
Abstract
Introduction
I
Infections due to CRE are now classified as an urgent public health threat. 1 As the progress of antimicrobial resistance pushes us further into a postantibiotic era, clinicians are now faced with limited therapeutic options to treat these multidrug-resistant organisms. Moreover, antibiotic drug development has failed to match novel resistance mechanisms employed by bacteria. 18 As a result, physicians have been forced to rely on the available pharmacokinetic and pharmacodynamic data on existing agents to develop a suitable strategy to overcome these selected organisms. Notably, of the antibiotics that have shown an activity against CRE, most have profound toxicities that further complicate therapeutic decision-making.
Case Presentation
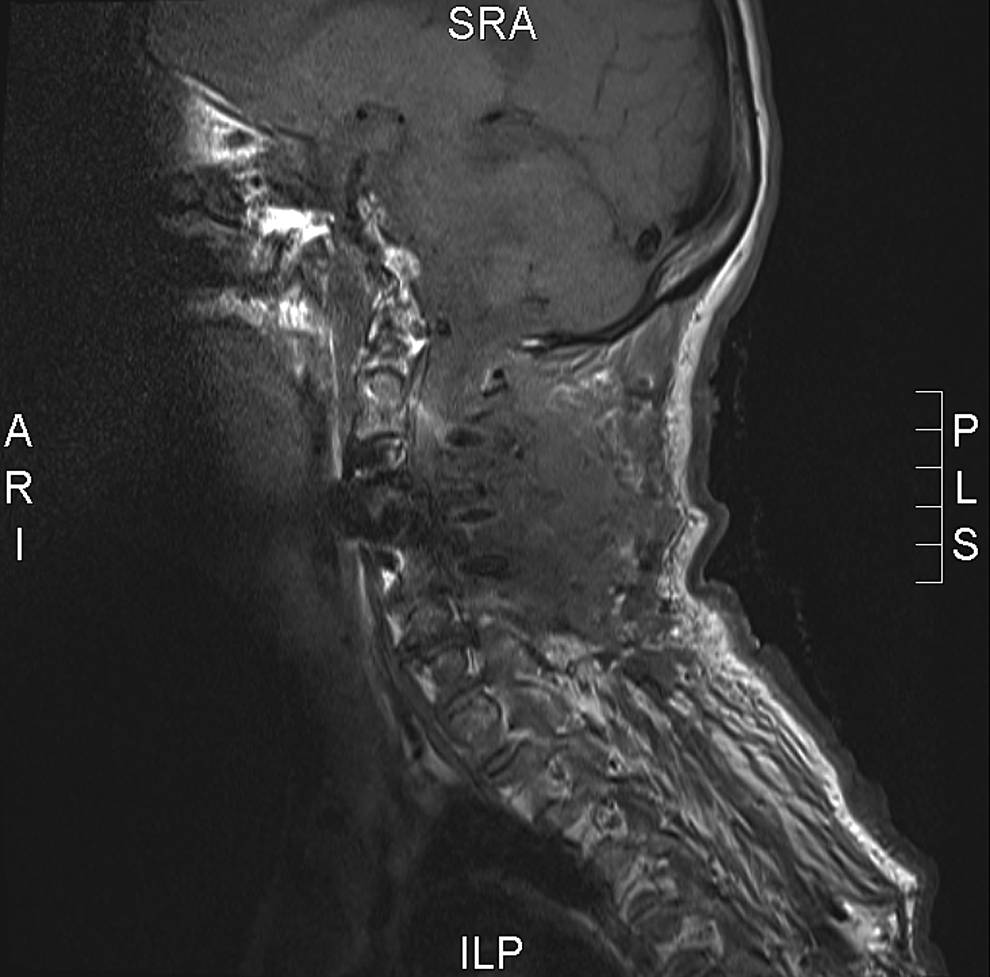
A 60-year-old woman was admitted to the hospital in January 2014 for an elective cervical spine posterior fusion and decompression following the development of progressive cervical myelopathy and central cord syndrome. She had a history of multiple spinal operations at cervical, thoracic, and lumbar levels for degenerative joint disease and scoliosis; many complicated by postoperative surgical wound infections. Perioperatively, she received a once-only dose of intravenous (IV) cefazolin 1 g. Following her procedure, she developed an increasing cervical spine instability and worsening of her central cord syndrome. Postoperative imaging of her neck revealed a large infected hematoma surrounding the operative site, for which she was promptly taken to the operating theatre for debridement and stabilization of her cervical spine (Fig. 1). Microbiology on operative specimens of the cervical wound fluid yielded Staphylococcus epidermidis and multiresistant Enterobacter cloacae. Postwound debridement and washout, the patient was noted to have a rising C-reactive protein (CRP) to 64 mg/L. Following the susceptibility testing on E. cloacae (Table 1), she was commenced on IV vancomycin 1 g and tigecycline 50 mg, both twice daily.
