
Abstract
Streptococcus pneumoniae is the cause of high mortality among children worldwide. Antimicrobial treatment and vaccination are used to control pneumococcal infections. In Ghana, data on antimicrobial resistance and the prevalence of multidrug-resistant pneumococcal clones are scarce; hence, the aim of this study was to determine the antibiogram of S. pneumoniae recovered from Ghanaian children younger than six years of age and to what extent resistances were due to the spread of certain sero- and multilocus sequence typing (MLST) types. The susceptibility of 115 pneumococcal isolates, recovered in a previous study, to six antimicrobials was determined by disk diffusion test. Overall, 90.4% of isolates were intermediate penicillin resistant, 99.1% were trimethoprim resistant, 73.0% were tetracycline resistant, and 33.9% were sulfamethoxazole resistant. Low resistance was recorded for erythromycin (2.6%) and cefotaxime (5.2%). Overall, 72.2% of isolates were resistant to penicillin (I or R) and at least two other antimicrobials. MLST of 20 isolates showing resistance to at least four antimicrobials revealed a high diversity documented by 16 different clones, none of which had previously been associated with multidrug resistance. The resistances found may have emerged due to nonprudent antimicrobial use practices and there is a need to monitor and promote prudent antimicrobial usage in Ghana.
Introduction
S
Pneumococci are susceptible to many antimicrobials, of which penicillin and other β-lactams are preferred options for treatment.5,60 However, due to global misuse of penicillin, 54 there is an emergence of pneumococcal serotypes that exhibit a high-level penicillin resistance and increasingly also showed resistance to non-β-lactams such as tetracycline (TET), erythromycin (ERY), chloramphenicol (CAM), sulfonamide, ciprofloxacin, and clindamycin. 2
In Ghana, penicillin is the drug of choice for the treatment of pneumococcal infections; 19 nonetheless, penicillin resistance is gradually increasing and constitutes a significant public health problem.15,20,31,52 The situation is further aggravated by misuse of antimicrobials through access to drugs without prescription; hence, patients indulge in self-medication. 20 Other factors that may further worsen the antimicrobial resistance among the pneumococci in Ghana are the overprescription of antimicrobials by clinicians for respiratory tract infections, which might have viruses as the causative agents rather than bacteria. Often, proper diagnosis cannot be done due to lack of laboratory equipment, unavailability of reagents for susceptibility tests, and inadequate trained laboratory staff. 52 In addition, the doctor to patient ratio is very low; hence, the time pressure on physicians and patient demand for drugs lead to unprudent use of antimicrobials (Dr. Larbi of Central Laboratory, Korle-Bu Teaching Hospital, pers. comm.).
In a recent study in Ghana, S. pneumoniae serotype 19F was the predominant serotype identified followed by 6B and 23F. 15 Little is, however, known about the antimicrobial susceptibility and serotypes of S. pneumoniae associated with multidrug resistance (MDR) in Ghana as previous studies included relatively small number of isolates.17,31,40 Donkor et al. 19 reported that 48.6% of S. pneumoniae isolates were resistant to ≥3 antimicrobials, but did not study the association between multiple drug resistance and the prevailing serotypes. In addition, it has been documented worldwide that specific clones can dominate different pneumococcal serotypes 6 and these dominating clones can, furthermore, be related to increasing antimicrobial resistance among specific serotypes.16,42,51
However, in Ghana, data on the prevalence of multidrug-resistant pneumococcal clones are scarce; hence, the aim of this study was to determine the antimicrobial susceptibility of S. pneumoniae recovered from healthy Ghanaian children under six and to what extent resistances were due to the spread of certain sero- and multilocus sequence typing (MLST) types.
