
Abstract
Enterococci are gram-positive cocci responsible for various infections worldwide, and their prevalence of antibiotic resistance greatly varies worldwide. This study investigates the prevalence of resistance to antibiotics in enterococci from patients admitted in the four university hospitals of Marseille between January 2013 and September 2014. Two thousand nine hundred seventy-six patients-bacteria couples were identified (2,507 Enterococcus faecalis and 469 Enterococcus faecium) in the four university hospitals of Marseille. 1.3%, 8.9%, 1.4%, and 0% of E. faecalis strains were resistant to amoxicillin, gentamicin, teicoplanin, and vancomycin, respectively, and 83.9%, 49.2%, 1.3%, and 0.2% of E. faecium strains were resistant to amoxicillin, gentamicin, teicoplanin, and vancomycin, respectively. Resistance to aminoglycosides and vancomycin in strains isolated from blood cultures was significantly lower than that of most European countries included in the 2012 European Antimicrobial Resistance Surveillance Network report. Our low percentage of antibiotic resistance in enterococci is likely due to a low level of E. faecium infections, underlining the need to implement surveillance systems, especially to monitor the E. faecalis/E. faecium ratio evolution in blood cultures and others.
Introduction
E
The prevalence of antibiotic resistance in enterococci varies worldwide. In the United States, before the 1990s, Enterococcus faecalis accounted for 90–95% of the strains collected from patients at the hospital level. 2 Since then, the increasing use of vancomycin and broad-spectrum antimicrobials led to an increase in the prevalence of hospital-acquired infections due to E. faecium, which became almost as prevalent as E. faecalis in hospitals settings, resulting in a dramatic increase in the number of VRE infections in US hospitals between 2000 and 2006. 2 In Europe, the prevalence of VRE collected from invasive infections ranges from 0% in Sweden and the Netherlands to 44% in Ireland according to the 2012 European Antimicrobial Resistance Surveillance Network (EARS-Net) report. 7 At the national level, low outbreaks of VRE hospital-acquired infections occurred in the North of France between 2004 and 2008.6,11–13,22 Nevertheless, no outbreak has ever been reported, to date, in the South of France.
In this context, we herein investigate the prevalence of resistance to antibiotics in enterococci from patients admitted in Marseille university hospitals between January 2013 and September 2014, and compare our results to available data.
Materials and Methods
All the data we analyzed herein came from the four University hospitals of Marseille (North, South, Conception and Timone hospitals). These hospitals include 3,700 beds with ∼1,500 beds for the Timone hospital, 600 beds for the North hospital, 700 beds for the Conception hospital, and 900 beds for the South Hospital. We retrospectively collected raw data of antibiotic susceptibility testing results for amoxicillin, gentamicin, vancomycin, and teicoplanin for E. faecalis and E. faecium strains isolated from January 2013 to September 2014 from the information management system of the four Marseille University hospitals. The enterococci strains analyzed herein were identified using matrix-assisted laser desorption/ionisation time-of-flight (MALDI-TOF) mass spectrometers, 21 which ensure good bacterial identification even for enterococci strains. 8 In our laboratory, we decide to follow the EUCAST recommendations. According to these recommendations, all the antibiotic susceptibility testing results were obtained after using the disk diffusion method. Moreover, E-test for vancomycin must be performed to validate or invalidate possible VRE resistance phenotype. Data were then sorted in a Microsoft Excel database from which duplicates were removed to finally conserve only one bacterial identification per patient. The classification of the infections was done according to the sample from which each enterococci strain was isolated.
Data on the percentage of resistance to gentamicin and vancomycin for E. faecalis and E. faecium strains studied in our study were compared to those available from different European countries included in the EARS-Net report. 7 In this report, only one record per infected patient was conserved, and only data referring to invasive enterococcal bacteremia or meningitis (both community- and hospital-acquired infections) were published.
Statistical analyses were done using Pearson's chi-square test or Fisher's exact test as appropriate using the Epi-Info 3.03 software (www.openepi.com/Menu/OE_Menu.htm). All were two sided, and p-values <0.05 were considered as statistically significant.
