.11,15,23 A recent publication showed that ST147 K. pneumoniae was responsible for a VIM epidemic in Greece between 2005 and 2006. 8 In a recent survey, ST147 was also among the five major international clones of K. pneumoniae disseminating OXA-48. 12 Of note, K. pneumoniae 204, reported to produce OXA-204, was identified as a ST383 strain. 20 This indicates that at least two different K. pneumoniae genetic backgrounds were responsible for the spread of OXA-204 in the same country in 2012/2013, which is the period of isolation of both strains.
Similar to K. pneumoniae 204, the blaOXA-204 gene was also located on an IncA/C plasmid together with blaCMY-4, which remains unusual for such a plasmid scaffold to carry a blaOXA-48-like gene. IncA/C-type plasmids possess a broad host range, which might give high opportunities to blaOXA-204 to disseminate among different K. pneumoniae clones, including through possible intermediate passages in other bacterial species. Thus, the expansion of OXA-204 producers warrants being carefully monitored in the future.
Here, we report the first carbapenem-resistant K. pneumoniae isolates in our hospital. More importantly, we characterized OXA-204 for the second time worldwide, again with a Tunisian origin, but produced by a different K. pneumoniae genetic background. This study adds to the knowledge on the epidemiology of OXA-204, a still rare but an emerging OXA-48 derivative.
Footnotes
Acknowledgments
This work was supported by Agency for Food, Environmental, and Occupational Health & Safety (ANSES). Raoudha Grami has a fellowship from the Region Rhône-Alpes (Accueil Doc, CMIRA 2011) and from the Ministère de l'Enseignement Supérieur et de la Recherche Scientifique in Tunisia.
Disclosure Statement
No competing financial interests exist.