Materials and Methods
Pneumococcal strain collection
In the study by Dayie et al., 15 serotype and penicillin resistance of 132 pneumococcal isolates were described. From that study (Dayie et al. 15 ), 115 S. pneumoniae isolates (64 isolates from Accra and 51 isolates from Tamale) were included in the present study. The isolates were collected from March to July 2011 before the PCV-13 was introduced in Ghana. Seventeen isolates were not included in this study due to laboratory setbacks. These 115 S. pneumoniae isolates consisted of 113 isolates that were intermediate penicillin resistant and two that were fully penicillin resistant. Briefly, the isolates were collected from children in 11 nurseries (<48-month-old children) and 7 kindergartens (48- to 72-month-old children) with no signs of upper respiratory tract infection and no record of antimicrobial treatment for the past month. These sites were randomly selected in Accra and Tamale as described by Dayie et al. 15 In addition, Dayie et al. 15 established the serotypes of these strains by latex agglutination (SSI Diagnostica) with subsequent confirmation by the Quellung reaction test using serotype-specific antisera (SSI Diagnostica). Penicillin resistance was determined by agar disc diffusion using 1-μg oxacillin discs and minimal inhibitory concentration (MIC) testing with penicillin G MIC strips. 15
Antimicrobial susceptibility testing
The 115 S. pneumoniae isolates were tested for susceptibility to TET, ERY, CAM, cefotaxime (CTX), trimethoprim (TMP), and sulfamethoxazole (SMZ). The disk diffusion susceptibility test was performed using Rosco tablets (Rosco Diagnostica) by spreading an inoculum of 0.5 McFarland standard onto Müller-Hinton (Liofilchem S.R.L. Bacteriology Products) agar plates containing 5% sheep blood. The plates were incubated for 24 hrs at 37°C in a 5% CO2 environment provided by a candle jar, after which the readings were taken with a caliper. The antimicrobial susceptibility was determined according to the European Committee on Antimicrobial and Susceptibility Testing ([EUCAST], 2012. Clinical Breakpoint Table v. 2.0, valid from Jan. 1, 2012) guidelines and clinical breakpoints in exception of two antimicrobials (CTX and SMZ), for which EUCAST did not provide breakpoints; hence, the manufacturer's breakpoints were used (Rosco Diagnostica). S. pneumoniae ATCC 49619 was used as a control (EUCAST). The pneumococcal isolates were tested against TET (S≥23 mm, R<20 mm), ERY (S≥22 mm, R<19 mm), CAM (S≥28 mm, R<21 mm), TMP (S≥18 mm, R<15 mm), CTX (S≥28 mm, R≤23 mm), and SMZ (S≥18 mm, R<15 mm). MDR was defined as the resistance to penicillin (I or R) and at least two other antimicrobials.46,54
Multilocus sequence typing
Twenty S. pneumoniae isolates showing resistance to four or more antimicrobials were subjected to MLST (Table 1). The MLST was performed at the NSR Lab (Statens Serum Institut) using the protocol described by Lambertsen et al. 39 with sequence types determined using primer pairs for the aroE, gdh, gki, recP, spi, xpt, and ddl genes as listed in the MLST online database (http://pubmlst.org/spneumoniae/).
Non-PCV-13 isolates are not included in the vaccine.
MDR, resistance to ≥4 antimicrobials.
The gene sequence did not match any known MLST sequence.
MDR, multidrug resistance; MLST, multilocus sequence typing; PCV, pneumococcal conjugated vaccines; ST, sequence type.
Data analysis
Data were analyzed using GraphPad Prism version 5 (GraphPad Software, Inc.) for descriptive statistical analysis. The MLST scheme database from http://pubmlst.org/spneumoniae/was used for MLST identification. From the allelic distance, groups of closely related isolates were identified. In this study, a clonal complex is defined as isolates sharing six of the seven loci that define the allelic profile.
Ethical approval
Ethical clearance of the study and the original collection of specimens 15 were obtained from the University of Ghana Medical School (MS-Et/M.5-P.5.4/2010-11) and permission to conduct the study was obtained from the Ministry of Education and Health. Informed consent was provided by the parents of children participating in the study.
Results
Among the isolates studied, 90.6% (58/64) from Accra and 90.2% (46/51) from Tamale showed intermediate penicillin resistance. A high resistance was found toward TMP in both Accra (98.4%; 63/64) and Tamale (100%; 51/51). More than half of the strains from both cities showed resistance to TET, whereas one-third of the isolates were resistant to SMZ (Fig. 1). The lowest prevalence of resistance was recorded for ERY and CTX (Fig. 1). Two isolates (serotype 6B and 19A) from Tamale showed an MIC >32 μg/ml to penicillin and were also resistant to TET and TMP. The serotype 6B isolate was, furthermore, resistant to CTX, while the serotype 19A isolate was resistant to CAM.
