
Abstract
The lack of treatment for multidrug-resistant (MDR) Enterobacteriaceae often leads to the use of double or triple antibiotic combinations to increase the option of clinical success. This study analyzes multiple combination bactericidal testing (MCBT) to screen double and triple antibiotic combinations, at standard peak serum concentration, for bactericidal activity against 21 MDR Klebsiella pneumoniae isolates. This method was compared with time–killing curves. The full bactericidal activity against all strains was obtained only by adding colistin. MCBT has a potential to become a rapid method for testing multiple antibiotic combinations for MDR microorganisms when colistin is used, providing clinicians with in vitro cidal data within 48 hr of strain isolation.
Introduction
M
There are multiple methodologies for synergy testing: among them checkerboard and time–killing (TK) curves are the most used even if time-consuming and labor-intensive 24 and multiple combination bactericidal testing (MCBT) have been used most often for cystic fibrosis isolates. 2 MCBT combines two or three drugs in microtiter wells and is relatively easy to perform in clinical microbiology laboratories.
In this study we report the use of an MCBT, which screens double and triple antibiotic combinations at peak serum level, comparing it with the TK method used as a reference.
Materials and Methods
Twenty-one well-characterized K. pneumoniae strains were used in this study. All strains were MDR or extensively drug-resistant clones, possessing different mechanisms of carbapenem resistance including, n.2 VIM-1, n.2 OXA-48, and n.17 K. pneumoniae carbapenemase (KPC)-producing K. pneumoniae strains belonging to STs 258, 512, 101, and 307.12,19 The strains were also selected on the basis of colistin resistance (12 out 21).
The following antibiotics were used in double and triple combinations for MCBT and the antibiotic concentrations were chosen on the basis of peak serum levels after standard intravenous administration: meropenem (120 mg/L) + ertapenem (70 mg/L) and/or with colistin sulfate (Sigma Chemical, St. Louis, MO) (20 mg/L); rifampin (6 mg/L) + tigecycline (0.9 mg/L) and/or with colistin (20 mg/L); and rifampin (6 mg/L) + colistin (20 mg/L).4,7,22,27,28 For the same antibiotics, minimum inhibitory concentrations (MICs) were determined by microdilution in cation-adjusted Mueller-Hinton broth as recommended by CLSI 2012 6 and results were interpreted according to EUCAST 2014 data. 8
MCBT procedures were performed in triplicate according to previously published methods. 1 Plates were incubated at 35°C for 24 hr and wells were examined for turbidity. The contents of nonturbid wells at 24 hr were subcultured by streaking 10 μl of suspension onto a Mueller-Hinton cation-adjusted agar plate, which was then incubated for 24 hr at 35°C and examined for 99.9% kill the next day (bactericidal activity).
The single antibiotics and combinations were also evaluated by TK curves, at the same MCBT concentrations, following standard methods. Bactericidal activity of single antibiotic was defined as a ≥3 log10 CFU/ml reduction of initial inoculum after 24 hr of incubation. Synergy was defined as a decrease of ≥2 log10 CFU/ml between the combination and the most active single agent at 24 hr. 4
Results
In this work we examined 21 MDR K. pneumoniae strains, most of them resistant to carbapenems, with the exception of the 1 OXA-48-producing K. pneumoniae strain, showing reduced susceptibility to meropenem, and both VIM-1 K. pneumoniae strains, susceptible to ertapenem, meropenem, and colistin. The MIC of rifampin ranged from 16 to 32 mg/L. Twelve out of 21 isolates were resistant to colistin (MIC range 4–32 mg/L) and most of all strains were susceptible to tigecycline (MIC range 0.03–1 mg/L). The results of the TK curves, expressed as difference between the initial inoculum and the number of residual viable colonies (CFU/ml) at 24 hr for each antibiotic, are shown in Table 1.
Positive values indicate increase of growth.
Negative values indicate reduction of growth.
MIC, minimum inhibitory concentration; KPC, K. pneumoniae carbapenemase.