Results
Two thousand nine hundred seventy-six patients-bacteria couples were identified throughout the study period, including 2,507 E. faecalis (84.2%) and 469 E. faecium (15.8%), with UTIs being the most common type of clinical isolates (69% and 62% for E. faecalis and E. faecium, respectively) (Fig. 1). 1.3%, 8.9%, 1.4%, and 0% of E. faecalis strains were resistant to amoxicillin, gentamicin, teicoplanin, and vancomycin, respectively. Conversely, 83.9%, 49.2%, 1.3%, and 0.2% of E. faecium strains were resistant to amoxicillin, gentamicin, teicoplanin, and vancomycin, respectively. To be able to compare our resistance level to that of the other European countries included in the EARS-Net report, 7 we divided resistance data from enterococci strains isolated from blood cultures (invasive infections) to that from strains isolated from other infection sites, including urine. The percentage of resistance to all the antibiotics tested in our laboratory of the E. faecalis and E. faecium strains isolated from blood cultures are presented Table 1. Gentamicin resistance was significantly more prevalent in E. faecium strains isolated from blood cultures than in E. faecalis strains isolated from blood cultures (p<10−5). In these enterococci strains, we also observed that the percentage of resistance to aminoglycosides and vancomycin was significantly lower than the percentage of resistance reported in 25 European countries for aminoglycosides and 7 countries for vancomycin (Table 1).
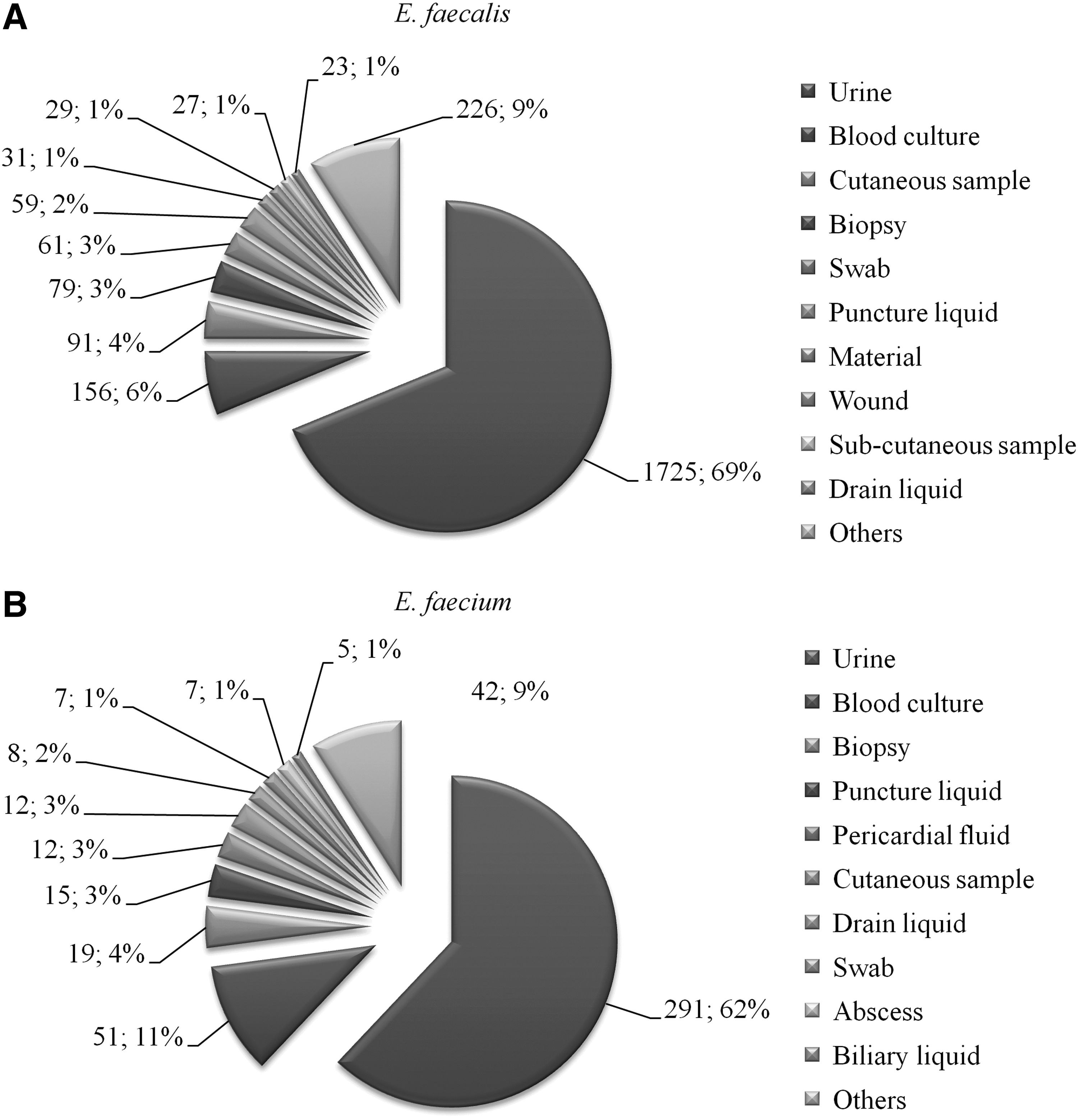
Summary of the 10 main types of sample Enterococcus faecalis
Data from the 2012 European Antimicrobial Resistance Surveillance Network report, www.ecdc.europa.eu/en/publications/Publications/antimicrobial-resistance-surveillance-europe-2012.pdf
NA indicates that the countries did not provide data for the antibiotic and the bacterial species of interest.