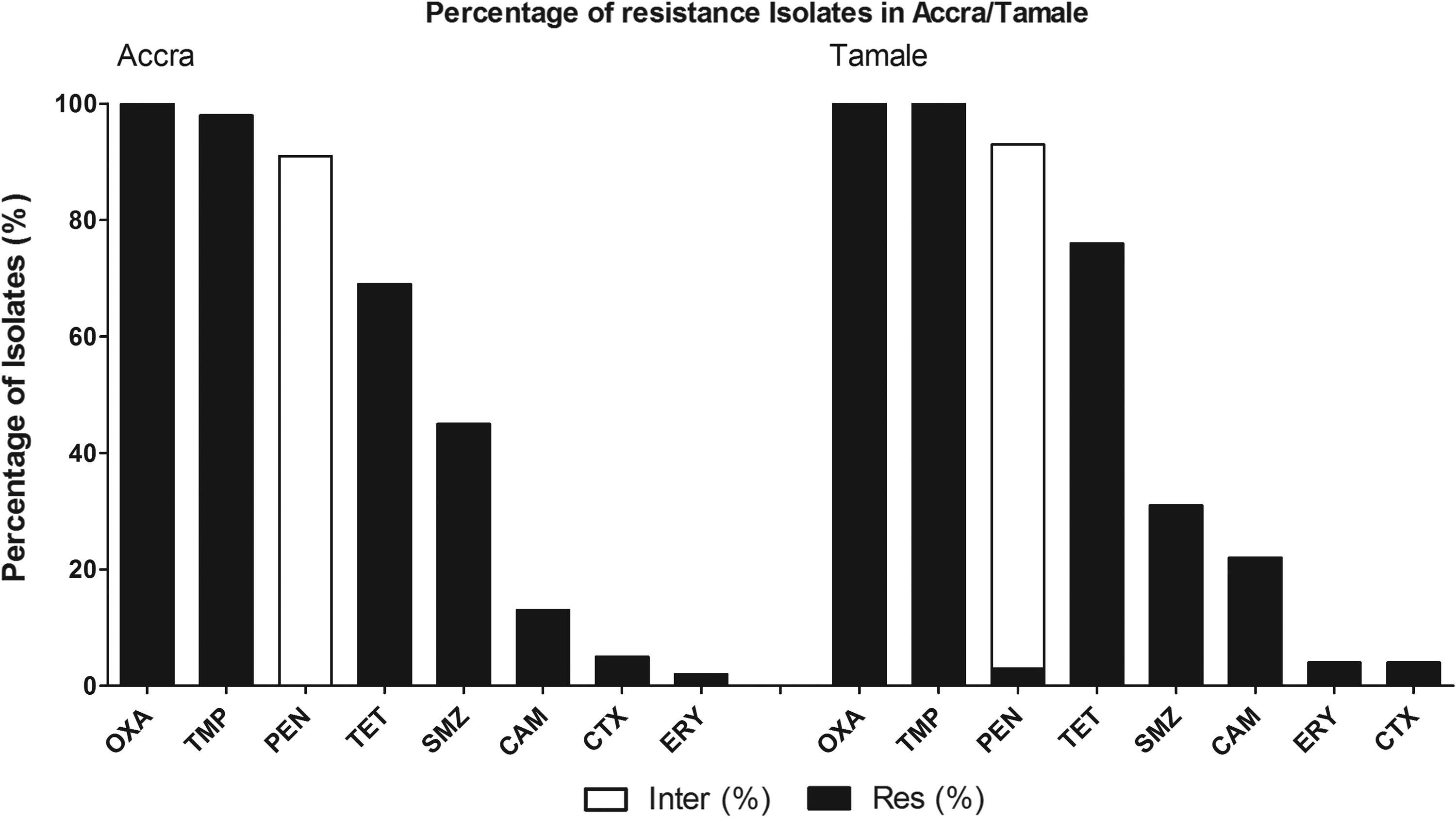
Antimicrobial susceptibility of 115 Streptococcus pneumoniae isolates from Accra and Tamale, Ghana; oxacillin (OXA), penicillin (PEN), trimethoprim (TMP), tetracycline (TET), sulfamethoxazole (SMZ), chloramphenicol (CAM), erythromycin (ERY), and cefotaxime (CTX).
A total of 43/64 (67.2%) isolates from Accra and 40/51 (78.4%) isolates from Tamale were resistant to multiple antimicrobials (Fig. 2). More specifically, 57.8% (37/64) isolates from Accra and 49.0% (25/51) isolates from Tamale showed resistance to three antimicrobials. Resistances to four antimicrobials were shown by 9.4% (6/64) and 29.4% (15/51) isolates in Accra and Tamale, respectively. One serotype 6A isolate showed resistance to all antimicrobials except CTX and one serotype 6C isolate showed resistance to all tested antimicrobials. The serotypes of the multiple-resistant isolates are shown in Fig. 2.