Postoperative cervical wound infection and osteomyelitis due to Staphylococcus epidermidis and Enterobacter cloacae.
AUG, augmentin; TMP, trimethoprim; SXT, sulfamethoxazole; GEN, gentamicin; TOB, tobramycin; AK, amikacin; TIM, timentin; TAZ, tazosin; MER, meropenem; FOS, fosfomycin; TIG, tigecycline; COL, colistin; CIP, ciprofloxacin; ERT, ertapenem; DOR, doripenem; R, resistent; S, sensitive; MIC, minimum inhibitory concentration.
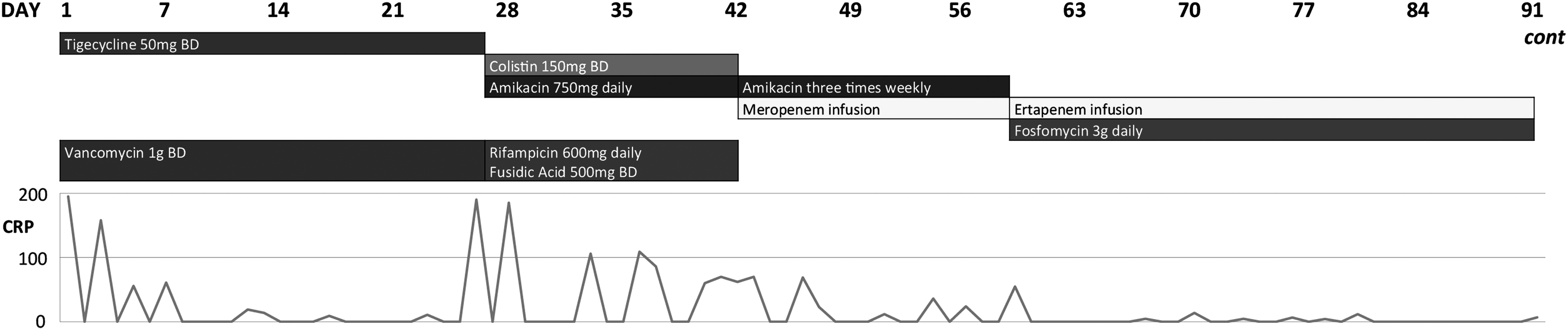
Despite 1 month of antibiotic therapy and multiple washouts of the wound, her symptoms and biochemical markers of inflammation worsened (CRP of 190 mg/L) and repeat imaging showed an inadequate resolution of her wound infection and critical cervical spine instability. This prompted the removal of the infected osteosynthetic material and metalwork, application of an external Mayfield head piece to maintain adequate cervical spine stability, bone grafting, and application of a vacuum dressing to the wound on day 28 of directed antimicrobial therapy. There was a persistence of growth and isolation of carbapenem-resistant E. cloacae with failure to isolate S. epidermidis on subsequent cervical spine washout and debridement. This was deemed to be a failure of antibiotic therapy, and the patient was commenced on a combination of IV amikacin 750 mg daily, IV colistin 150 mg twice daily (i.e., 300 mg of colistin base activity or 10 million IU daily), by mouth (PO) fusidic acid 500 mg twice daily, and PO rifampicin 600 mg daily; with the cessation of tigecycline and vancomycin. The baseline renal function and audiometry were recorded.