Analyses performed using two-sided Pearson chi-square or Fisher exact tests as appropriate, p-value <0.05, comparing the number of E. faecalis or E. faecium strains resistant to gentamicin and vancomycin in our study to that of the different countries presented in the European Antimicrobial Resistance Surveillance Network report.
AMX, amoxicillin; GM, gentamicin; TEC, teicoplanin; VA, vancomycin.
Discussion
It is well known that E. faecium strains have an extraordinary genome plasticity, allowing them to be more frequently resistant than E. faecalis strains.2,4 In the US, the increase in the number of E. faecium strains isolated from patients led to an increase in the isolation of VRE from 0% in the 1980s to 80% in 2007 and currently, the prevalence of nosocomial infections due to E. faecium species is almost the same as E. faecalis. 2 Similar observations were made in France where the ratio E. faecium/E. faecalis infections increased from 10%/90% at the end of the 1990s to 27%/73% in 2010, leading to an increase in the resistance of enterococci strains isolated from hospitalized patients. 4 The French national reference center for antibiotic resistance observed that more than 95% of the VRE received nationwide were E. faecium strains from 2006 to 2013 (www cnr-resistance-antibiotiquesfr/bilans-dactivites html) and mainly those included in the clonal complex 17 (CC17), a clade of strains that is pandemic and associated with hospital-acquired E. faecium infections. 9 The common capability of the CC17 strains to colonize and harbor resistance genes was directly involved in the increase of isolation of E. faecium strains in hospitalized patients in US and European hospitals.2,4,7
In Europe, avoparcin, a glycopeptide antibiotic used to promote food-producing animals growth in agriculture,4,10 was suspected to select for VRE gut carriage 25 and was banned for animal husbandry in 1996.2,4 Several years after, studies demonstrated that the number of VRE declined in food-producing animals, including chicken and pigs in Denmark and France, 4 likely explaining the lower prevalence of VRE in Europe as compared to the US. Nevertheless, numerous European studies identified E. faecium VRE colonization in nonwild animals, including buzzards, 18 migratory wild birds, 23 and mullets fish, 1 supporting the possible role of wild animals as VRE reservoir.
Our results also allowed us to observe that the percentage of resistance to gentamicin in E. faecium strains isolated from blood cultures was significantly higher compared to E. faecalis strains (Table 1). This was also observed in a 2006–2009 Danish population-based cohort study, 16 in Australia in 2010, 5 and in Greece. 17 High-level gentamicin resistance gene aac(6′)-Ie-aph(2″) (aacA-aphD) is usually located on Tn4001-type transposons, which can be carried by highly transferable plasmids19,20 among E. faecium strains reported in Greece and Australia.5,17
Interestingly, whole genome sequencing of the major clones of E. faecium causing outbreaks has shown that the presence of clustered regularly interspaced short palindromic repeats elements, small DNA elements that protect bacteria against the acquisition of foreign DNA, was inversely correlated with the presence of resistant genes in most multidrug-resistant enterococci clonal isolates, especially in the hospital-adapted CC17 E. faecium strains. 15 This finding shows that the acquired resistance is not established and that bacteria may eliminate foreign DNA when it did not confer a useful phenotype. It also shows that the resistance level may not be cumulative, but results from epidemic clones favored by environmental factors.
Our study suffered from a major limitation; the fact that we did not perform any molecular analyses to check if our strains, especially the E. faecium strains, belonged to a special clonal complex like the CC17. We believe that such molecular analyses should be performed in our region in a future molecular epidemiological study based on human and animal samples.
In conclusion, our low level of antibiotic resistance in enterococci is likely due to a low level of E. faecium infections, maybe due to a regional low animal carriage of this bacterial species.
These observations underlined the need to implement integrated surveillance systems to quickly identify resistant clone outbreaks, survey the CC17 incidence, and to monitor the E. faecalis/E. faecium ratio evolution.
Footnotes
Acknowledgments
This work was partly funded by the Centre National de la Recherche Scientifique and the Institut Hospitalo-Universitaire Méditerranée Infection.
Disclosure Statement
There are no conflicts of interest for all authors.