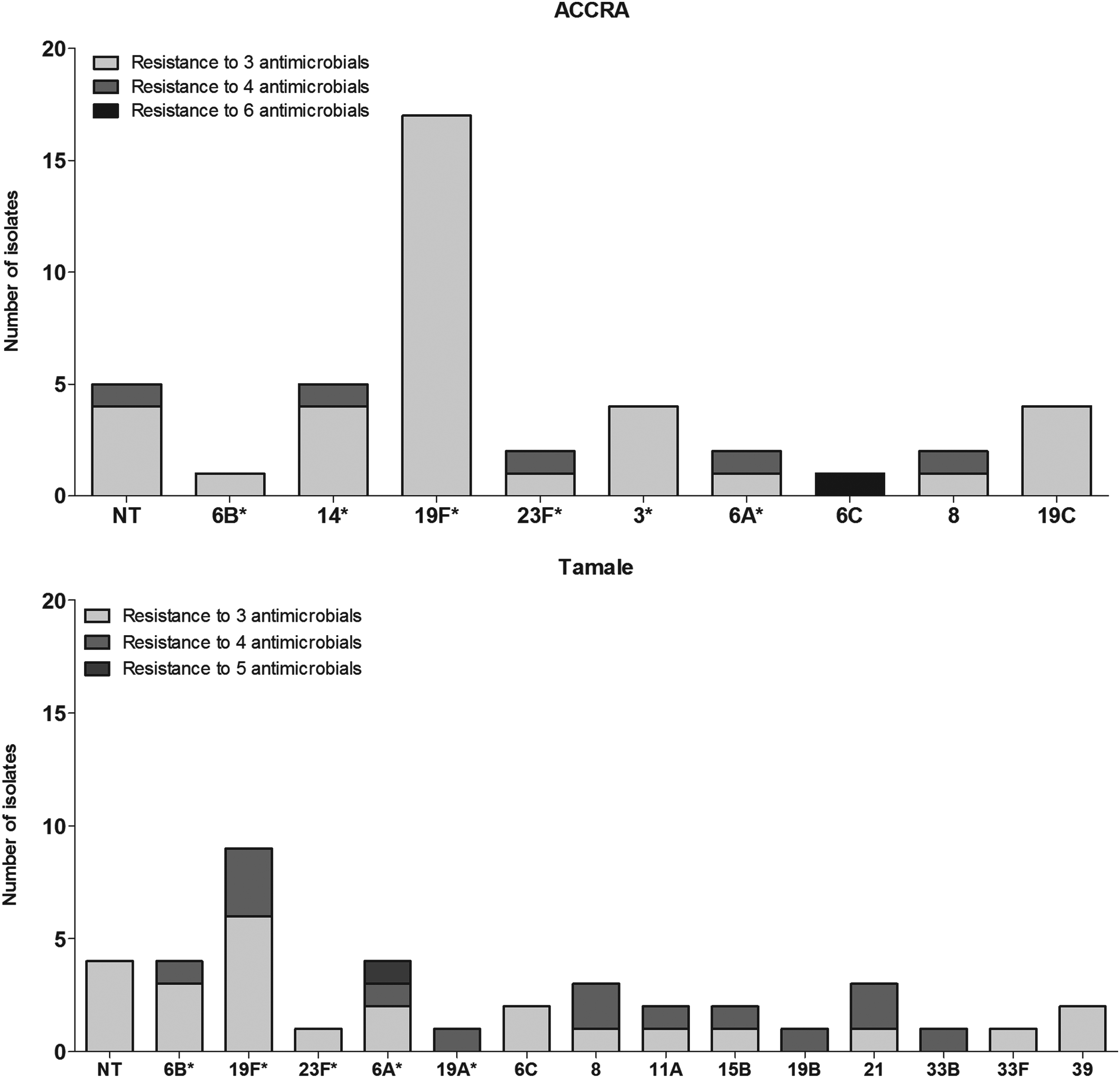
The serotype distribution of S. pneumoniae isolates, which were resistant to three or more antimicrobials. *Serotypes included in the pneumococcal conjugated vaccines (PCV)-13 vaccine.