The minimum inhibitory concentration (MIC) of amikacin was 4 mg/L on Etest. During an intensive therapy with amikacin and colistin, peak plasma concentrations of amikacin (unbound drug) ranged between 35.0 and 51.9 mg/L, achieving a Cmax/MIC of around 10.
Although a moderate improvement in her wound infection was observed with this regimen, as well as a down-trending CRP to 23 mg/L, the patient experienced a considerable decline in renal function (estimated glomerular filtration rate [eGFR] >90–52 ml/minute/1.73 m2) and detectable sensorineural hearing loss bilaterally. Colistin was ceased and the amikacin dosing and frequency were altered to accommodate her altered renal function. Daily, continuous IV meropenem infusions were commenced in an attempt to provide adequate free drug plasma concentrations above the MIC of 32 mg/L on Etest. A target carbapenem drug concentration above the MIC was sought to ensure fT>MIC was equal to or greater than 40%. However, an increase in the total infused dose of meropenem up to 6 g daily could only achieve a highest steady-state concentration of 29 mg/L, thus failing to provide therapeutic plasma concentrations (Table 2). The length of continuous meropenem infusions ranged from 20 to 24 hours due to drug stability issues. Daily doses of carbapenem were calculated over 24 hours. Unbound meropenem levels were measured 6 hours postdose adjustment, which provided adequate information on steady-state free drug concentrations (meropenem half-life equals 60 minutes in healthy subjects). This therapy extended over a total of 4 weeks and coincided with a downtrending CRP of 36–14 mg/L and an improvement in the clinical status. While on continuous carbapenem-infusion therapy, her renal function was normal (eGFR>90) indicating adequate drug clearance.
Her neck wound was kept open throughout this time and continued to show signs of healing and improved stability despite the compromised antibiotic therapy. The frequency of amikacin dosing was reduced to thrice weekly and eventually ceased, while she was commenced on a continuous IV ertapenem infusion of 2 g daily, with a close monitoring of free drug levels. Unbound plasma ertapenem levels were measured between 4.2 and 10 mg/L (ertapenem MIC of 1 mg/L on Etest) on this therapy. She was stabilized on this parenteral regimen with the addition of oral fosfomycin 3 g (fosfomycin MIC of 2 mg/L), rifampicin 600 mg, and fusidic acid 500 mg twice daily. As her overall condition improved, as well as her neck wound, on day 95 of total antibiotic therapy, her external halo was removed with a successful closure of her neck wound. She was then transferred to a subacute rehabilitation unit where she continued to make gains in her overall function and medical status. Seven months after commencement of IV therapy and 5 months after commencement of ertapenem, her IV antibiotics were ceased due to the healed neck wound and continued suppression of inflammatory markers (CRP<5.0 mg/L). In addition, repeat imaging of her cervical spine revealed the evidence of ossification. One month thereafter, all oral antibiotics were ceased at follow-up with a monthly monitoring of CRP levels, which have remained within normal limits to date (<5.0 mg/L). A timeline of sequential antibiotic therapy and inflammatory markers are illustrated in Figure 2.
Sequential antibiotic therapy.
Discussion
Traditionally, TDM involving antimicrobial therapy has been used for drugs where there is a narrow therapeutic range, known drug toxicity, and a pharmacokinetic profile that is difficult to predict (e.g., aminoglycosides). 6 More recently, studies have emerged demonstrating the widening scope of TDM with a primary focus on maximizing drug efficacy and optimizing antibiotic exposure to improve clinical outcomes. 23 TDM for β-lactam therapy in critically ill patients has revealed favorable results. 21 Roberts et al. demonstrated that dose adjustment was necessary for 74.2% of ICU patients to reach target drug concentrations. 20 In a prospective study examining 50 burn injury patients, a statistically significant shorter duration of antibiotic therapy was described in those patients, which achieved therapeutic targets. 17 A case report of sepsis due to drug-resistant Pseudomonas aeruginosa describes the use of TDM with meropenem to achieve the resolution of infection. 25 Evidence as to whether this is a novel approach to treat an infection in both critically ill and noncritically ill patients requires further elucidation and well-designed, randomized controlled trials. To date, there is no documented use of TDM to guide therapy on invasive carbapenem-resistant Enterobacter infection.