In time-killing analysis, neither tigecycline nor rifampin were cidal against all the studied MDR K. pneumoniae strains at peak serum concentration even for those strains that have peak serum values higher than MIC values. It is noteworthy that the activity of other antibiotics (ertapenem, meropenem, and colistin) was not bactericidal against some strains, although their peak serum concentration was higher than MIC values. The synergistic activity of various combinations tested and the agreement results between both methods are shown in Fig. 1. In the various combinations used, the double carbapenem combination was synergic for 9/21 strains on TK; full bactericidal activity against all strains was obtained only by adding colistin. The same was true for tigecycline+rifampin, cidal only against both VIM-1 K. pneumoniae strains: the addition of colistin rendered the combination strongly bactericidal. The rifampin+colistin combination was cidal against all strains with both methods. In all cases, adding colistin enhanced the effect of the double antibiotic combinations.
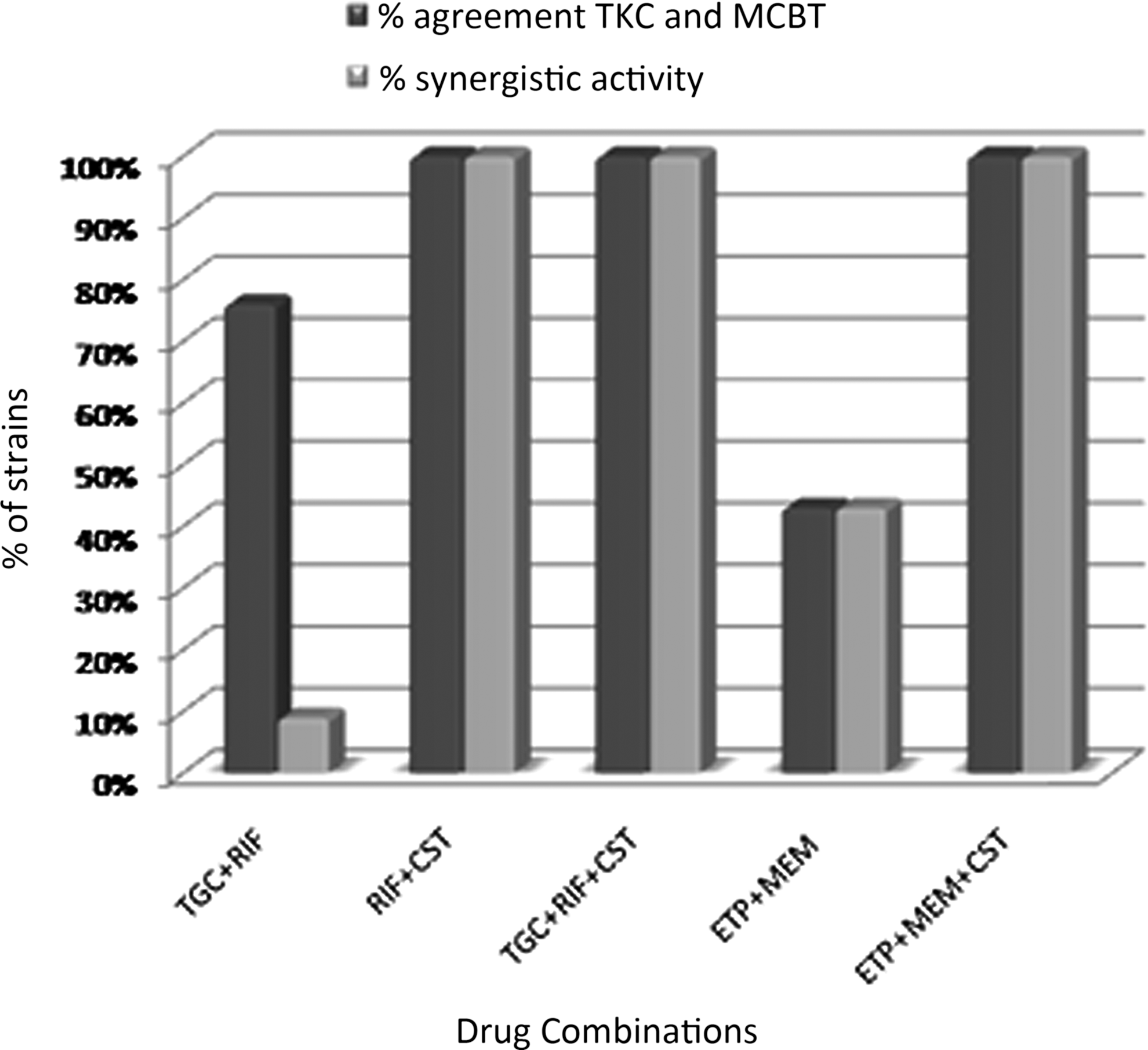
Agreement between time–killing and MCBT methods; synergistic activity of double and triple combinations against 21 Klebsiella pneumoniae. CST, colistin; ETP, ertapenem; MCBT, multiple combination bactericidal testing; MEM, meropenem; RIF, rifampin; TGC, tigecycline; TKC, TK curves.