Of the 43 multiresistant isolates from Accra, 12 isolates had serotypes not included in PCV-13 vaccine and of the 6 isolates showing resistance to four antimicrobials, serotype isolates 6C, 8, and an NT isolate were not included in the vaccine. The 40 isolates from Tamale that showed resistance to multiple antimicrobials represented 21 serotypes not included in the PCV-13 vaccine. Furthermore, among the 15 isolates showing resistance to four antimicrobials, 7 isolates belonged to serotypes not included in the PCV-13 vaccine (serotypes 8, 11A, 15B, 21, and 33B).
Table 1 presents the MLST of 20 S. pneumoniae isolates showing resistance to four or more antimicrobials, among which 16 different clones were observed. The serotype 6A isolate showing resistance to five antimicrobials and the serotype 6C isolate showing resistance to six antimicrobials were found to represent new MLST types and were not found clonally related to any of the other isolates in the minimum spanning tree analysis. The penicillin-resistant serotype 6B (ST4194) and serotype 19A isolate (ST847) belonged to two different clones. The sequence type (ST) of the 5 isolates from Accra showing resistance to four antimicrobials were not identical or related (six or more matches) to any ST of the 15 isolates from Tamale showing resistance to a similar number of antimicrobials.
Discussion
Recently, WHO published a report on the development of antimicrobial resistance worldwide, where it was stated that bacterial resistance has reached alarming levels in many parts of the world. 59 Globally, the prevalence of antimicrobial-resistant S. pneumoniae has also increased significantly, 38 with resistance shown not just to penicillin but also a wide range of non-β-lactam antimicrobials.3,28,32,36 Hence, treatment of pneumococcal infections is becoming difficult and the risk of treatment failure and prolonged hospitalization increasing.10,13 Our findings of multiple antimicrobial resistance (defined here as resistance to penicillin [I or R] and at least two other antimicrobials) shown by 72.2% of S. pneumoniae document that pneumococcal resistance to multiple antimicrobials is indeed on the rise in Ghana and is higher compared to a prevalence of 48.6% observed in a previous study in Ghana. 19 In addition, the 72.2% prevalence of MDR strains observed in our study is higher than the 16.5% in Tanzania 49 and 18.4% in South Africa. 13
The high intermediate penicillin resistances observed at both study sites (90.6% among isolates from Accra and 90.2% among isolates from Tamale) suggest mutation within the penicillin-binding proteins. 41 This mutation might be due to nonprudent use of antimicrobials, including use of substandard drugs, which is common among Ghanaians.20,52 There is evidence that the usage of substandard antimicrobials, the practice of truncating antimicrobial chemotherapy because of a lack of financial resources, 53 and exposure to low concentrations of antimicrobials during treatment may induce antimicrobial stress, which can lead to genotypic and phenotypic changes in the pneumococcus, 29 resulting in penicillin nonsusceptibility. 12
More than half of the isolates were resistant to tetracycline and this agrees with previous findings in Ghana.19,20,31,52 Tetracycline, although not included in the standard treatment guideline for treating pneumococcal infections in Ghana, was tested to observe current trends of pneumococcal resistance to tetracycline. It is, however, prescribed for the treatment of other bacterial infections in Ghana and is one of the drugs that have been abused among the Ghanaian population in the past. 52 Since resistance to tetracycline is mediated by genes borne on transposons, it is possible that the pneumococci acquired these genes from other organisms within the nasopharynx. Trimethoprim-sulfamethoxazole (TMP-SMZ) is recommended by the WHO as first-line treatment for respiratory tract infections in most resource-limited countries.1,58 However, it has been reported from a cross-sectional survey in Nigeria that 93.0% (187/201) of pneumococcal isolates from healthy children and adults in the Pakoto village of Ogun State was resistant to TMP-SMZ. The carriage prevalence of pneumococci in this study was 52.5% and the target sample population was in a range of 384–518 children <5 years. 1 The TMP-SMZ resistance reported by Adetifa et al. 1 is similar to findings in this study, where 99.1% of isolates were resistant to TMP and 33.9% of isolates were SMZ resistant. These observations are, furthermore, consistent with previous findings that the use of TMP-SMZ as a prophylactic measure against opportunistic infections selects for resistance.22,37,45 The use of sulphamethoxazole-pryrimethamine as the first-line antimalarial drug in countries endemic with malaria is also likely to contribute to TMP-SMZ resistance in S. pneumoniae. 56 In addition, sulfadoxine-pyrimethamine is recommended by the Ghana Health Service and administered to all pregnant women during antenatal care as a prophylaxis to reduce maternal anemia, placental parasitemia, and low birth weight due to malaria. 35