The medical literature regarding treatment of both sensitive and resistant gram-negative osteomyelitis is scant. Our understanding of the best way to treat these uncommon infections remains relatively primitive. 12 Providing an optimal therapy is complicated by the ability to maintain efficacious local drug concentrations within the bone tissue for extended periods of time. 23 Patients often have concurrent illness and comorbidities that further compromise the optimal drug dosing, which aims to achieve target therapeutic drug concentrations at the site of infection. 28 Limited data are available on efficacious antibiotic agents as well as the duration of therapy for gram-negative osteomyelitis. 3 These studies have mainly involved susceptible gram-negative organisms. Animal and healthy subject in vivo studies on the pharmacokinetic profile and osseous tissue penetration of antibiotics with an activity against gram-negative bacteria, including carbapenems, have been recorded.15,23 An elegant study observing ertapenem bone penetration established that the bone tissue/serum ertapenem concentration ratio was 0.1 at 24 hours after injecting 1 g of ertapenem in volunteers who underwent a total hip replacement. 4 The median cancellous and cortical bone tissue concentrations were 13.2 and 8.0 μg/g, respectively, at 1 hour. 4 Knowledge of local infected tissue antibiotic concentrations and MIC of the organism is invaluable in the clinical setting to optimize the dose of antibiotic and achieve a faster resolution of infection. 19 Other important factors to consider when dosing β-lactam antibiotics include changes in the volume of distribution (e.g., third space losses), kidney function (e.g., augmented renal clearance), and adequate blood flow to the infected tissue. 23
There have been several case reports of difficult-to-treat osteomyelitis caused by multiresistant gram-negative bacteria, each with unique treatment failures and successes.2,11 One case of refractory vertebral osteomyelitis has been described due to an extended spectrum β-lactamase (ESBL)-producing Escherichia coli with an apparent treatment failure to ertapenem despite a susceptible MIC on E-testing (0.5 mg/L). 11 In this case the authors describe multiple patient factors (e.g., peripheral vascular disease, bone necrosis) that contributed to therapeutic failure, in addition to suboptimal local antibiotic concentrations. A case of cervical discitis caused by an ESBL-producing Klebsiella pneumoniae successfully treated with IV temocillin has also been reported. 2 Unfortunately, both the antibiotic and susceptibility testing for temocillin are unavailable in Australia.
Although current evidence suggests that colistin, tigecycline, and aminoglycosides are the mainstay of treatment for invasive CRE infections, other therapeutic options have been advocated. 27 An expert opinion has proposed that CRE with carbapenem MICs<4 mg/L can be adequately treated with high-dose prolonged-infusion carbapenem therapy. 5 Meropenem was initially used in this patient despite the relatively high and discordant MICs (Vitek 2: 16 and Etest: 32), for which the cause remains uncertain, although could be due to E-testing having increased the detection of carbapenemase producers with a high-level carbapenem resistance.
Carbapenems exert their antibiotic effect in a time-dependent manner with a bacteriostatic effect being achieved at 20% time above the MIC (fT>MIC) and bactericidal effects observed at 40% fT>MIC. 26 In addition, meropenem has demonstrated beneficial outcomes when the TDM target is set at fT>4−5×MIC. 28 This is particularly useful due to the low toxicity demonstrated by carbapenems, even at high plasma levels. 26 This decreases the rate of suboptimal plasma concentrations and thus, subtherapeutic antibiotic concentrations at the site of infection. In addition, targeting 100% fT>MIC has shown that maximum exposure may be required for a quicker resolution of infection. 23 An increased time above the MIC can be achieved by more frequent, intermittent bolus dosing or by switching to either an extended or continuous infusion. 23 Differences in the clinical outcome or resolution of infection between intermittent dosing versus continuous infusion of β-lactams are yet to be researched. In the setting of resistance and a known carbapenem MIC, a high-dose prolonged infusion with carbapenem levels above the MIC for a minimum of 40% of duration of infusion can provide the effective treatment. 13