All strains were tested by TK curves and MCBT. In all isolates the reference TK method revealed a high agreement of 100% with MCBT for rifampin+colistin, tigecycline+rifampin+colistin, and ertapenem+meropenem+colistin.
Of the 21 MDR K. pneumoniae strains, there was only a 43% concordance for ertapenem+meropenem whereas the MCBT and TK results agreed in 16 of the 21 isolates for tigecycline+rifampin. The best agreements were with combinations that included colistin.
Results of our study suggest that (1) MCBT is an easy and realistic method to study in vitro activity of combination therapies by using standard serum concentration of antibiotics, providing clinicians with in vitro cidal data within 48–72 hr of strain isolation; (2) MCBT can be used in place of TK curves because these methods showed the same discriminatory power and reproducibility (Fig. 1); (3) adding colistin as a third antibiotic to a nonbactericidal double-drug combination increased the likelihood of bactericidal effects; (4) these combinations combined with colistin are bactericidal in strains with a complex profile of resistance, including the same antibiotics combined.
Conclusions
Severe MDR infections are an increasing problem, and in areas where MDR microorganisms are endemic, the use of combination therapy with colistin has been an option in the treatment of serious infections.11,14 However, evaluation of in vitro susceptibility testing methods for colistin has shown testing errors with various methods.9,13,16 EUCAST recommends testing colistin with an MIC method with respect to the disk diffusion method. 8 In agreement with results recently published, the broth microdilution method is considered more sensitive with respect to the gradient test.9,16,18
Due to the limited options for the treatment of MDR K. pneumoniae, we report on the in vitro activity of the colistin combined with the most used drugs, showing improved antibacterial activity as demonstrated by different authors20,25 in an attempt to assess synergy among two and three antibiotics using a simple and reproducible method and to compare the agreement between MCBT and TK curves using 21 clinical isolates of MDR K. pneumoniae.
Numerous methods used to detect in vitro synergy between antibiotics have been described: the gradient test and recently the two-dimensional gradient technique.3,26 Both are relatively easy tests to routinely perform in the clinical microbiology laboratory.
Methodologically, MCBT is a rapid method requiring 48 hr to give results to the clinician, it is an easy method to use, requiring nonexpensive resources, and is easily performed in the laboratory. On the basis of our results, the MCBT method appears to be a possible alternative to TK curves because, using the peak serum concentration, we obtained the results in half the time with respect to TK curves.
In this context, our model appears robust at identifying a promising combination for the treatment of MDR KPC-producing isolates.
Because only a modest number of isolates were included in this study, it will be necessary to perform further MCBT studies for the other antibiotic combinations against MDR microorganisms. Therefore, the future direction of our work will aim to determine the possible veracity of this technique by developing other antibiotic associations.
In conclusion, the performance of MCBT is reliable when colistin is used in triple combinations against carbapenem-resistant strains both susceptible and resistant to colistin.
Footnotes
Acknowledgment
The authors express their gratitude to Scientific Bureau of the University of Catania for language support.
This work was supported by PON funding no. 01_02589.
Disclosure Statement
No competing financial interests exist.