ERY is considered as an alternative drug for the treatment of pneumococcal infections; however, it is known in Spain and other European countries that ERY resistance in S. pneumoniae is now widespread 9 due to the increased usage of this antimicrobial among children less than 5 years of age.33,34 In addition, selection for coresistance seems more commonly associated with the use of macrolides than β-lactams.4,24 Although resistance to macrolides and β-lactams are common among pneumococci in Europe, 9 the situation in Ghana and other African countries are different. We observed a low resistance prevalence to ERY (2.6%) and CTX (5.2%) in pneumococcal isolates showing intermediate resistance to penicillin (Fig. 1) probably due to the minimal usage of these antimicrobials in Ghana, that is, mostly in hospitals rather than in communities like the ones sampled in our study.25,52 In addition, the low prevalence of ERY resistance in isolates showing intermediate resistance to penicillin is consistent with other studies done in East and West Africa.1,30,49
Our finding that 33 of the 83 multiple-resistant S. pneumoniae serotypes from Accra and Tamale were not included in the recently introduced PCV-13 vaccine 15 may indicate a problem of serotype replacement where nonvaccine serotypes with increased antimicrobial resistance and possible different virulence properties could replace pneumococcal serotypes included in the vaccine and subsequently lead to an increase in IPD. 13 The problems with antimicrobial-resistant S. pneumoniae and other bacterial pathogens in Ghana is, furthermore, worsened by inadequate human resources and lack of basic facilities for bacterial culture and antimicrobial sensitivity testing in most district hospitals.19,52 As a result, decisions on antimicrobial treatment are often empirical based on standard treatment guidelines and the essential drug list provided by the Ghana Health Sevice rather than specific laboratory diagnosis and antimicrobial susceptibility testing. 52
The MLST typing of 20 S. pneumoniae multidrug-resistant isolates showed a dispersed clonal relationship, in which 16 different STs were observed. None of the strains characterized in our study have their STs similar to that of the Pneumococcal Molecular Epidemiology Network clones associated with MDR globally. Nevertheless, some of the clones (ST802, ST847, ST344) identified in our study were also observed in other African countries.14,18,26 This very dispersed group of multidrug-resistant MLST clones indicates that it is not due to the spread of single clones, 43 which accounts for the increased antimicrobial resistance, but rather that the diverse group of multidrug-resistant clones are due to imprudent antimicrobial usage, for example, prudent use of antimicrobials may not be adhered to by clinicians and widespread public access to antimicrobials without prescription.20,52
Conclusion
This study shows that the antimicrobial resistance in pneumococcal isolates carried among young children in Ghana is high and for some drugs is close to 100% (Fig. 1). The data, furthermore, show that the introduction of the PCV-13 in the child vaccination program in Ghana might not have a larger effect on reducing the number of pneumococcal MDR isolates, in that, about 40.0% of the MDR serotypes were not included in the PCV-13. The MLST data showed that the origin of the MDR isolates was not due to spread of a few clones, but constituted a diverse group of different serotypes and clones (Table 1). The presented study strongly supports the need to continuously monitor antimicrobial resistance among bacterial isolates, including pneumococcal carriage isolates.50,59
Footnotes
Acknowledgments
We are most grateful to the Danish International Development Assistance (Danida) for their support to the project “Antibiotic Drug Use, Monitoring, and Evaluation of Resistance in Ghana” (ADMER project number 09-099SSI; ![]() ) that provided the funds for this study. We also wish to thank the Ministry of Health and Education of Ghana as well as the parents of the study subjects for having given us permission to carry out the research on the children. Finally, we wish to thank all senior researchers and their assistants who helped both in the Department of Microbiological Surveillance and Research at the University of Ghana Medical School and Statens Serum Institut, Copenhagen, for supporting the project.
) that provided the funds for this study. We also wish to thank the Ministry of Health and Education of Ghana as well as the parents of the study subjects for having given us permission to carry out the research on the children. Finally, we wish to thank all senior researchers and their assistants who helped both in the Department of Microbiological Surveillance and Research at the University of Ghana Medical School and Statens Serum Institut, Copenhagen, for supporting the project.
Disclosure Statement
No competing financial interests exist.