In difficult-to-treat infections, the use of multiple antimicrobial agents can provide a therapeutic synergism, reduce the development of resistance, as well as allow a lower dose of toxic agents to be used. 24 Combination therapy appears to be superior to monotherapy for severe infections caused by CRE. 16 Carbapenem containing regimens confer a mortality benefit in observational studies when the MIC<8 mg/L. 14 In addition, high failure rates have been reported with tigecycline monotherapy (as occurred in our patient) mainly due to low serum peak levels. 9 Fosfomycin has satisfactory bone and joint penetration with proven clinical efficacy in osteomyelitis. It has a role in providing adjunctive therapy in CRE infections with a carbapenem MIC>8 mg/L. 10
Currently, there are very few antimicrobials that justify TDM. The characteristics of drugs classically used in TDM include those with a narrow therapeutic index, known toxicity, ill-defined clinical parameters allowing for dose adjustment, known correlation between plasma concentration and efficacy/toxicity, unpredictable relationship between dose and clinical outcome, and difficult-to-predict pharmacokinetics. 23 Antibiotic levels most commonly measured in clinical practice include the aminoglycosides (gentamicin, tobramycin, and amikacin) and vancomycin.7,8 The use of carbapenem drug monitoring in the clinical setting is rarely, if ever, performed. For treatment of invasive CRE infections with continuous carbapenem infusion where fT>MIC is critical for optimal therapy, serum carbapenem levels are able to inform clinical decision-making and ensure an optimal outcome. There remains no literature or guidelines regarding the best practice for TDM in this setting. However, given the increasing number of patients encountered with CRE, a formal investigation of the utility of TDM is warranted. Adverse outcomes have been demonstrated to occur in critically ill hospitalized individuals secondary to inadequate antibiotic exposure warranting a paradigm shift toward an individualized antibiotic dosing. 28
Therapeutically, this was a complex case of multiresistant gram-negative osteomyelitis featuring an apparent treatment failure to tigecycline, drug toxicity secondary to amikacin and colistin, in the context of multiple patient comorbidities. A submaximal dose of tigecycline was used (50 mg twice daily) with the possibility of subtherapeutic drug concentrations given a borderline-high MIC of 0.5 mg/L. 22 In addition, an exceptionally high meropenem MIC of 32 mg/L as well as the initial unavailability of IV fosfomycin provided for difficult and limited therapeutic options. Ultimately, continuous high-dose IV ertapenem infusions with TDM resulted in known serum antibiotic levels above the ertapenem MIC (1 mg/L) for a sufficient amount of time (>40% fT>MIC) as well as also providing for an adequate surrogate marker for osseous tissue penetration. Some degree of uncertainty remains as to whether bone penetration in standard-dose carbapenem therapy is linearly related to high-dose continuous infusion therapy. Ultimately, this atypical treatment strategy led to rapid clinical improvement of the patient's cervical spine stability, wound infection, and osteomyelitis.
Conclusion
The decline in antimicrobial drug development is currently being met by a steady rise in the incidence of infections due to multiresistant bacteria. Previous solutions to this problem have been to import expensive agents from overseas or to rebirth older more toxic agents that can cause harm to an already vulnerable patient population. As our knowledge of the actions of existing antibiotics continues to grow, we are provided with alternate and perhaps more cost-effective means of curing infection.
Carbapenems, like all β-lactams, are time-dependent bactericidal antibiotics. In an isolate with a high carbapenem MIC, monitoring plasma antibiotic levels is able to dictate whether adequate therapy is being given. Carbapenems are a perfect candidate for such therapy as they are easily measured and well tolerated with minimal toxicity, allowing for higher than normal concentrations in ill patients; and a detailed knowledge of its bone and tissue penetration is readily available. To best inform therapeutic decision-making, the optimal frequency of plasma antibiotic level testing is yet to be confirmed. Although there is some evidence for the use of high-dose carbapenem infusion for invasive CRE infections, further investigation is required to demonstrate the effect of TDM on patient outcomes.
Footnotes
Acknowledgments
We thank Dr. Hanna Sidjabat for the genomic sequencing of the IMP-4-producing E. cloacae isolated in this case as well as the research staff at the University of Queensland Centre of Clinical Research (UQCCR) Infection and Immunity Theme.
Disclosure Statement
No competing financial interests exist.